


Abstract
3040
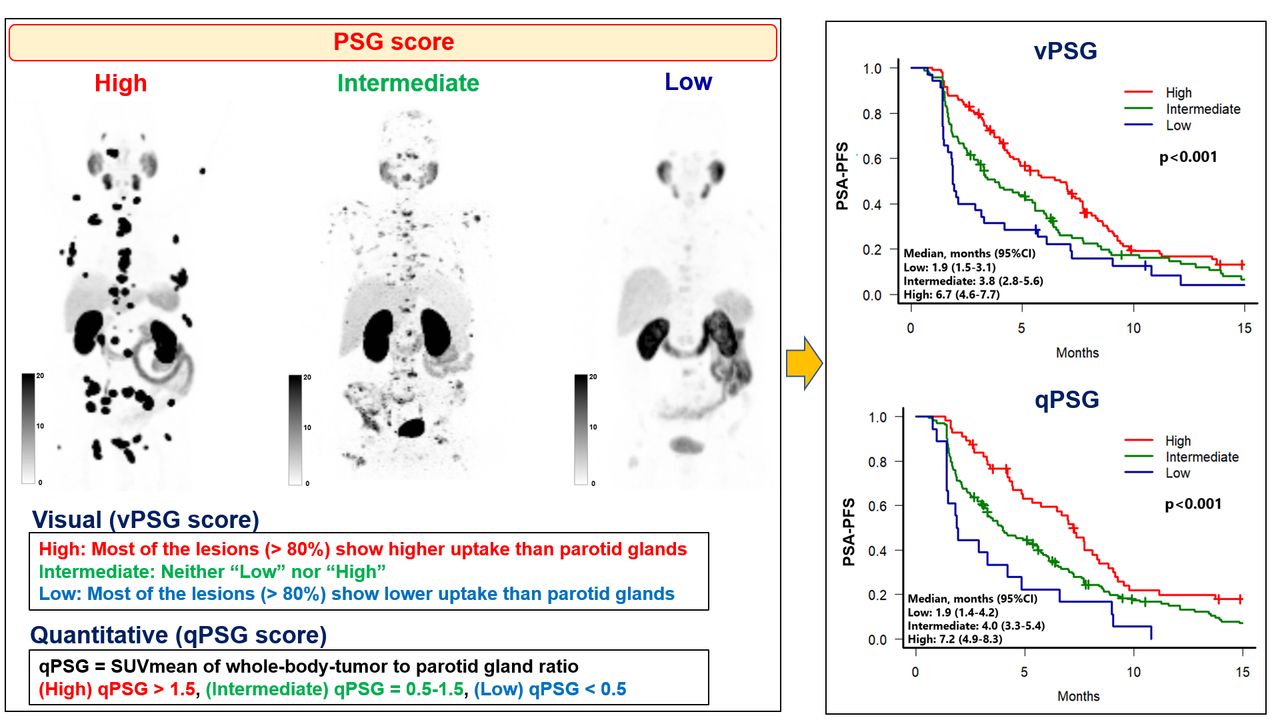
Introduction: PSMA-targeted Radioligand therapy (RLT) can prolong survival and improve the quality of life of patients with advanced metastatic castration-resistant prostate cancer (mCRPC). However, patients do not respond uniformly and a PSA decline of ≥50% (PSA50) was achieved only in 46% of the patients in the VISION trial. We hypothesized that using the parotid glands instead of the liver as the reference organ to evaluate the tumor PSMA uptake would enable more selective stratification of patients prior to Lu-177 PSMA therapy. The aim of this study was to test pre-defined quantitative and visual criteria using the parotid glands as a reference organ to predict outcomes after Lu-177 PSMA therapy in patients with mCRPC
Methods: This was an international multicenter retrospective study conducted in an established dataset from a prior published cohort of 270 patients with mCRPC treated with Lu-177 PSMA RLT (Gafita A, Lancet Oncol 2021). In a first step, we assessed quantitatively (qPSG score) the PSMA tumor-to-salivary-gland ratio of the whole-body tumor burden (qPSG = SUVmean whole-body-tumor/ SUVmean parotid glands) using a semi-automatic segmentation software (qPSMA). Patients were divided into three groups: high (qPSG > 1.5), intermediate (qPSG = 0.5 - 1.5) and low (qPSG < 0.5). In a second step, we assessed the reproducibility and the predictive value of the PSG score graded visually (vPSG score) by 10 blinded independent readers with the experience (> 2 years) in PSMA PET reading. Each reader was blinded to patients' outcomes and read independently the baseline PSMA PET 3D maximum intensity projection (MIP) images of each patient. The readers classified the patients into three groups: (high) most of the lesions (> 80%) show higher uptake than parotid glands; (intermediate) neither “low” nor “high”; (low) most of the lesions (> 80%) show lower uptake than parotid glands. In case of inter-reader disagreement, a majority rule was used. If disagreement “intermediate vs high” or “low vs intermediate” persisted (e.g., 5 vs 5), the cases were classified as high or low, respectively, avoiding intermediate category. The Fleiss’ and Cohen's weighted Kappa statistics were used for the assessment of inter- and intra-reader reproducibility, respectively. Outcome measures included PSA-progression free-survival (PSA-PFS), overall survival (OS), and PSA50. The Fisher’s exact test and Kaplan–Meier analysis with the log-rank test was performed for PSA50 and survival analysis, respectively.
Results: 237 men were analyzed after excluding 33 men with more than half of the parotid glands out of the PET scan field-of-view. The number of the patients in the high, intermediate, and low groups were 56/237 (23.6%), 163 (68.8%), and 18 (7.6%) for qPSG score, and 106/237 (44.7%), 96 (40.5%), and 35 (14.8%) for vPSG score, respectively. The inter- and intra-readers reproducibility of the vPSG score showed substantial (Fleiss’ weighted Kappa: 0.68) and almost perfect (Cohen's weighted Kappa (mean): 0.83) agreement, respectively. The median PSA-PFS of high, intermediate, and low groups were 7.2, 4.0, and 1.9 months (p < 0.001) for qPSG score and 6.7, 3.8, and 1.9 months (p < 0.001) for vPSG score, respectively. Higher PSA50 rate was observed in the high group followed by the intermediate and low groups (high vs intermediate vs low: [qPSG] 69.6% vs 38.7% vs 16.7%; [vPSG] 63.2% vs 33.3% vs 16.1%). OS was longer in the high group than in the intermediate + low (i.e., non-high) group by qPSG score (15.0 vs. 11.7 months (p = 0.013)) and vPSG score (14.3 vs.11.0 months (p = 0.038)).
Conclusions: The PSG score assessed visually or quantitatively is a valuable predictive biomarker for response in men with mCRPC treated with Lu-177 PSMA RLT. The visual criteria (vPSG score) yielded substantial reproducibility and comparable predictive value to the quantitative analysis (qPSG score). Although prospective validation is warranted, the PSG score may assist individual decision-making and clinical trial design.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.