


Abstract
2624
Introduction: Prostate-specific membrane antigen (PSMA) is overexpressed on 95% of prostate cancers and has become a critical biomarker for targeted imaging with positron emission tomography (PET) agents. [18F]-DCFPyL, an FDA approved PSMA-based PET agent, has demonstrated superiority for early metastatic prostate cancer detection [1]. However, a pitfall of PSMA-PET is the presence of indeterminate PSMA uptake in soft tissue and bone lesions [2,3]. Since metastatic prostate cancer commonly involves bones, indeterminate bone lesions (IBLs) that are truly benign entities could be easily mistaken for bone metastases, leading to unnecessary biopsy and overtreatment of patients with life-changing interventions. Therefore, it is imperative to understand and interpret IBLs with high accuracy. Herein, we aim to define variables based on PSMA-PET imaging findings that predict the clinical outcome of IBLs.
Methods: [18F]-DCFPyL PET/CT imaging was performed in 244 consecutive biochemically recurrent (BCR) and high-risk primary disease patients with histologically confirmed prostate cancer and without prior evidence of metastatic disease at CT and bone scan. Patients included in the analysis had at least one IBL identified by [18F]-DCFPyL with or without the presence of other definitive metastatic bone or lymph node lesions. Each IBL was interpreted by 2 readers using follow-up imaging and guided biopsy (when available), and was defined as benign, malignant, or equivocal. Patient variables (age, Gleason Grade, TNM stage, PSA), lesion variables (location [spine, pelvis, rib, other], SUVmax) and scan variables (presence of positive lymph nodes, local findings in the prostate/prostate bed, other indeterminate or definite bone lesions suspicious of metastatic disease) were noted. Statistical testing included Pearson’s chi-square tests for categorical variables, Wilcoxon rank sum tests for continuous variables, and logistic regression analysis. Statistical analysis was performed accounting for the clustered nature of lesion data on the patient-level.
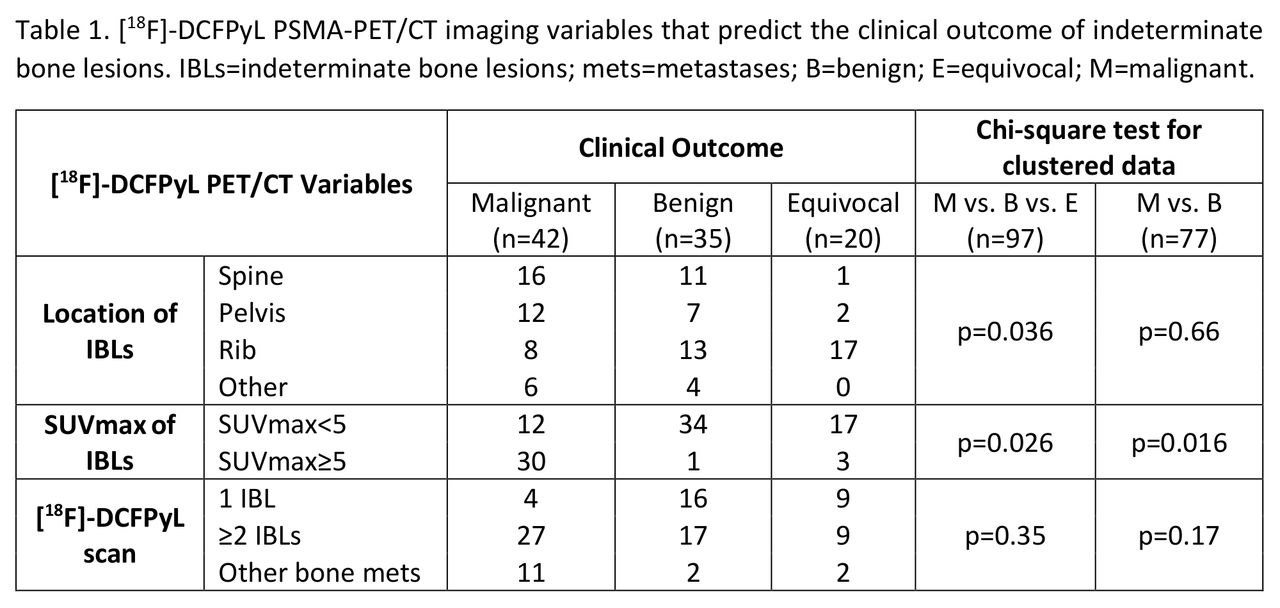
Results: Of the 244 patients that underwent [18F]-DCFPyL imaging, 97 IBLs were identified in 47 patients. After prospective or retrospective interpretation of each IBL, 42 were considered as malignant, 35 were benign, and 20 had equivocal findings. With few exceptions, IBLs that were interpreted as equivocal resulted from no patient follow-up or insufficient imaging information to make a definitive decision. Lesion location (chi-square p=0.036) and SUVmax (chi-square p=0.026) were categorically predictive variables of IBL clinical outcome, including equivocal lesions (Table 1). 41 of the 42 IBLs (97.6%) interpreted as malignant were found in the pelvis or spine, had SUVmax≥5, or had other definite bone metastases noted at [18F]-DCFPyL scans. 34 of the 35 IBLs (97.1%) with benign interpretation were present in the ribs or had SUVmax<5. Similar to IBLs with benign findings, 19 of the 20 IBLs (95.0%) with equivocal interpretation were located in the ribs or had SUVmax<5. Logistic regression revealed that SUVmax (OR=2.21, p=0.002) and the presence of other typical metastatic bone lesions in the scan (OR=2.23, p=0.014) were significant predictors of clinical outcome.
Conclusions: In this BCR and high-risk prostate cancer patient cohort, lesion location, lesion SUVmax, and the presence of additional typical bone metastases are significant predictive variables for determining the clinical outcome of IBLs at [18F]-DCFPyL PET/CT imaging. Although different PSMA-PET radiotracers require specific decisions for a particular scan, radiologists could utilize these predictive variables when interpreting [18F]-DCFPyL PET/CT images to guide their decision-making for IBLs. However, correlating imaging findings with patient history can be necessary before defining IBLs as benign findings or pursuing additional interventions for further interrogation to depict metastatic disease.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.