


Abstract
2538
Introduction: In the setting of biochemical recurrence (BCR) of prostate cancer (PCa), salvage radiation therapy (SRT) can be a curative approach. SRT is conducted following contouring guidelines based on expert consensus, such as the Radiation Therapy Oncology Group (RTOG) guidelines, that are not derived from patient’s anatomic patterns of recurrence. The aim of this study was to analyze the typical patterns of recurrence from PCa in the prostate fossa (PF) in patients experiencing BCR after radical prostatectomy using 68Ga-PSMA-11 PET/CT (PSMA PET) and evaluate the correlation between the clinical target volumes (CTVs) delineated using the RTOG contouring guidelines and PSMA PET recurrence in the PF.
Methods: Patients with PCa experiencing BCR post radical prostatectomy were retrospectively included in the analysis if their PSMA PET showed recurrence in the PF. Two nuclear medicine physicians manually delineated the PF recurrence on the CT images of the PSMA PET/CT and documented the location of the recurrence. Four radiation oncologists, masked to the PSMA PET component of the PET/CT study and the PSMA-based lesions delineations, contoured the CTVs on the same CT using the RTOG contouring guidelines. 3-dimensional heat maps of the PSMA PET-positive PF lesions were obtained to visually depict the typical patterns of PSMA PET recurrences. The coverage of the PSMA PET recurrence by the RTOG-based CTV was categorized as follows: PSMA recurrence fully within, fully outside or partly covered by the CTV. Further, we evaluated the differences in PSMA recurrence patterns among patients with PF limited disease (miTrN0M0), pelvic nodal (miN1) or distal nodal and/or distant metastatic disease (miM1).
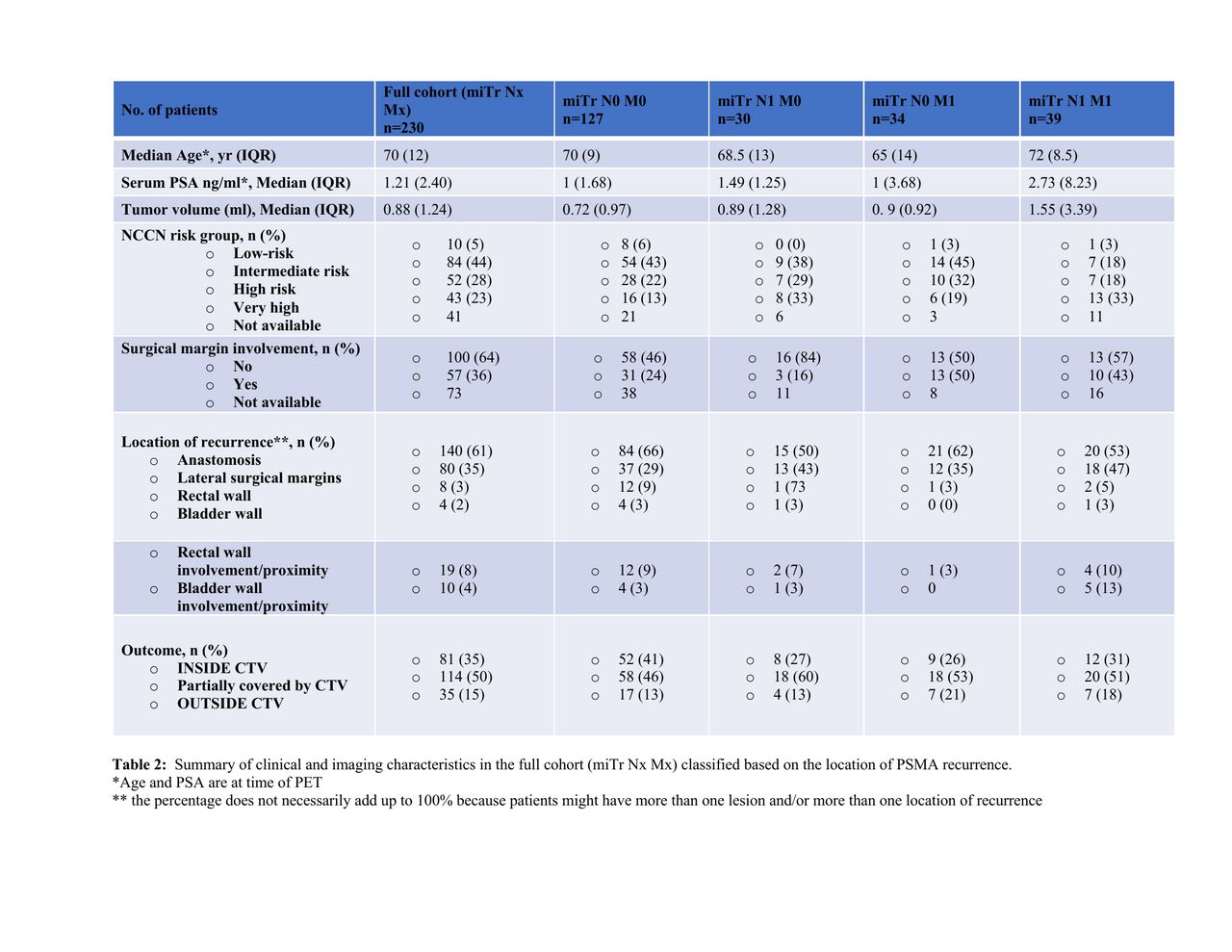
Results: 2,415 PSMA PET scans done at UCLA between 11/2016 and 11/2020 were screened for inclusion criteria. 230/2415 (10%) patients with PF recurrence on PSMA PET were included in the analysis. 127 patients had PSMA recurrence limited to the PF (miTrN0M0), 30 had PSMA PET disease spread to the pelvic nodes only (miTrN1M0), 34 to the distant organs and/or extra-pelvic nodes only (miTrN0M1), and 39 to both pelvic nodes and distant organs/extra-pelvic nodes (miTrN1M1).
In the miTrN0M0 cohort, the PSMA-positive PF recurrences was fully covered by the CTV in 52/127 (41%) patients, partly covered in 58/127 (46%) patients, and fully outside in 17/127 (13%) patients. In the latter group, the location of the recurrence was in the central aspects of the surgical anastomosis in 14/17 (82%) cases, lateral aspect of the anastomosis/seminal vesicle bed in 1/17 (6%) and rectal wall in 2/17 (12%). The lesion involved or was in close proximity to the rectal wall in 6/17 (35%). Overall, the recurrence was centrally, laterally located, in the rectal or bladder wall in 84/127 (66%), 37/127 (29%), 4/127 (4%) and 3/127 (2%), respectively. It involved or was in close proximity to the rectal and bladder wall in 12/127 (9%) and 4/127 (3%), respectively.
The median (IQR) serum PSA levels were 1,11 (1.57), 1.10 (2.14) and 0.79 (0.58), and the volumes of PSMA PET recurrences were 0.57 (0.76), 1 (1.51) and 0.55 (0.58) in patients with PSMA recurrences fully within, partially covered and fully outside the CTV, respectively.
Conclusions: Our study showed that in patients experiencing BCR post-RP with disease limited to the PF (miTrN0M0), the RTOG contouring guidelines for SRT cover the full extent of the disease in 41% of the patients. In 46% of the cases the recurrence is only partly covered and in 13% this is located fully outside the CTV. Our study suggests that PSMA PET can be an invaluable tool for SRT planning in the setting of BCR for patients with disease limited to the PF, and should be incorporated in the definition of the RT contouring guidelines.





In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.