


Abstract
2487
Introduction: Ovarian cancer is common and deadly. Inhibitors of Poly-(ADP ribose) polymerase 1 (PARP), an enzyme involved in cellular recognition and repair of damaged DNA, have improved treatment options, but clinical response is heterogeneous. Guidelines recommend BRCA1 testing prior to PARPi therapy, but patients without BRCA1 germline mutation may respond. A rapid, non-invasive test of tumoral PARP expression prior to therapy that could be repeated to measure PARP inhibitor (PARPi) drug engagement during treatment remains an unmet clinical need. Our group has developed a PARPi PET tracer, 18F Fluorthanatrace (18F FTT). Uptake of this tracer has been shown to correlate with the expression of PARP-1 in both mouse and patient studies and is reliably blocked by PARPi therapy. This study further evaluates the clinical performance of 18F FTT PET in comparison to 18F FDG PET.
Methods: Patients with known or suspected ovarian, fallopian, and peritoneal tumors were enrolled on a prospective clinical trial of 18F FTTPET/CT imaging. Patients underwent 18F FTTPET/CT imaging in either a biodistribution or dynamic imaging protocol. Within 4 weeks, standard-of-care 18F FDG PET/CT scans were also performed. All PET/CT images were reviewed by a board-certified nuclear medicine physician and a third-year radiology resident. Up to 6 lesions per patient were included. SUVmax was calculated semi-automatically using MIM software. 18F FDG and 18F FTT uptake were compared using a best fit line and coefficient of determination. Additional sub-group analysis was also performed. Medical records were reviewed to obtain pathologic and germline/somatic mutation status and to identify a clinical example in which a patient underwent 18F FTT and 18F FDG PET/CT before and after PARPi therapy.
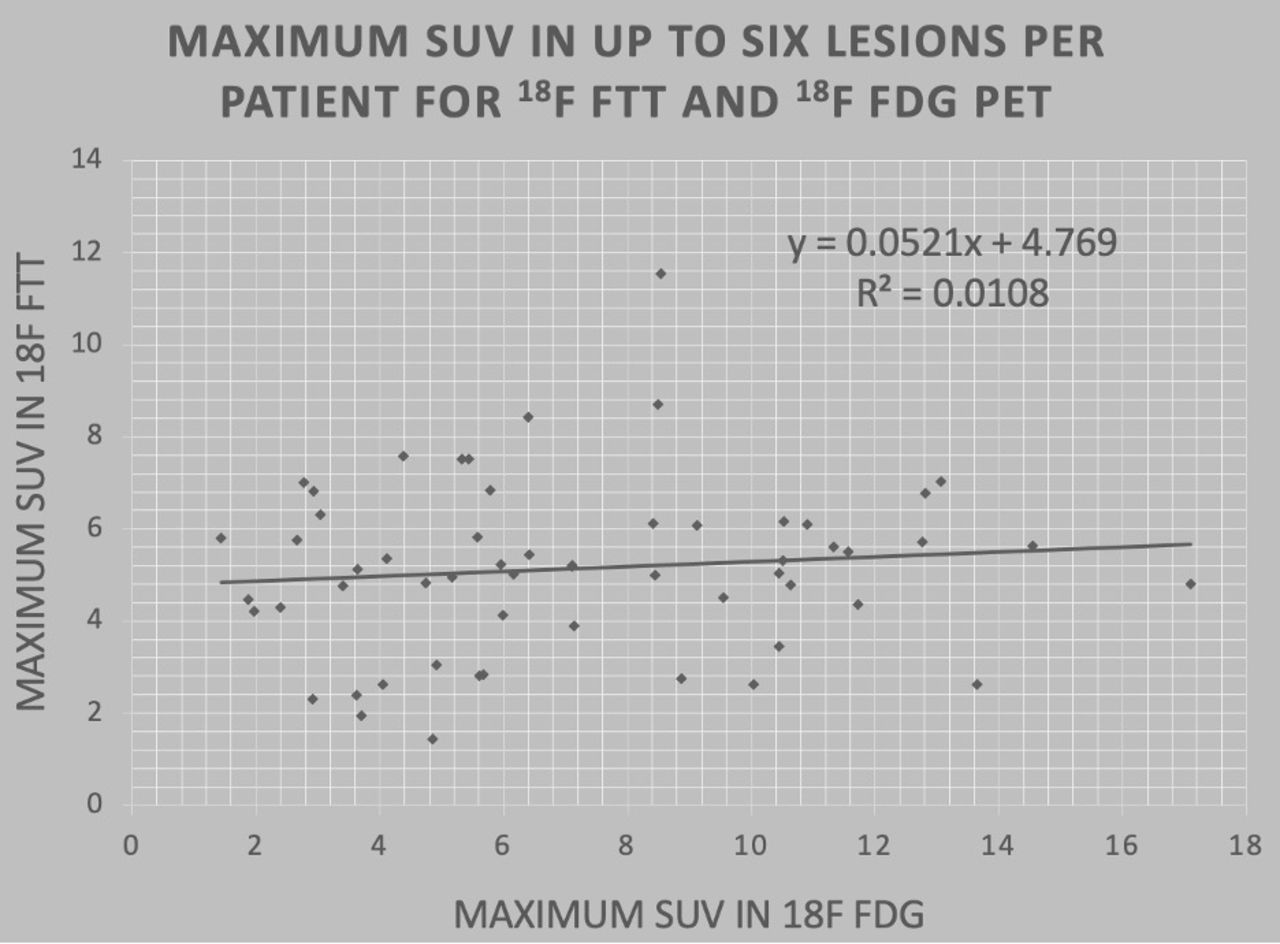
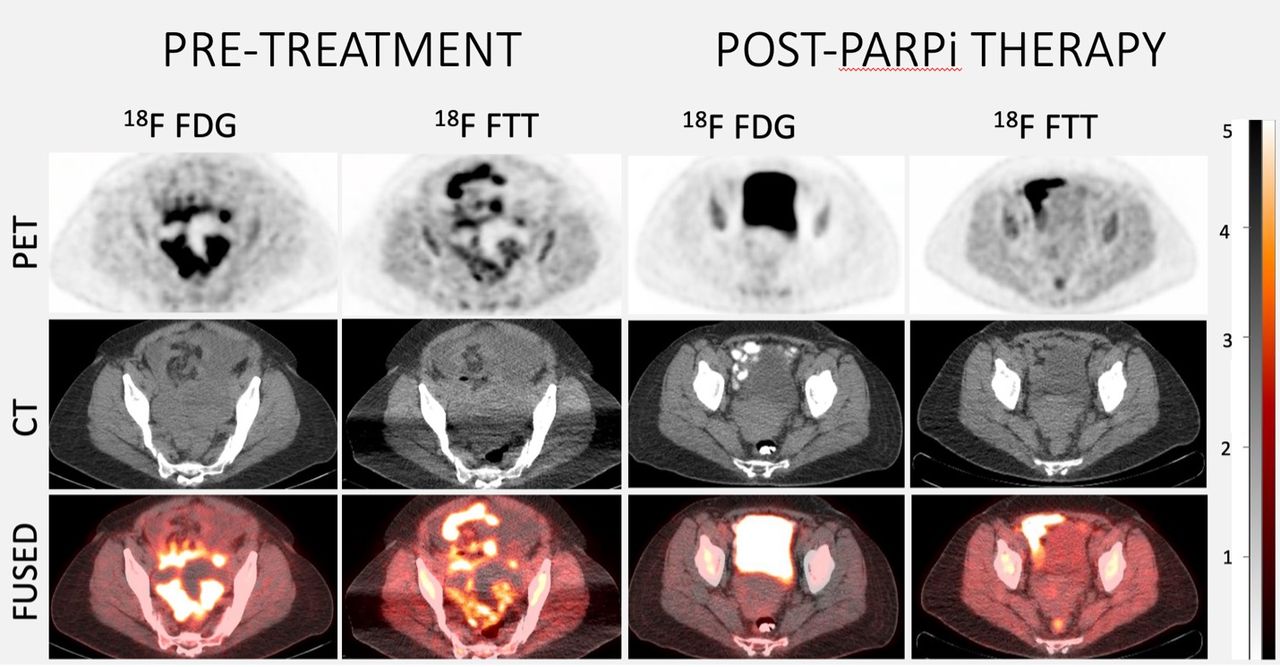
Results: A total of 20 subjects were enrolled in the single-center trial. Two subjects were unable to schedule their PET imaging prior to definitive surgery and were excluded. Two patients underwent imaging, but had no radiotracer uptake on 18F FTT or 18F FDG PET. The SUVmax ranged from 1.4 to 11.6 for the 18F FTT PET and from 1.4 to 17.1 for the 18F FDG PET. There was no correlation between SUVmax for 18F FTT and 18F FDG PET/CT (R2= 0.011, p = 0.44.) On subgroup analysis, the average SUVmax was 5.5 (SD 1.9) for high-grade ovarian cancers, 6.4 (SD 1.2) for germline BRCA1 mutation, 5.7 (SD 1.8) for BRCA-ness qualities, and 4.7 (SD 1.6) in non-high grade/non-BRCA patients. There was significant overlap in range of 18F FTT PET uptake across these groups. During normal clinical management, one patient received 3 months of chemo- and PARPi therapy (carboplatin-taxol and veliparib) between initial and follow up 18F FTT and FDG PET/CT scans. This patient had a somatic BRCA 1 mutation and high-grade serous carcinoma of the bilateral ovaries and fallopian tubes. Her post PARPi therapy 18F FTT PET/CT scan showed complete tumor blocking. Her post PARPi therapy 18F FDG PET/CT showed a complete metabolic response.
Conclusions: 18F FTT and 18F FDG uptake was identified in all anatomically visible tumors. There was no correlation between 18F FTT and 18F FDG uptake, reflecting their unique molecular targets. There was a positive trend with wide range and significant overlap of 18F FTT uptake in patients with high grade ovarian cancers, BRCA 1 germline mutation, BRCA-ness qualities, and in patients without genetic or histologic pre-determinants of PARP1 expression. This highlights the limitations of genetic and histologic predictors of PARP1 expression. A clinical example showed high PARP expression in a patient who received veliparib in the interim between initial and repeat 18F FTT PET imaging and demonstrated complete tumor blocking on repeated 18F FTT PET and a complete metabolic response on repeated 18F FDG PET. These findings support the further investigation of 18F FTT to characterize ovarian tumor PARP expression in order to guide therapeutic decisions for patients receiving PARPi in the future.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.