


Abstract
2297
Introduction: The complex interactions and the balance between inflammation and fibrosis play a crucial role in cardiac repair after acute myocardial infarction(AMI). Cardiac inflammation and fibroblast activation could be evaluated by 18F-fluorodeoxyglucose (FDG) and radionuclide-labeled fibroblast activation protein inhibitor (FAPI) PET imaging after AMI, respectively. This study aimed to evaluate the cardiac inflammation-fibrosis processes after AMI by the spatiotemporal distribution features of myocardial 18F-AlF-NOTA-FAPI and 18F-FDG activity, and further, to explore the relationship between fibroblast activation and cardiac outcomes.
Methods: AMI was induced in 7 healthy Chinese minipigs with self-made emboluses (the balloon combined with gel sponge) placed 1~2mm below the first diagonal branch of the left anterior descending coronary artery (LAD). Serial 99mTc-sestamibi SPECT/CT myocardium perfusion imaging, 18F-AlF-NOTA-FAPI and 18F-FDG cardiac PET/CT imaging under fasting and heparin conditions were performed at acute phase (7 days), subacute phase (14 days), and chronic phase (3 months) in minipigs after AMI. Additional gated 18F-FDG myocardial metabolic imaging was conducted to acquire cardiac function parameters including end-diastolic volume (EDV), end-systolic volume (ESV) and left ventricular ejection fraction (LVEF). Regional analysis was performed on cardiac 18F-AlF-NOTA-FAPI and 18F-FDG inflammatory PET/CT images at different time periods, including the maximum standardized uptake value (SUV max), the mean standardized uptake value (SUV mean) and the extent of elevated tracer uptake activity (%LV), which was identified by polar map area with SUV above a threshold of mean + 2 standard deviations of blood pool activity of left atrium using cardiac PMOD software. One pig was sacrificed after imaging in each time point, and all the remaining minipigs were euthanized in the last time point. The hearts were removed for ex vivo analysis, including H&E staining, Masson’s trichrome staining, and immunochemical staining.
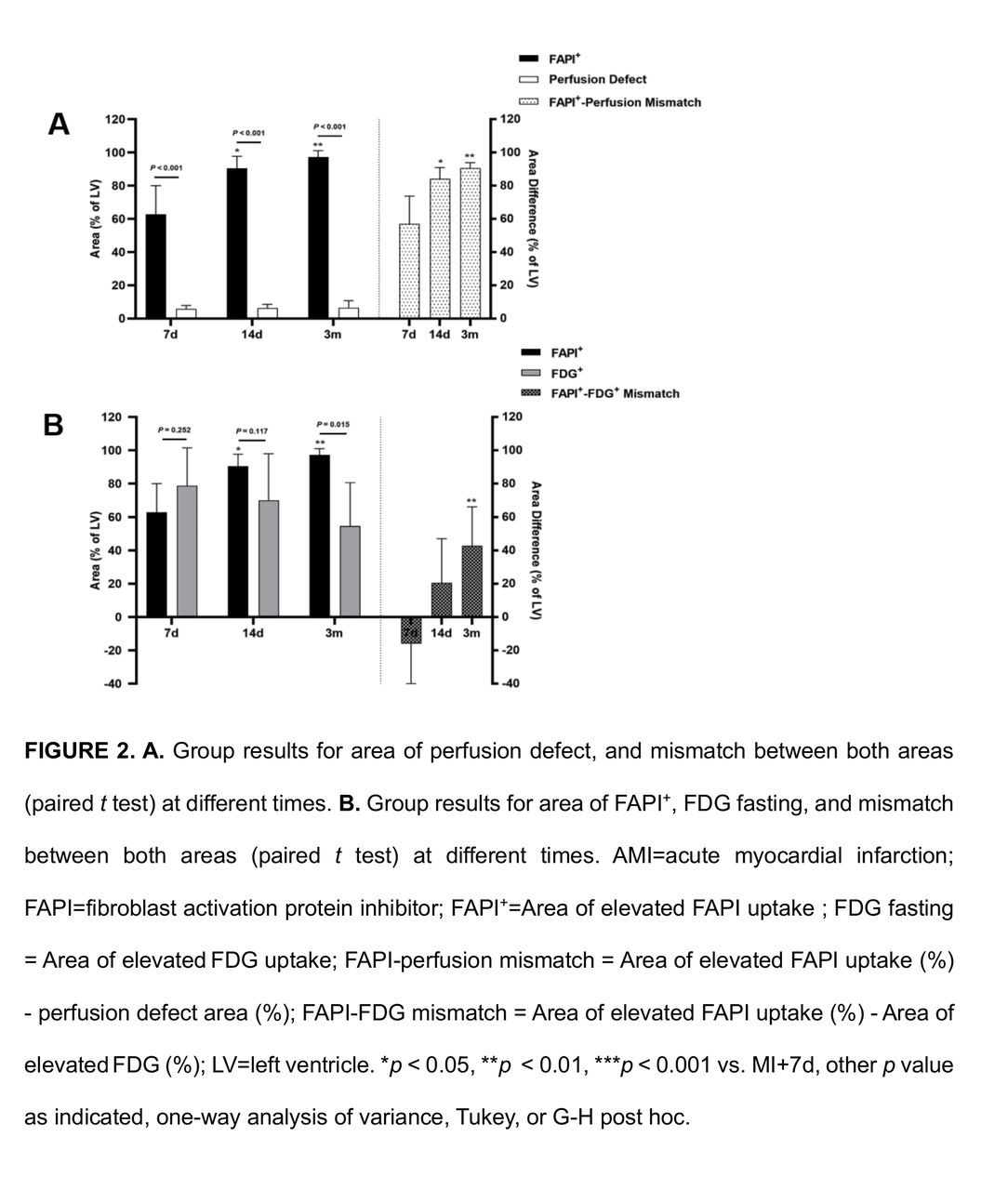
Results: 18F-AlF-NOTA-FAPI enriched region was larger than the perfusion defect at the acute, subacute, and chronic phases (62.9 ± 17.2% vs. 5.8 ± 2.1%, p < 0.001; 90.5 ± 7.2% vs. 6.3 ± 2.2%, p < 0.001; 97.3 ± 3.8% vs. 6.3±2.2%, p < 0.001, respectively), and the mismatch between both areas gradually increased over time (p = 0.002) (Fig.2). 18F-AlF-NOTA-FAPI (62.9 ± 17.2%) and 18F-FDG enriched regions (78.9 ± 22.7%) overlaid at acute phase after AMI on polar map (p = 0.252), both located in the infarcted region and peri-infarcted myocardium (Fig.1). The activity of 18F-AlF-NOTA-FAPI and18F-FDG(SUVmax) declined in enriched regions with time prolonged, which was the lowest at the chronic phase (p < 0.001, p = 0.043). The extent of 18F-FDG enriched region was gradually reduced while the extent of enriched 18F-AlF-NOTA-FAPI was expanded progressively. 18F-AlF-NOTA-FAPI uptake elevated region nearly spread over the whole left ventricle at the chronic phase (97.3 ± 3.8%), which was significantly larger than that in the acute phase (62.9 ± 17.2%, p = 0.004) (Fig.2). Histology analysis confirmed the presence of FAP expression in the 18F-AlF-NOTA-FAPI uptake elevated region. Additionally, there was a significant correlation between SUVmax of 18F-AlF-NOTA-FAPI in the infarct myocardium at 7 days and changes in EDV (r = 0.909, P = 0.032) and ESV (r = 0.911, P = 0.032) from 7 days to 3 months.
Conclusions: Our study revealed a spatiotemporal variation of cardiac inflammation-fibrosis processes post-MI injury by in vivo 18F-AlF-NOTA-FAPI and 18F-FDG PET imaging. Further, the early 18F-AlF-NOTA-FAPI activity could predict subsequent ventricular remodeling.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.