


Abstract
2267
Introduction: We performed the first-in-human clinical trial to evaluate the expression of PARP-1, the target of PARP-inhibiting (PARPi) medications, in prostate cancer using 18F-FluorThanatrace (18F-FTT), a rucaparib analogue. Recent FDA approvals for PARPi in metastatic castrate resistant prostate cancer have improved clinical outcomes in men with DNA-damage repair (DDR) deficient prostate cancer. However, selection of these patients using genetic biomarkers such as homologous recombination deficiency (HRD) are insufficient to predict who may respond to these medications. We report the first clinical trial of non-invasive in vivo assessment of PARP-1 expression in men with prostate cancer.
Methods: Men with intact, clinically localized prostate cancer with planned radical prostatectomy were included. Patients were required to have at least 2 biopsy cores with >50% involvement, OR >1cm dominant prostate lesion on MRI. Men received a single pre-operative [18F]FluorThanatrace ([18F]FTT) scan. [18F]FTT is a radiopharmaceutical that selectively measures the in vivo inhibition of the PARP-1 nuclear enzyme with positron emission tomography (PET/CT). Patients received a single injection of approximately 8-12 mCi of [18F]FTT and underwent 60 minutes of dynamic scanning, following by a static scan approximately 90 minutes post-injection. All patients consented to providing prostate tissue. Ex vivo immunohistochemistry and digital autoradiography was performed after surgical removal. The study was approved by the University of Pennsylvania IRB (UPCC #13817, ClinicalTrials.gov, number NCT03334500).
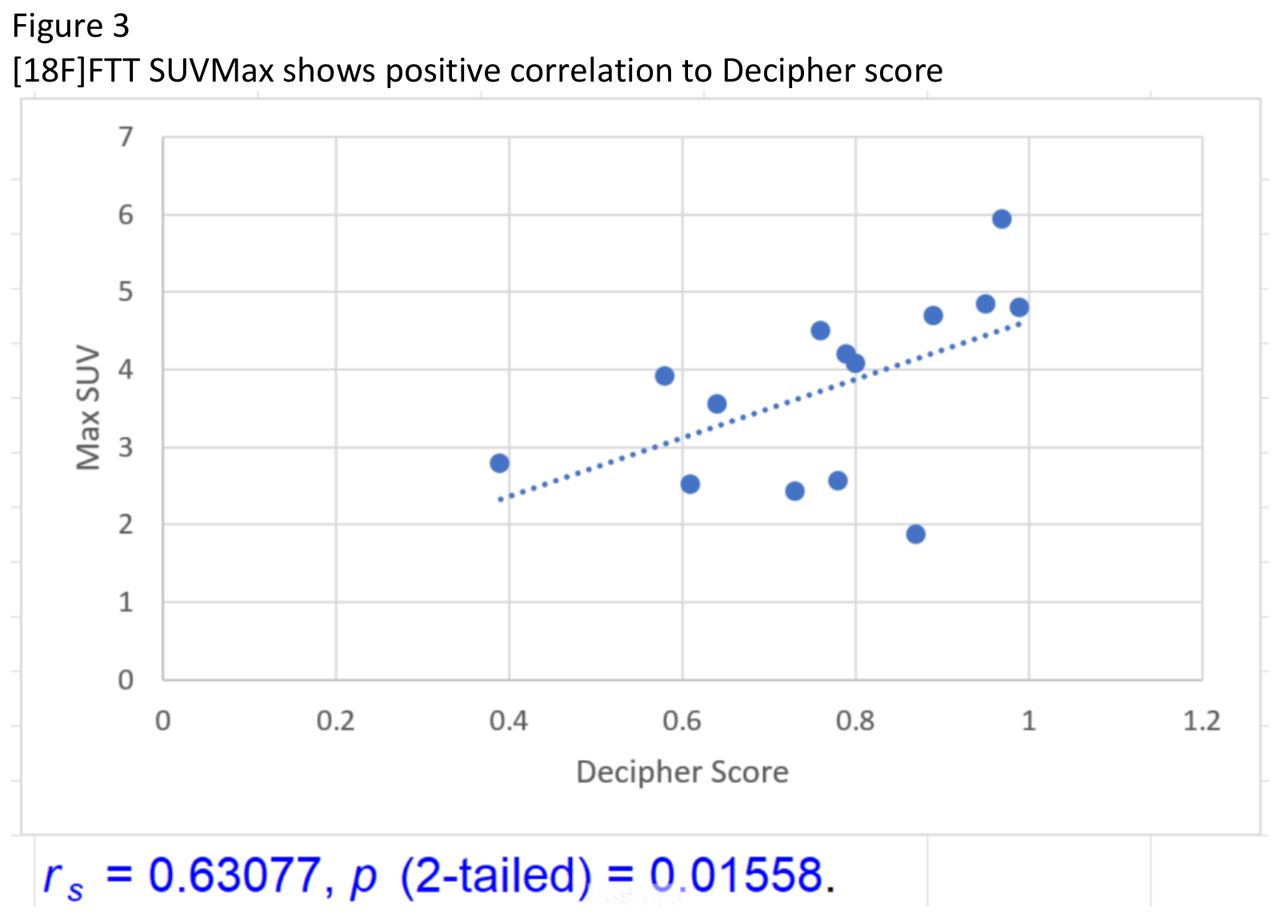
Results: From June 2019 to December 2020, 30 men consented for participation, of which 29 had a presurgical MRI. Mean PSA was 9.8 ng/mL (range 2.35 – 60) and dominant prostate lesion size 1.9cm (range 0.8 – 3.4). Gleason Grade (GG) groups included: GG 1 (n=1), GG 2 (n=10), GG 3 (n=5), GG 4 (n=7), and GG 5 (n=7). Stages included: pT2 (n=12), pT3a (n=10), pT3b (n=8). There were two patients with pN1 disease (cN0 by MRI). Mean injected dose was 10.32 mCi (range 7.52 – 11.62). There were no serious adverse events noted for any patient. Of the patients with a presurgical MRI, a range of uptake on the PET/CT was seen to correlate to the dominant intraprostatic lesion identified by MRI (Figure 1). The mean and median SUVMax of all lesions was 3.52 and 3.46, respectively (range 1.03 – 6.56). Both patients with pathologically involved nodes had those nodes identified on the [18F]FTT scan, and did not meet size or morphologic criteria on the MRI. SUVMax was significantly associated with increasing Gleason Grade group (Figure 2) Rs = 0.37298, p (2-tailed) = 0.04. SUVMax was significantly associated with Decipher scores (Figure 3) (GenomeDx Biosciences, San Diego, CA), a genomic test predictive of metastasis and cancer-specific mortality Rs = 0.63077, p (2-tailed) = 0.02. Ex vivo IHC showed localization of PARP1 staining on prostate specimens to the regions identified on MRI. Ex vivo autoradiography using [I125]KX1, a FTT analogue, is ongoing (Figure 4).
Conclusions: [18F]FTT is able to detect in vivo PARP-1 expression in localized, clinically significant prostate cancer. This tracer may be used to as an imaging biomarker in men with prostate cancer that expresses PARP-1, the target of PARPi. [18F]FTT SUVMax is associated with higher Gleason Grade groups and Decipher scores, both of which prognosticate poorer outcomes. A follow-up study to assess change in [18F]FTT uptake before and after administration of PARPi in men with metastatic prostate cancer is underway to test [18F]FTT as an imaging biomarker for treatment selection for and response to PARPi (UPCC #08821).




In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.