


Abstract
The improvement of existing techniques and the development of new molecular imaging methods are an exciting and rapidly developing field in clinical care and research of neurodegenerative disorders. In the clinic, molecular imaging has the potential to improve early and differential diagnosis and to stratify and monitor therapy in these disorders. Meanwhile, in research, these techniques improve our understanding of the underlying pathophysiology and pathobiochemistry of these disorders and allow for drug testing. This article is an overview on our perspective on future developments in neurodegeneration tracers and the associated imaging technologies. For example, we predict that the current portfolio of β-amyloid and tau aggregate tracers will be improved and supplemented by tracers allowing imaging of other protein aggregation pathologies, such as α-synuclein and transactive response DNA binding protein 43 kDa. Future developments will likely also be observed in imaging neurotransmitter systems. This refers to both offering imaging to a broader population in cases involving the dopaminergic, cholinergic, and serotonergic systems and making possible the imaging of systems not yet explored, such as the glutamate and opioid systems. Tracers will be complemented by improved tracers of neuroinflammation and synaptic density. Technologywise, the use of hybrid PET/MRI, dedicated brain PET, and total-body PET scanners, as well as advanced image acquisition and processing protocols, will open doors toward broader and more efficient clinical use and novel research applications. Molecular imaging has the potential of becoming a standard and essential clinical and research tool to diagnose and study neurodegenerative disorders and to guide treatments. On that road, we will need to redefine the role of molecular imaging in relation to that of emerging blood-based biomarkers. Taken together, the unique features of molecular imaging—that is, the potential to provide direct noninvasive information on the presence, extent, localization, and quantity of molecular pathologic processes in the living body—together with the predicted novel tracer and imaging technology developments, provide optimism about a bright future for this approach to improved care and research on neurodegenerative disorders.
With the growing elderly population and the consequently increased prevalence of neurodegenerative conditions, there is a public health need to identify individuals at risk of developing syndromes associated with these diseases. Alzheimer disease (AD) and Parkinson diseases are the most prevalent neurodegenerative conditions in the elderly. Furthermore, better understanding of the interaction of the known pathomechanisms involved in neurodegeneration is required, as well as better insight into additionally contributing factors, yet insufficiently understood.
Molecular imaging biomarkers today allow identification and quantification of the degree and extent of several of the known underlying pathologic traits in these conditions, permitting better characterization of disease and a more precise approach to the identification of risk factors. These can have independent or combined—synergistic, potentiating, or antagonistic—effects on the specific phenotype.
Molecular imaging markers of pathology, such as β-amyloid and tau imaging, and markers of neurodegeneration, such as brain glucose hypometabolism, have already been incorporated into new diagnostic criteria. Furthermore, molecular imaging studies have proven that the development of the underlying pathologic traits, such Aβ deposition in AD or loss of nigrostriatal terminals in Parkinson disease, is a long and protracted process that precedes the clinical phenotype for decades.
In AD, the introduction of biomarker-based approaches for the identification of brain pathology has informed new strategies for the design of clinical trials aimed at preventing or delaying the onset of cognitive impairment and dementia. The implementation of these biomarkers has shown that defining disease purely on the basis of the clinical syndromal appearance will not be sufficient to select suitable patients for therapies (i.e., exhibiting the therapy target or neuropathology). The implementation of multimodal imaging may also be the most reliable way to allow early initiation of therapy in patients at risk before development of extended irreversible neuronal injury. These imaging biomarkers may therefore play an increasingly important role in patient selection and monitoring of novel therapy approaches.
Many of the great advances and developments in the field of molecular imaging in neurodegeneration are covered in greater detail in the other articles of this supplement issue. In this article, we give a general outlook on the needs and further developments in the field.
DEVELOPING NEW TRACERS FOR PROTEIN AGGREGATION PATHOLOGY IMAGING IN NEURODEGENERATIVE DISORDERS
Most neurodegenerative disorders are histopathologically characterized by the presence of certain protein aggregates. These include β-amyloid, tau, α-synuclein, transactive response DNA binding protein 43 kDa (TDP-43), and other aggregates.
The detection of these pathologic protein accumulations in certain brain areas by postmortem histopathology has been considered the gold standard to diagnose these disorders. The successful introduction of radiotracers to image β-amyloid and tau pathology in vivo has shifted the time point of accurate diagnosis from postmortem to antemortem, and even possibly to prodromal disease stages, and allows assessment of changes over time. This is important because accurate in vivo diagnosis can impact individual patient management.
The current state of already-established PET tracers to image brain β-amyloid and tau pathology is discussed in separate contributions to this supplement. However, further developments in the field of tracers for protein aggregation pathologies are highly relevant in several respects. In specific neurodegenerative diseases, more than one proteinopathy is often present, as in AD, in which β-amyloid and tau proteins are found. Conversely, specific protein pathologies are often found in different neurodegenerative diseases, such as tau, which is present not only in AD but also in certain forms of frontotemporal dementia, movement disorders such as corticobasal degeneration or progressive supranuclear palsy, and primary age-related tauopathy. Although the aggregates found in these tauopathies are based on the same protein, they differ in brain location, affected cell type, and structure. Whereas in AD, for instance, predominantly intraneuronal tau aggregates in the form of paired helical filaments are found, in other tauopathies, such as corticobasal degeneration or progressive supranuclear palsy, aggregates of straight filaments are observed more frequently, located also in glial cells (1). These facts explain the need for tracers with high affinity for specific tau accumulation forms. Some of the second-generation tau PET tracers have been studied (discussed in another article in this supplement), but the development of tauopathy-selective compounds may be worthwhile. With regard to β-amyloid tracers, this development might also refer to different amyloid pathologies such as vascular β-amyloid to diagnose cerebral amyloid angiopathy, or β-amyloid oligomers in AD to place PET imaging closer to the neurodegenerative process.
Regarding β-amyloid imaging, there is also the question of whether we will see SPECT tracers emerge. In principle, a relevant place for such tracers as an addition to the established PET tracers is anticipated because the prevalence of AD is growing, the hope for the emergence of more disease-modifying drugs is high, and the target density in the affected brain is high enough to allow visualization by SPECT. To explore this intriguing concept, different groups have performed intensive work over the last few years (2–6) but without a major breakthrough so far, although preclinical data were promising. This current lack of success seems to be related mainly to insufficient signal-to-noise ratios in the human brain and high blood flow effects on target retention. It will be fascinating to observe whether optimized β-amyloid SPECT tracer candidates, eventually developed by novel drug development technologies, will be more successful.
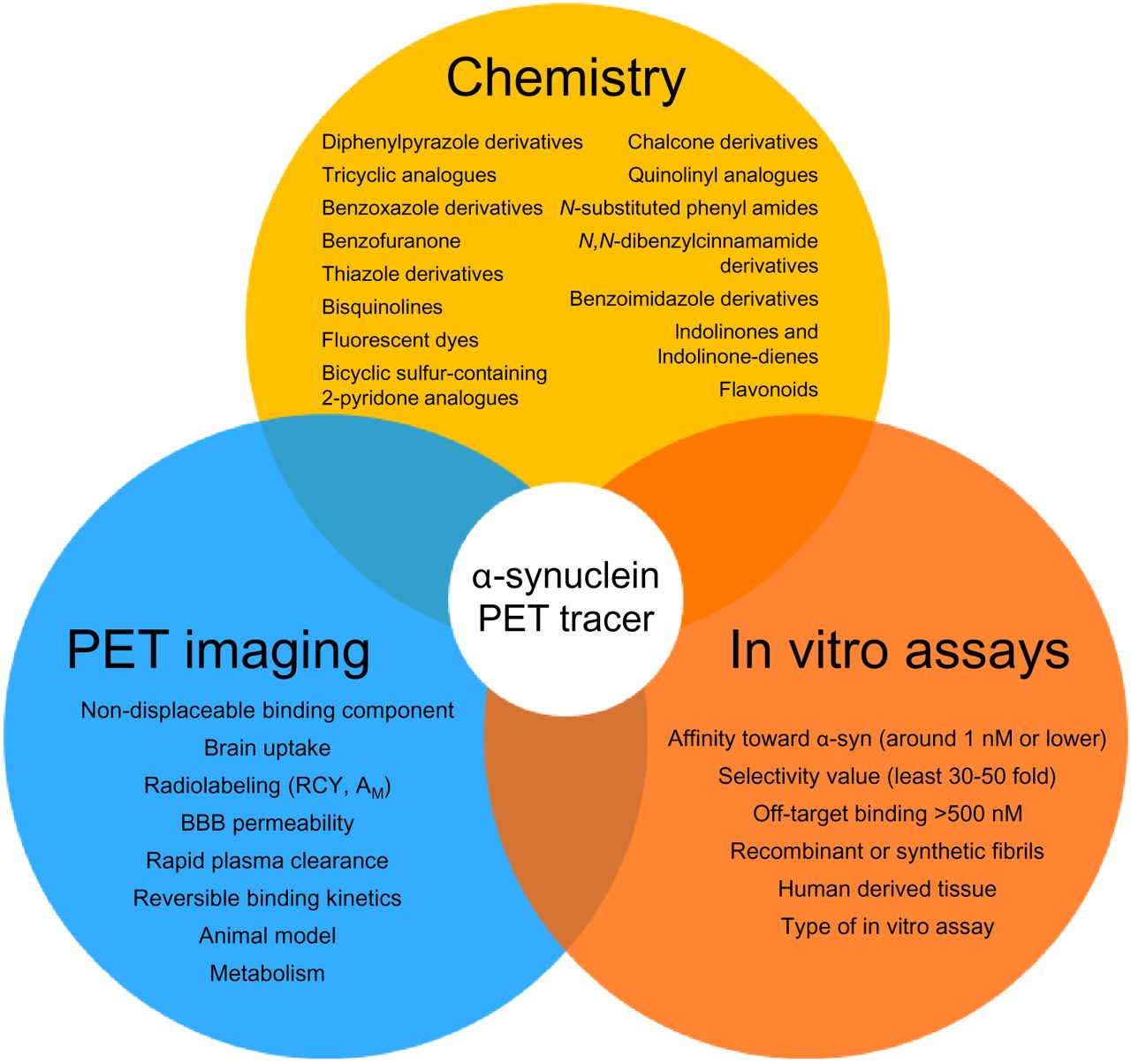
Apart from these efforts to extend the tracer portfolio to image β-amyloid and tau, there are increasing efforts to develop PET tracers for other protein aggregates. These include tracers to image α-synuclein aggregates, which represent the histopathologic hallmark of Parkinson disease, Lewy body dementia, and multisystem atrophy. If successful, PET tracers selective for α-synuclein would significantly extend the concept of in vivo histopathology-based diagnosis to many new patients. The current state of development in this field was recently reviewed in an elegant manner by Korat et al. (7). The development of α-synuclein tracers faces 3 challenges. First, the target density is low compared with that of β-amyloid and tau aggregates or some enzymes such as monoamine oxidases. Second, avoidance of cross-selectivity is complicated, because to date, the tracers are aimed at binding β-sheets, the same secondary structure as found in β-amyloid and tau aggregates. Third, there is a lack of knowledge on the full crystal structure of the target, but progress with cryogenic electron microscopy might facilitate tracer development (8). As a consequence, α-synuclein tracers need to have exceptionally high binding affinity and selectivity. As Korat et al. noted, molecule candidates of 37 different chemical classes have so far been developed up to different stages (Fig. 1). According to Korat et al., only 2 of them, namely the diphenylpyrazole derivative 11C-MODAG-001 (9) and the quinolinyl analogs of 125I-TZ6184 (10) show sufficient target affinity, and 4 of them present with sufficient binding selectivity over β-amyloid and tau. To our knowledge, none of the tracers tested so far in humans by academic or commercial researchers was successful. The breakthrough may also be hindered by a lack of reliability and reproducibility of the available evaluation assays. There is, however, hope that advanced development strategies such as high-throughput screening, computational modeling, or antibody engineering might be more promising (7).

Overview on current state of candidate classes tested for their potential to provide viable α-synuclein PET tracers, together with recommended in vitro/PET imaging testing strategy. AM = molar activity; BBB = blood–brain barrier; RCY = radiochemical yield. (Reprinted from (7).)
With regard to TDP-43 (a histopathologic hallmark of amyotrophic lateral sclerosis, some forms of frontotemporal dementia, and limbic-predominant age-related TDP-43 encephalopathy), no suitable PET tracers are yet available. It will, thus, also be fascinating to observe whether TDP-43 or other neurodegeneration pathology tracer candidates emerge.
EXTENDING THE ROLE OF IMAGING NEUROTRANSMITTER SYSTEMS IN NEURODEGENERATIVE DISORDERS
In neurodegenerative disorders, the degenerative process may affect all kinds of brain tissue components. Thus, many neurotransmitter systems can be altered in these diseases. Further, specific neurotransmitter deficits can drive the clinical phenotype or represent main symptomatic treatment targets, such as the dopaminergic deficit in Parkinson disease (11) and, at least in part, the cholinergic deficit in AD (12). Other neurotransmitter disbalances seem to be responsible for comorbidity, such as serotonergic imbalance causing depressive symptoms (13) in several neurodegenerative diseases. PET and SPECT are the only imaging techniques capable of in vivo tracking of the state of these neurotransmitter systems and of respective drug effects. These imaging techniques play a significant role, both for clinical routine and for research—for example, to investigate the involvement of different neuroreceptor or transmitter systems in neurodegenerative disorders and to potentially develop new treatments. Imaging of the cholinergic and serotonergic systems may improve patient selection for and monitoring of specific symptomatic treatments and, in combination with pathologic imaging markers, measurement of potential multilevel drug effects.
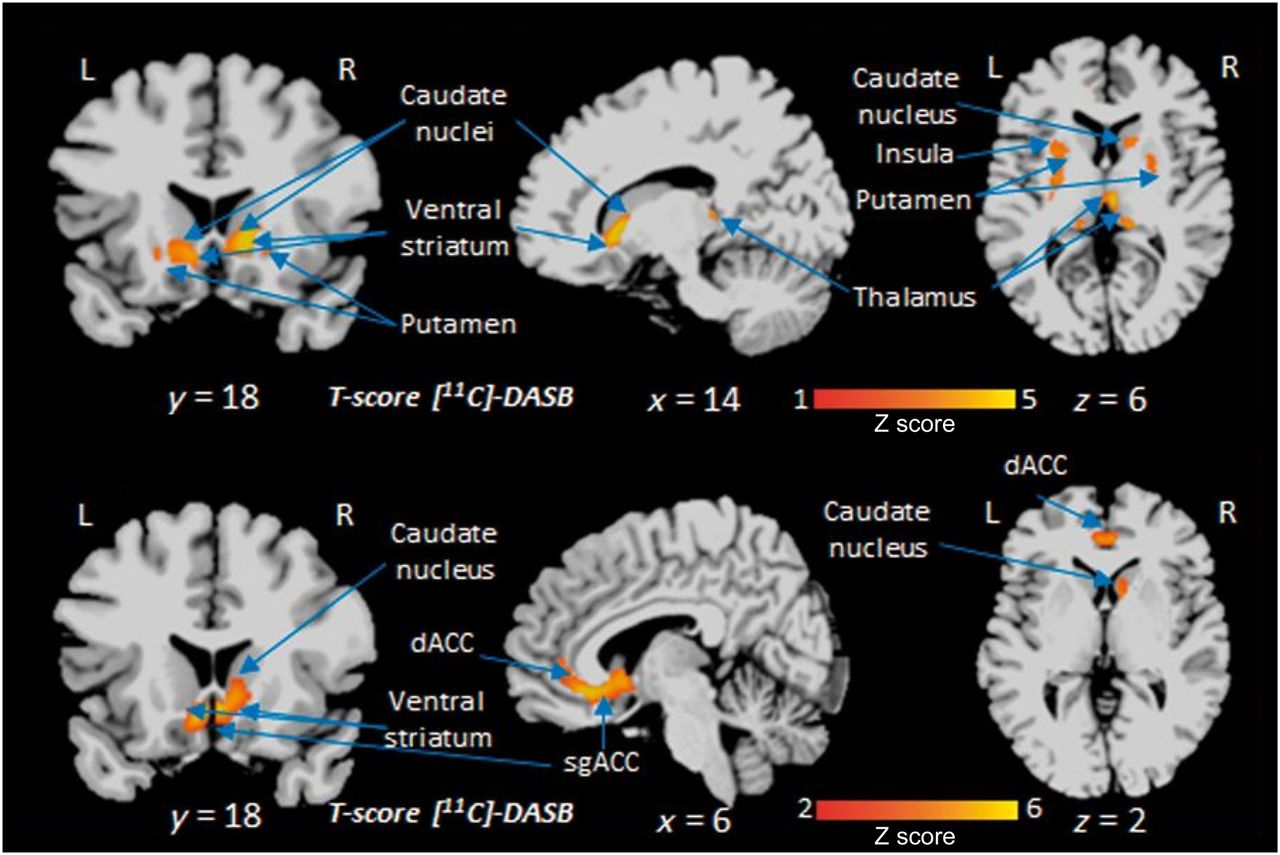
Because of their exceptional role in neurodegenerative diseases, molecular imaging techniques assessing the dopaminergic and cholinergic systems in the brain are discussed in separate contributions to this supplement. Could imaging of other neurotransmitter systems find greater application in neurodegenerative diseases? One definitive candidate is the serotonergic system. Several PET tracers are available to image different aspects of this system (14). Of major interest is the serotonin transporter, a monoamine transporter that carries serotonin back from the synaptic cleft to the presynaptic neuron. Serotonin reuptake inhibitors, drugs that ameliorate depressive symptoms via increasing the concentration of serotonin in the synaptic cleft, target this structure. Future strategies for wider imaging use in the clinic as a means of personalized medicine might individually determine the presence and degree of a serotonergic deficit to guide decisions on whether serotonergic drugs will be considered in subsequent individual treatment decisions (Fig. 2).
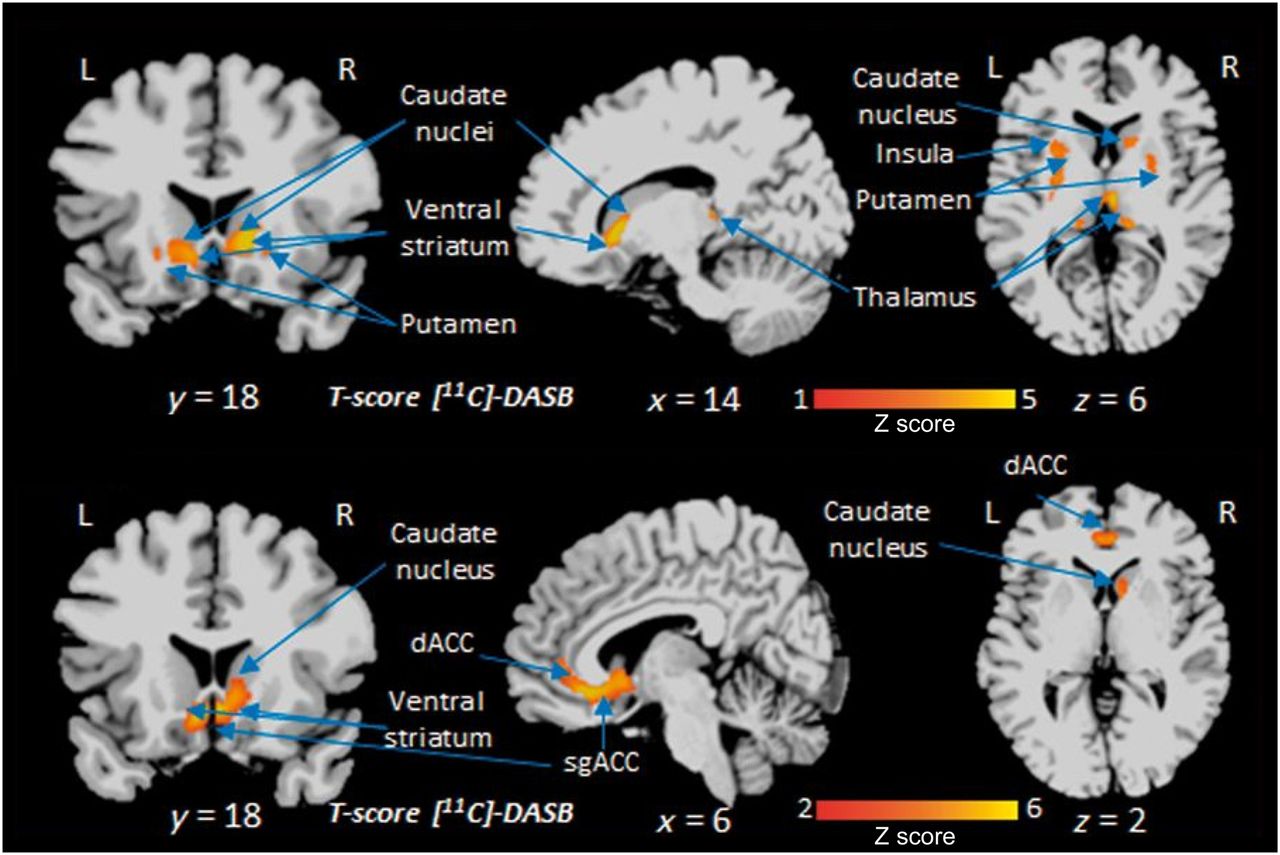
Voxelwise comparison of 11C-labeled 3-amino-4-(2-dimethylaminomethyl-phenylsulfanyl)-benzonitrile (11C-DASB) serotonin transporter PET data of patients with de novo Parkinson disease depending on level of apathy. Clusters of reduced serotonin transporter availability (orange) in several deeper brain areas of apathetic PD patients as compared with healthy controls (top row) and nonapathetic PD patients (bottom row). dACC = dorsal anterior cingulate cortex; sgACC = subgenual anterior cingulate cortex. (Reprinted with permission of (44).)
Another neurotransmitter system that recently emerged as an attractive PET imaging target is the σ1 receptor system. σ1 receptors, formerly grouped with other opioid receptors, are membrane proteins at the endoplasmic reticulum that modulate calcium signaling. They seem to be involved in regulating metabolic cell stress in neurodegenerative diseases. Several PET tracers to image σ1 receptors are now available (15). As a striking example of how to use them in research, the United Kingdom–based multipartner MIND-MAPS initiative is applying the σ1 receptor tracer 11C-SA-4503 in combination with tracers of mitochondrial complex 1 and synaptic vesicle 2A to monitor the multiparametric progress of neurodegeneration across different disorders (16). The first published results of this initiative were encouraging (17). Another recently applied approach—this one using 18F-fluspidine—is to investigate the state of σ1 receptors by PET imaging as a potential drug target to treat Huntington disease (18). It will also be interesting to observe whether and to what extent PET techniques or tracers targeting other neurotransmitter systems, such as tracers that bind to metabotropic glutamate subtype 5 receptors (19) that modulate synaptic transmission and can be compromised by, for instance, β-amyloid oligomers in AD, will find broader research or even some clinical applications. At least for the latter, the fate of such tracers will certainly also depend on the progress made in specific drug developments.
Regarding dopaminergic-system tracers currently in clinical use, the most widely applied is the SPECT tracer 123I-FP-CIT (20). This tracer binds to presynaptic dopamine transporters, thus providing a valuable surrogate readout for the integrity of the nigrostriatal pathway or dopamine-producing neurons in patients with Parkinsonian syndrome or suspected Lewy body dementia. It will be interesting to observe whether this SPECT imaging predominance for this application will change. There are, as an example, tracers available to image dopamine transporters and vesicular monoamine transporters by PET. The use of PET instead of SPECT as the image acquisition technique would have the advantage of providing a higher spatial resolution, quantitative data and the new option of combining molecular with structural imaging by hybrid PET/MRI systems. 18F-FE-PE21, 18F-FP-CIT, and 18F-AV-133 are examples of promising tracers in this regard (Fig. 3) (21–23).
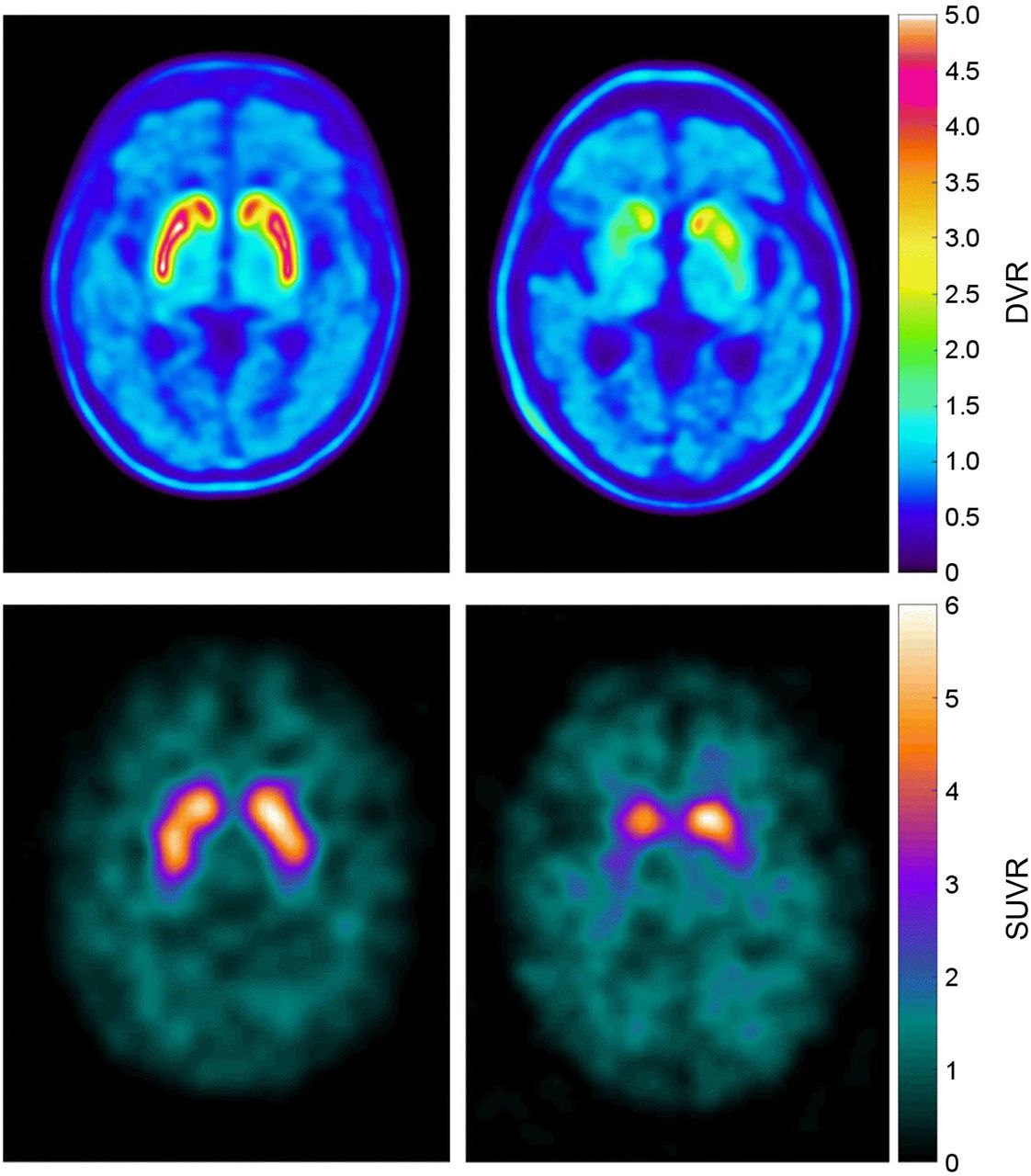
Intraindividual comparison between dopamine transporter imaging by 18F-FE-PE2I PET (top row) and 123I-FP-CIT SPECT (bottom row) in healthy control (left) and patient with Parkinson disease (right). DVR = distribution value ratio; SUVR = SUV ratio. (Reprinted from (21).)
APPLYING NEW TECHNOLOGIES FOR MOLECULAR IMAGING OF NEURODEGENERATIVE DISORDERS
The application of new image acquisition and processing technology is anticipated to improve and broaden the application of molecular imaging in neurodegenerative disorders as well. The following developments are predicted to provide the most significant impact on future neurodegeneration imaging.
PET/MRI
Hybrid PET/MRI technology allows the simultaneous evaluation of molecular and structural or functional changes in the living body. It is considered the tool of choice for brain imaging research. In clinical practice, a breakthrough application has not yet emerged, probably because of the relatively high purchasing and running costs of the scanners and the limited reimbursement options. Clinically, in suspected neurodegenerative diseases, MRI represents the first-line imaging technique, performed mainly to exclude other diseases such as vascular disorders, inflammation, trauma, or tumor. Diagnostic algorithms are available advocating the subsequent use of specific molecular imaging techniques depending on the diagnostic question, such as in dementia work-up (24). However, PET or SPECT imaging is currently performed on only a subset of patients. This limited use might change; for example, the demand for β-amyloid imaging in AD may increase in conjunction with broader availability of antiamyloid drugs. These drugs have relevant side effects, and PET/MRI might be the most expedient way not only to confirm the presence and engagement of the target (25,26) but also to provide structural information before and throughout therapy (27). In particular, regular monitoring for amyloid-related imaging abnormalities (28) by MRI is mandatory for these novel therapies. There is also potential to improve the quality of brain PET data with the support of simultaneously acquired MRI data, such as through MRI-supported PET reconstruction, PET tracer input-function generation, movement correction, partial-volume-effect correction, and PET tracer uptake quantification (Fig. 4) (25).
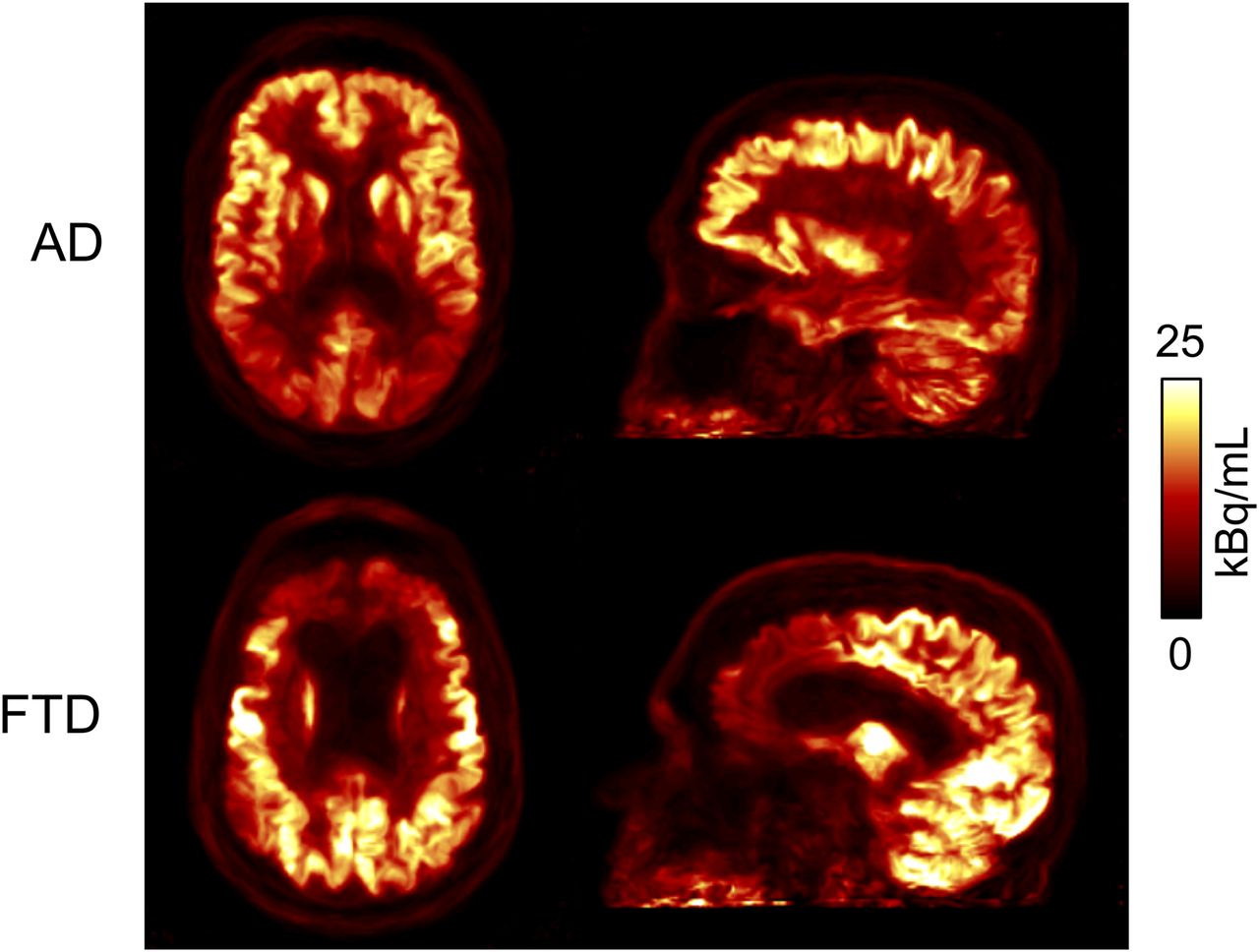
18F-FDG glucose utilization PET images as obtained by hybrid PET/MRI and optimized by MRI-assisted attenuation correction, reconstruction, and movement correction in AD patient and frontotemporal dementia patient. (Reprinted from (34).)
Dedicated Brain PET Scanners
The idea of developing dedicated brain PET scanners follows the desire to allow access of a wider population to PET imaging as the social burden of neurodegenerative diseases increases and effective disease-modifying drugs emerge. Several academic and commercial groups are developing such systems (29). The initial clinical applications for this technology will likely use 18F-FDG but will rapidly extend to the use of amyloid and tau tracers.
Total-Body and Large-Field-of-View PET Scanners
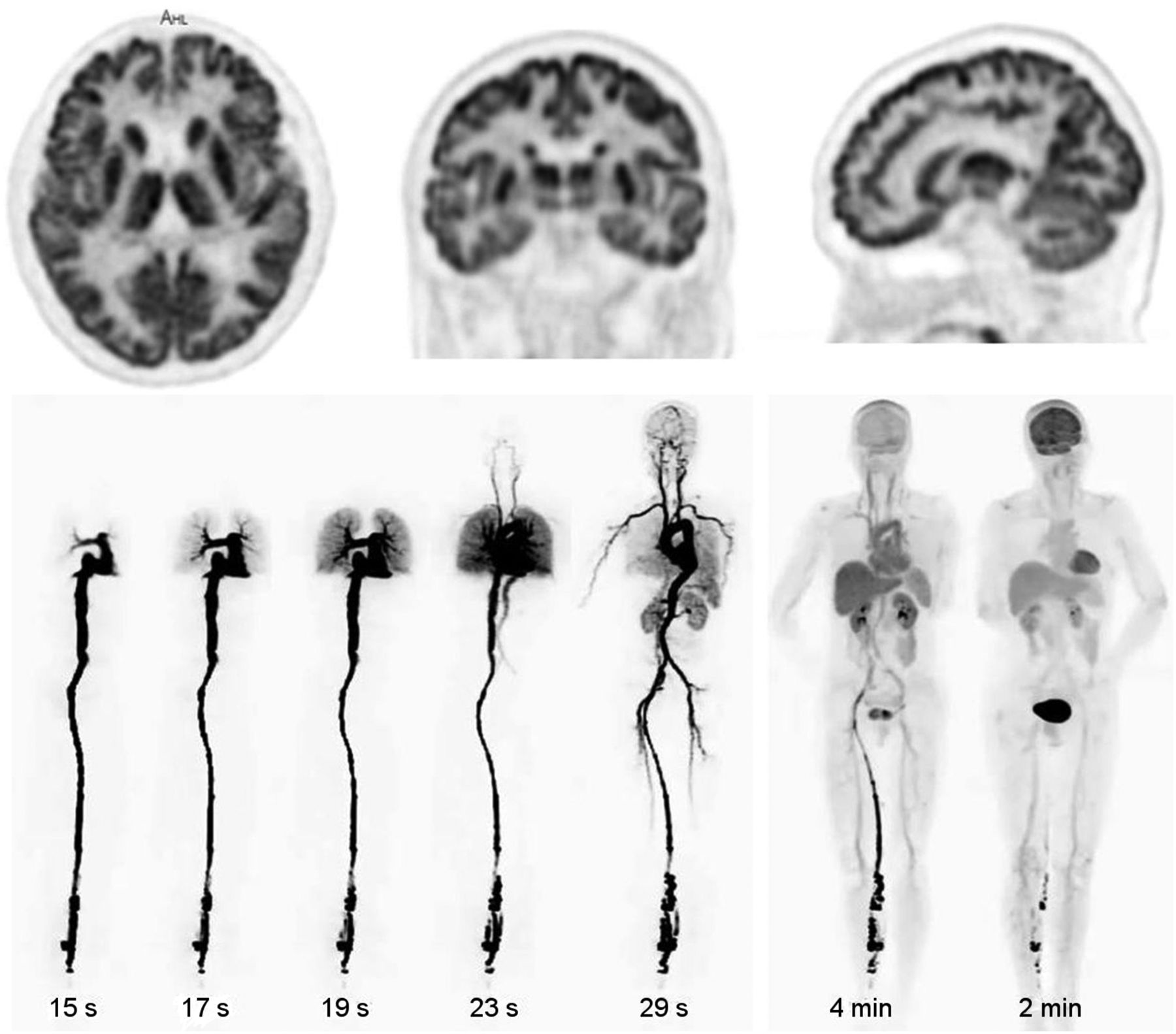
With the recent emergence of total-body and large-field-of-view PET scanners (30), there is a chance to simplify and improve studying the pharmacokinetics, pharmacodynamics, and dosimetry of new PET tracers (Fig. 5). What is more exciting is that it will also be possible to study, for the first time, the integrity of neurohumoral communication systems in the body, such as that of the gut–brain and heart–brain axes, as well as drug effects on these systems simultaneously for the entire body.
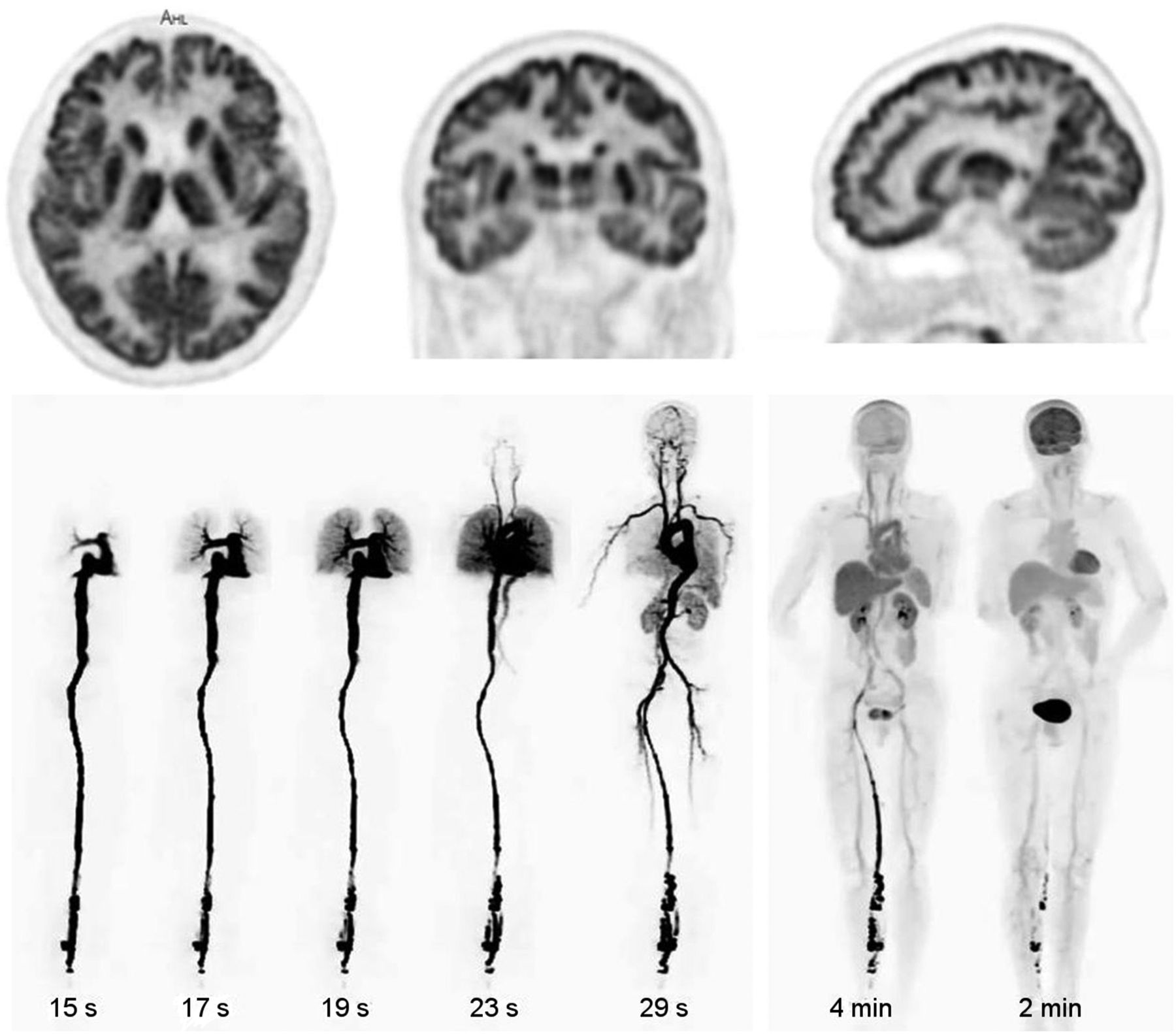
18F-FDG glucose utilization PET images of brain (top row) and dynamically of whole body in healthy volunteers at different time points 0–60 min after tracer administration, with scan durations provided (bottom row). Data were acquired within first-in-humans study of EXPLORER total-body scanner. (Reprinted from (30).)
Advanced Image Acquisition and Processing Protocols
Molecular brain imaging may also benefit from advanced image acquisition protocols. In particular, early perfusion-phase acquisitions with different tracers for amyloid and tau PET have provided results consistent with 18F-FDG PET, allowing dual information to be obtained from a single imaging session (31–33). In addition to this multipurpose function, such protocols would also allow correction of the specific (late-phase) image information for perfusion effects. This ability may allow reliable, perfusion-independent protein pathology quantification, potentially of great importance for therapy response monitoring. In addition to benefiting from new imaging protocols, molecular imaging of the brain may also strongly benefit from new data-processing techniques, particularly using artificial intelligence. These techniques may allow improved image reconstruction of scans with low activity (34), calculation of attenuation even without requiring a CT scan (35), and improved automated image analysis. One example of the latter is extraction of information on multiple pathologies from a single tracer, thus enabling amyloid, tau, and neurodegeneration classification in a single session, as suggested for tau PET (36). Artificial intelligence may open many further unforeseeable opportunities.
All these technologic developments also might reduce radiation exposure, scanning time, and tracer dose by improving system sensitivity (total-body systems), preventing the need for a CT acquisition (hybrid PET/MRI), allowing for single-tracer multipurpose protocols, or improving image reconstruction (artificial intelligence). These advantages might increase acceptance of the imaging tests, reduce costs, allow imaging of less compliant or more radiation-sensitive subjects, allow for larger series of repeated imaging, and allow application of multiple tracers.
WHAT WILL THE FUTURE BRING FOR MOLECULAR IMAGING OF NEURODEGENERATIVE DISORDERS? AN OPTIMISTIC LOOK INTO THE GLASS BALL
Molecular Imaging Will Become the Standard for Diagnosis of Neurodegenerative Diseases
In most centers, PET imaging of patients with suspected neurodegenerative disorders is currently used only as a diagnostic adjunct in uncertain cases. Diagnosis in these patients is based mainly on clinical testing for the presence of certain symptoms, whereas CT or MRI is used to exclude other disorders.
Through the years, this approach to defining neurodegenerative diseases as a syndromal construct, and consequently to diagnosing them on the basis of a certain clinical phenotype, has not led to a breakthrough in curative or disease-modifying treatment. AD was the first neurodegenerative disorder for which a new diagnostic concept was developed. Jack et al. proposed defining AD via biomarker testing for amyloid, tau, and neurodegeneration (37). This concept is already extensively used in research and for drug testing. With the approval of aducanumab by the Food and Drug Administration, we now have a β-amyloid–reducing drug approved to treat AD (38). Other anti–β-amyloid drugs and drugs effectively removing or preventing the formation of tau, α-synuclein, and other pathologic aggregates will hopefully follow. The concept of defining neurodegenerative diseases as a syndromal construct will potentially continue to change toward a definition of neurodegenerative diseases as a biologic construct. New etiologic treatment approaches will require a biomarker-based diagnosis. In this paradigm shift, PET imaging will potentially play a decisive role (Fig. 6).

Molecular Imaging Will Become the Decisive Imaging Test for Experimental and Clinical Drug Application
Already, 18F-FDG, amyloid, tau, dopaminergic-system, and other neurotransmission tracers are being used for drug evaluation in neurodegenerative disorders (27). This portfolio will be reinforced by tracers to image different aspects of neuroinflammation and synaptic density, for which the current state of knowledge is summarized in separate reviews in this supplement.
For example, there is increasing understanding that removing pathologic proteins might produce a better clinical outcome if the drug is administered earlier. The concept is being explored of applying these drugs in prodromal or even asymptomatic subjects to prevent clinical manifestation of the disease, with the ongoing A4 trial in AD being one example (39). In such subjects, because clinical testing or structural imaging does not allow validation of the treatment rationale, molecular imaging will potentially gain more relevance for this purpose. Further, longitudinal molecular imaging is the ideal tool to assess regional treatment effects directly within the brain. Future scenarios are imaginable in which serial imaging allows individual tailoring of treatment intensity and duration, another perfect example of personalized medicine. Because PET is the only technique that can measure the regional distribution and density of the imaging target in an absolute quantitative manner, efforts to standardize quantitative PET readouts across different tracers for the same target and across centers will potentially gain more relevance, such as the centiloid concept in amyloid imaging (40).
Use of β-amyloid PET in aducanumab prescription is a subject of controversy, which recently culminated in a limited-coverage decision by the Centers for Medicare and Medicaid Services (41). β-amyloid PET was used in the drug development program, first, to stratify patients at baseline according to the presence of the drug target and, second, to serve as a secondary outcome measure. Amyloid PET imaging should be considered mandatory for selecting patients for therapy with this drug. Interestingly, however, the authors of recently published appropriate-use criteria for aducanumab treatment suggested that patients may also be included on the basis of cerebrospinal fluid (CSF) analysis, although conceding that patients positive on CSF testing but negative on β-amyloid PET should not be treated and that patients with inconclusive CSF results should undergo amyloid PET (42). Because CSF sampling was not validated as an entry test for aducanumab treatment, and specifically given the potentially avoidable side effects and costs in cases of false-positive CSF tests, caution should be used when considering this suggestion. Because of the controversies about the efficacy of anti-amyloid therapy at the dementia stage, it also appears advisable to perform amyloid PET follow-up examinations to validate and quantify therapy effects, which CSF sampling is not capable of doing (38).
Molecular Imaging Will Redefine Its General Role with Regard to Fluid Biomarkers to Diagnose Neurodegeneration
β-amyloid and tau PET imaging are competing with CSF sampling when it comes to clinical routine binary classification of suspected AD patients. It is interesting that there has also been relevant progress in potentially substituting CSF testing for AD biomarkers by less invasive blood sampling (43). This progress raises the question of what specific value PET imaging will have. The answer potentially depends on what kind of PET readout is obtained and for which purpose the diagnostic test is performed. In stages of clinically manifest dementia, blood sampling may provide a similar answer on whether β-amyloid pathology is present. However, in prodromal disease stages, which probably last for decades, β-amyloid PET may allow assessment not only of the presence but also the stage and location of the pathology and therapeutic target—an assessment that does not seem feasible by CSF or blood tests. The situation may again be different for tau imaging, for which different tauopathies are diagnosed and differentiated via evaluation of the regional PET signal, a property that fluid biomarkers cannot provide. An alternative prediction combines relatively inexpensive screening of at-risk subjects with blood biomarker testing, followed by diagnostic confirmation through PET imaging to provide a rationale for drug treatment and a baseline for subsequent drug monitoring (a property that, again, fluid biomarkers have not been shown capable of providing; Fig. 7). Besides this use, PET imaging of β-amyloid and tau will certainly still play a decisive role in testing during the early development phase of drugs because of its unique ability to provide absolute quantitative data on the density of treatment targets in the brain. PET imaging will also serve as the gold standard in vivo test against which novel fluid biomarkers are validated.
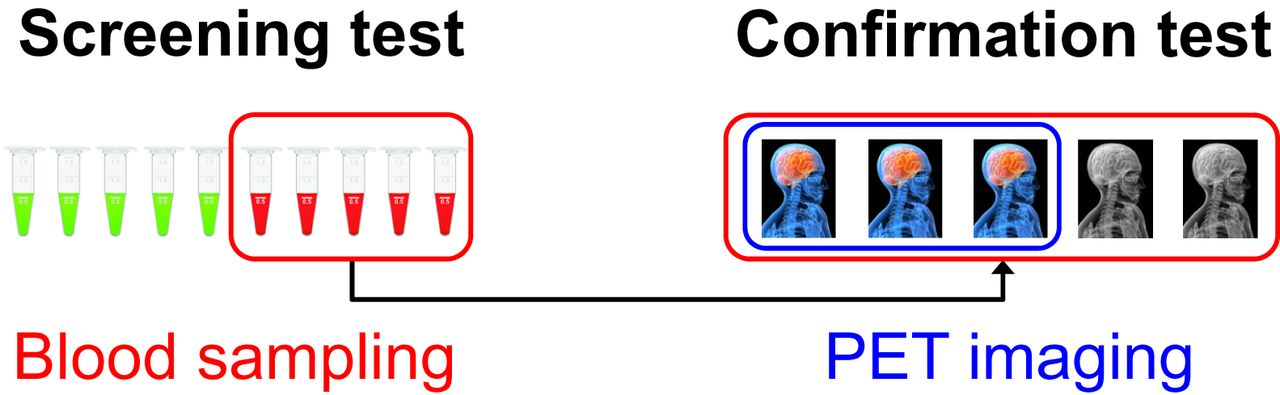
Schematic presentation of future scenario in diagnosis of neurodegenerative disease based on pathology biomarkers. Subjects at risk or even all subjects will be screened by blood test for β-amyloid, tau, α-synuclein, TDP-43, and others. This screening test will be optimized for sensitivity, that is, tolerating certain number of false-positives. Positives based on blood test will then undergo respective (or multiple) brain PET scans as confirmation testing. This confirmation testing will be optimized for specificity. It will establish or exclude diagnosis, as well as presence of dedicated drug targets, and will serve as baseline test for subsequent therapy monitoring in cases of disease-modifying drug prescription.
SUMMARY AND CONCLUSION
Motivated by the ongoing paradigm shift in defining and diagnosing neurodegenerative diseases through the underlying pathology, and by new hope for a breakthrough in disease-modifying drugs, there is great enthusiasm about advancing this facet of the field of molecular imaging. It is predicted that techniques will be improved, be made more broadly available, be supplemented by new tracers targeting aspects of neurodegeneration not previously trackable in vivo, and be enhanced by new approaches to acquiring, processing, and analyzing images.
There is still a considerable gap between the unique possibilities of in vivo characterization of neurodegenerative diseases and the frequency with which these modern molecular imaging methods are applied. Although some imaging biomarkers, such as 18F-FDG, dopaminergic, or β-amyloid tracers, have been available for a quite some time and their value is well established, their broader integration into clinical neurologic routine has not yet been achieved. This shortfall is seriously discrepant with, for instance, the extent to which PET imaging has been integrated into the oncologic standard of care. Thus, the results of prospective, outcome-oriented multicenter trials such as IDEAS (https://www.ideas-study.org/) and AMYPAD (https://amypad.eu/) need to be translated into reimbursement decisions. Also, for the recently Food and Drug Administration–approved tau tracer 18F-flortaucipir, application has been restricted mainly to drug testing trials, with only limited use for diagnostic assessment, internationally. Systematic integration of these tools into clinical practice appears overdue.
In addition to improved implementation of existing tools into the clinical praxis, molecular imaging bears great potential to extend our view outside the beaten track to other factors involved in neurodegeneration, such as different protein aggregates, synaptic loss, inflammation, and various neurotransmitter dysbalances. Finally, molecular imaging in neurodegeneration may benefit from developments in imaging instrumentation and data processing, such as hybrid PET/MRI and artificial intelligence. We believe that colleagues in neuronuclear medicine would be well advised to take advantage of these innovations. Also, the obvious advantages of imaging tools over other biomarkers of neurodegeneration—that is, the provision of direct information on the presence, extent, localization, and quantity of neuropathology—justify mandatory use of these tools in selecting patients and monitoring their response to modern causal therapy. Finally, advances in tracers and imaging technology may even allow clinical protocols with multiple time points and multiple tracers. The nuclear imaging community should intensify efforts to implement such personalized protocols.
Because of space restrictions, this overview cannot address all questions and future challenges in greater detail. One question is, What are the limitations of the biomarkers mentioned, and how do these limitations impact diagnostic value? For example, in emerging tau tracers, the selectivity and degree of binding translate to differences in the effect on differential diagnosis and on detection of changes on longitudinal imaging. Another question is, To what degree is the possibility of new biomarkers to image neurodegenerative diseases counterbalanced by practical problems such as access to instrumentation and tracers, imaging capacity, equity and cost-effectiveness? Regional differences in these features only add to the complexity. As a third question to consider, Are the thoroughness of neurodegeneration biomarker development and the speed of clinical translation always adequate? Similar questions can be asked about drug development. Academia should abstain from pressure related to nonacademic factors and adhere to the concept of evidence-based science. All open questions such as these are significant and deserve careful consideration.
The future of molecular imaging of neurodegenerative diseases is bright. More work is required, but developments in this exciting field will expand use both clinically and in research, to the betterment of our patient care.
DISCLOSURE
Henryk Barthel received speaker honoraria from Novartis/AAA and reader honoraria from Life Molecular Imaging. Victor Villemagne received consulting fees from Eli Lilly, Life Molecular Imaging, Hospicom, and IXICO and speaker honoraria from ACE Barcelona and IXICO. Alexander Drzezga received research support from Siemens Healthineers, Life Molecular Imaging, GE Healthcare, AVID Radiopharmaceuticals, and SOFIE; received speaker/advisory board honoraria from Siemens Healthineers, Sanofi, GE Healthcare, Biogen, Novo Nordisk, and Invicro; owns stocks from Siemens Healthineers and Lantheus Holding; and holds a pending patent for 18F-PSMA7. No other potential conflict of interest relevant to this article was reported.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication January 31, 2022.
- Revision received April 19, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- DEVELOPING NEW TRACERS FOR PROTEIN AGGREGATION PATHOLOGY IMAGING IN NEURODEGENERATIVE DISORDERS
- EXTENDING THE ROLE OF IMAGING NEUROTRANSMITTER SYSTEMS IN NEURODEGENERATIVE DISORDERS
- APPLYING NEW TECHNOLOGIES FOR MOLECULAR IMAGING OF NEURODEGENERATIVE DISORDERS
- WHAT WILL THE FUTURE BRING FOR MOLECULAR IMAGING OF NEURODEGENERATIVE DISORDERS? AN OPTIMISTIC LOOK INTO THE GLASS BALL
- SUMMARY AND CONCLUSION
- DISCLOSURE
- REFERENCES
- Figures & Data
- Info & Metrics