


Visual Abstract

Abstract
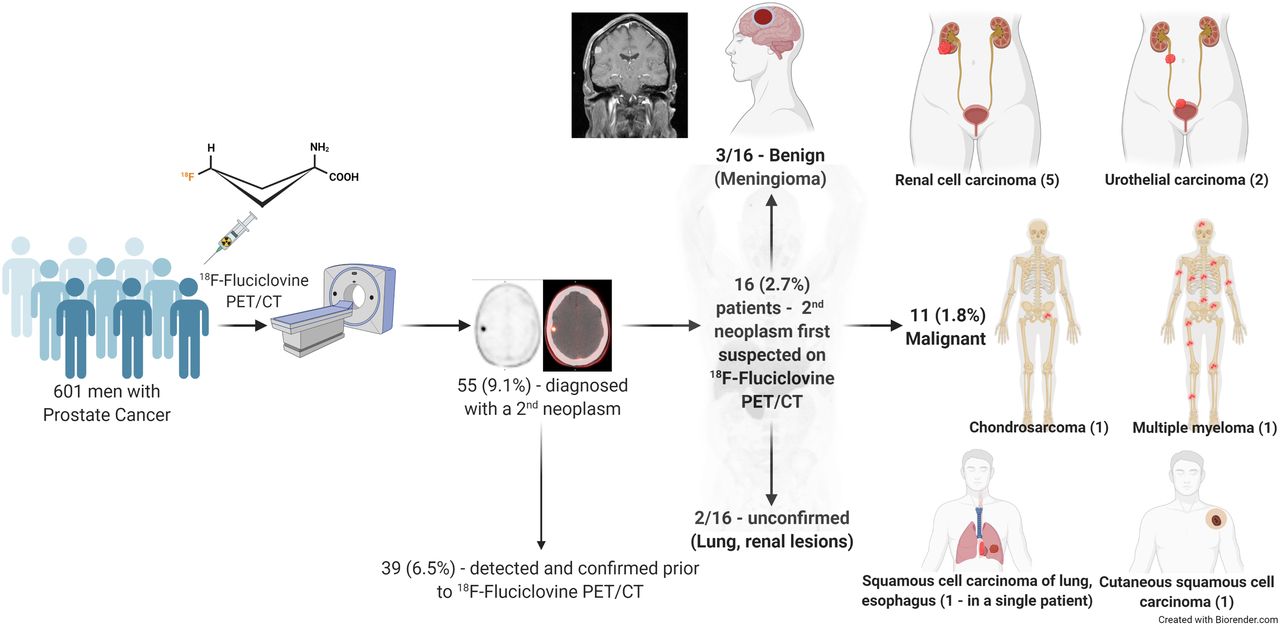
The aim of this study was to evaluate the detection rate of incidental second primary neoplasms in patients with prostate cancer on 18F-fluciclovine PET/CT. Methods: Imaging reports and patient demographic data were retrospectively reviewed from 663 clinical 18F-fluciclovine PET/CT studies, performed in 601 patients for the assessment of their prostate cancer (643 – recurrence evaluation, 20 – initial staging) from August 2016 to April 2021. Maximum SUV (SUVmax) of the suspected second neoplasms was determined. The results of 18F-fluciclovine PET/CT were correlated with clinical and radiologic studies to determine the nature of the suspected second neoplasms. Results: Fifty-five patients (9.1%) had findings suggestive of a second neoplasm. Thirty-nine of 55 had a known second neoplasm diagnosed before the PET/CT. An incidental second primary neoplasm was first suspected on 18F-fluciclovine PET/CT in 16 of 601 patients (2.7%). Three of the 16 patients had PET/CT suggestive of a meningioma that was corroborated on MRI. Of the remaining 13 patients, 11 had a tissue diagnosis confirming a malignancy. Second malignancies included renal cell carcinoma (RCC; 5/11; 45.5%), urothelial carcinoma (n = 2), multiple myeloma, chondrosarcoma, cutaneous squamous cell carcinoma, and squamous cell carcinoma of the esophagus and lung (n = 1, each; except for 1 patient with both esophageal and lung carcinomas). Among histopathologically confirmed malignancies, clear-cell RCC had the lowest uptake (SUVmax 3.4), and cutaneous squamous cell carcinoma had the highest uptake (SUVmax 13.6). Of the 2 patients with no histopathologic confirmation, 1 had ultrasound and MRI findings corroborating the diagnosis of RCC. The other patient had a solitary lung nodule suggestive of primary lung carcinoma and elected to undergo observation. Conclusion: Incidental findings consistent with a second primary neoplasm are not infrequently seen on 18F-fluciclovine PET/CT performed for assessment of prostate cancer (9.1%). Of the incidentally detected primary cancers, RCC was the most common (45.5%). These findings indicate the need for a careful analysis of 18F-fluciclovine PET/CT images, due to the broad tumor imaging capabilities of this radiotracer.
Anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid (18F-fluciclovine) is a radiolabeled, synthetic amino-acid analog that was initially developed for the evaluation of cerebral gliomas, mainly because of its negligible uptake in the normal brain parenchyma (1). The uptake of 18F-fluciclovine is mediated by the amino-acid transporters, primarily by the sodium-dependent alanine-serine-cysteine transporter-type 2, ASCT-2, along with the sodium-independent large neutral amino-acid transporter-type 1, LAT-1 (2). The uptake of 18F-fluciclovine was incidentally noted in primary and metastatic sites of prostate cancer, leading to further studies and subsequent U.S. Food and Drug Administration approval of 18F-fluciclovine for suspected recurrence of previously treated prostate cancer (3).
The amino-acid transporters are overexpressed in several malignancies because of the increased nutrient demands of the cancer cells (4). The overexpression of amino-acid transporters formed the basis of exploring the role of 18F-fluciclovine PET/CT in nonprostate malignancies such as breast and lung cancers, renal cell carcinoma (RCC), and gliomas (5–8). The detection of additional primary neoplasms on 18F-fluciclovine PET/CT has several implications. First, the understanding that most, if not all, radiotracers are nonspecific to a single cancer type, alerts the reader to the possibility of a second neoplasm when the pattern of disease involvement is discordant with the primary malignancy. Second, raising the suspicion of an additional neoplasm can prompt further investigations, including laboratory workup, imaging, and where appropriate, tissue analysis. Third and most importantly, identification of a second neoplasm can lead to significant changes in management, and prognosis—both in the case of a benign diagnosis, where the management of the primary malignancy can change to a less radical one (especially when the second lesion is the solitary suspected metastatic site) and in the case of a malignant diagnosis, where the treatment would need tailoring to fit in the second malignant diagnosis (and possibly an associated worsening of prognosis) (9).
Several single-case reports and short case series have documented the uptake of 18F-fluciclovine PET/CT in multiple nonneoplastic, and nonprostate neoplastic (benign and malignant) entities (10,11). This nonspecificity to a single cancer type is not unique to 18F-fluciclovine but is an attribute of most radiopharmaceuticals. Previous studies have described the detection of second primary neoplasms with 18F-FDG, 18F-choline, 68Ga-prostate-specific membrane antigen (PSMA), and several other radiotracers (12–16). In the absence of a planned prior study in this space, we performed the present study to evaluate the detection rate of additional primary neoplasms in patients with prostate cancer on 18F-fluciclovine PET/CT.
MATERIALS AND METHODS
Imaging reports and patient demographic data from 663 clinical 18F-fluciclovine PET/CT studies, performed in 601 patients for the assessment of their prostate cancer (643, recurrence evaluation; 20, initial staging) from August 2016 to April 2021, were retrospectively reviewed for the diagnosis of a second neoplasm. The timeline of PET/CT and clinical/laboratory/other imaging studies was reviewed to ascertain the previously unknown neoplasms that were incidentally detected on 18F-fluciclovine PET/CT. PET/CT images of these patients with incidentally detected second neoplasms were reviewed, and regions of interest were drawn to determine the maximum SUV (SUVmax) of the suspected lesions and average SUV (SUVmean) of the blood pool (descending thoracic aorta) and bone marrow (L3 vertebra; L2 vertebra if L3 had disease involvement) for comparability. The results of 18F-fluciclovine PET/CT were correlated with clinical and radiologic studies to determine the nature of the suspected second neoplasms. The study was approved by the institutional review board, and the need for written informed consent was waived.
RESULTS
Fifty-five of the 601 patients (9.1%) were diagnosed with a second neoplasm, at any time during their disease course, of which 39 had the diagnosis established before the 18F-fluciclovine PET/CT (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org). An incidental second primary neoplasm was first suspected on 18F-fluciclovine PET/CT in 16 of 601 patients (2.7%), with all 16 studies being performed for recurrence evaluation. Patient and imaging characteristics and management of the second neoplasms are shown in Table 1. Three of the 16 (18.7%) patients had 18F-fluciclovine PET/CT results suggestive of a meningioma (Supplemental Fig. 1) that was corroborated on MRI. Of the remaining 13 patients, 11 had a tissue diagnosis confirming a malignancy. Second malignancies included RCC (n = 5; Fig. 1), urothelial carcinoma (n = 2; Fig. 2), multiple myeloma, chondrosarcoma, cutaneous squamous cell carcinoma, and squamous cell carcinoma of the esophagus and lung (n = 1, each; except for 1 patient with both esophageal and lung carcinomas – Fig. 3). Among histopathologically confirmed malignancies, clear-cell RCC had the lowest uptake (SUVmax 3.4; SUVmean blood-pool 1.3; SUVmean bone-marrow 2.4), and cutaneous squamous cell carcinoma had the highest uptake (SUVmax 13.6; SUVmean blood-pool 1.8; SUVmean bone-marrow 5.6) (Fig. 4). Of the 2 patients with no histopathologic confirmation (Table 1, patients 1 and 2), 1 had ultrasound and MRI findings corroborating the diagnosis of RCC. The other patient had a solitary lung nodule suggestive of primary lung carcinoma and elected to undergo observation.
Incidentally Detected Neoplasms on 18F-Fluciclovine PET/CT: Patient and Imaging Characteristics
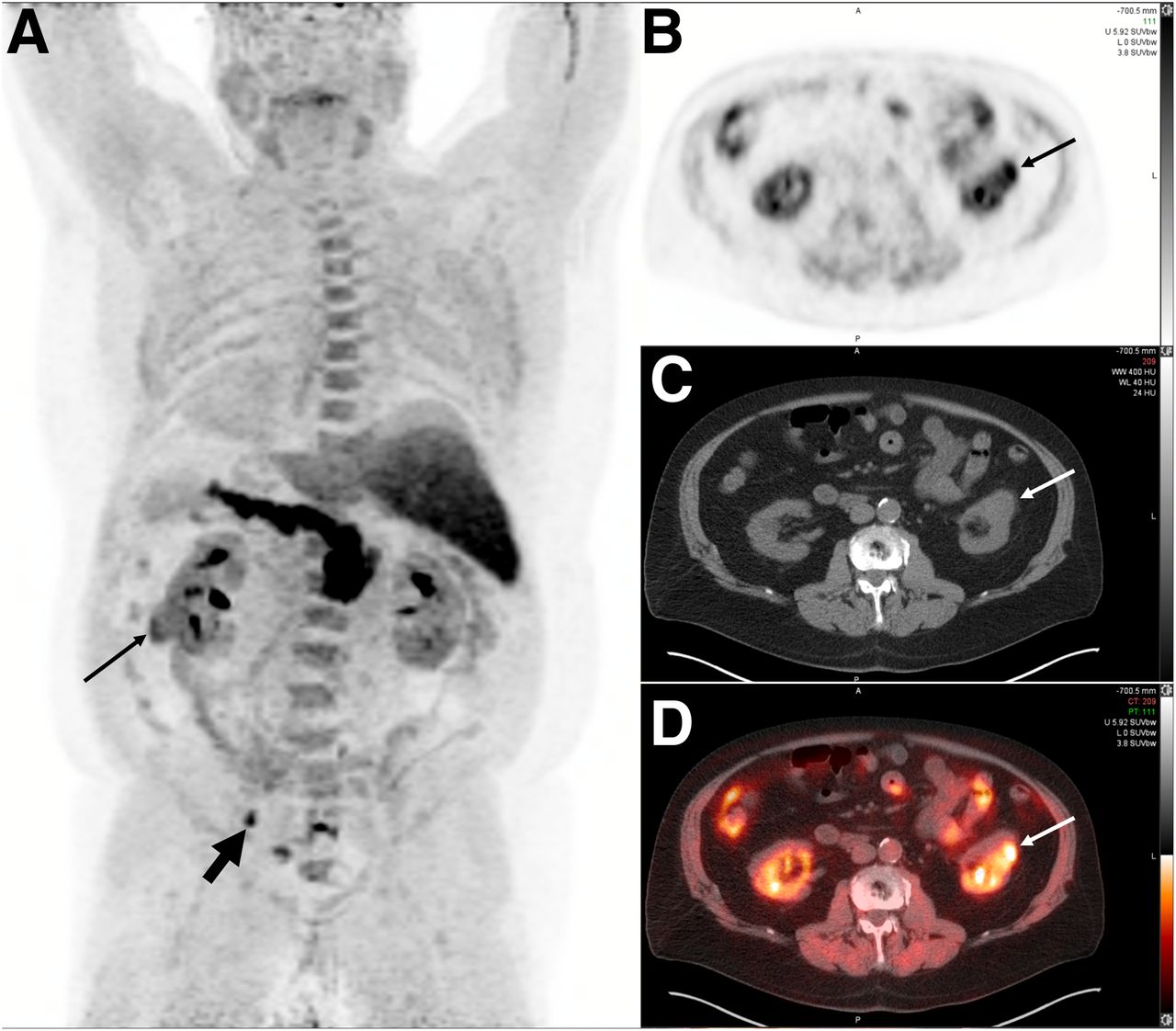
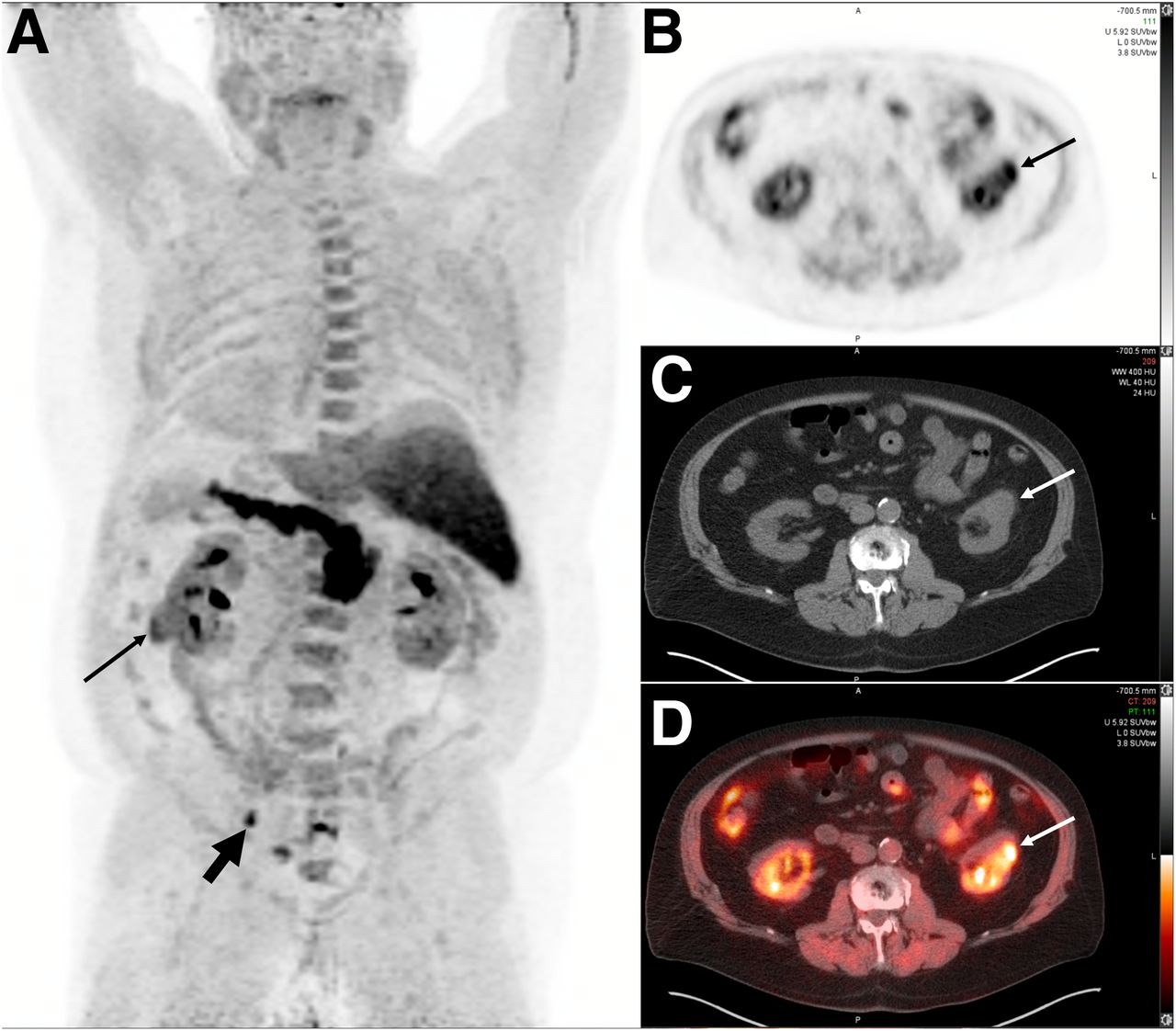
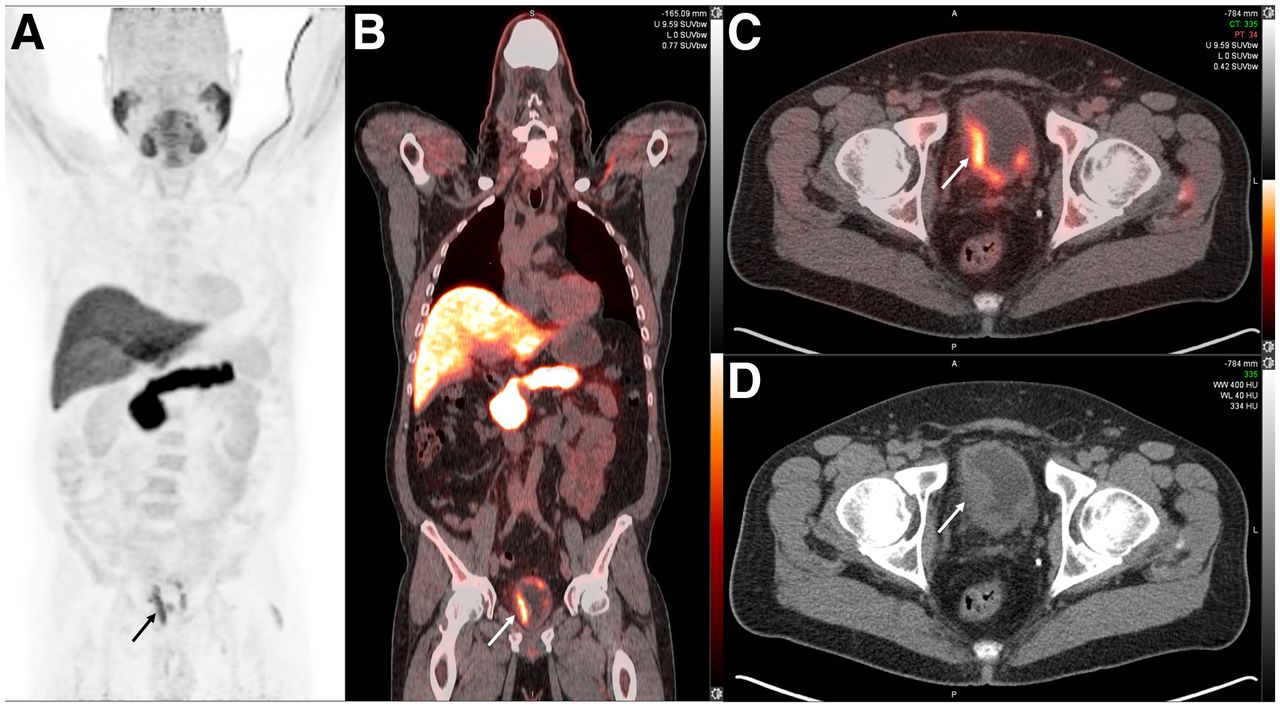
A 74-y-old man with adenocarcinoma of the prostate (Gleason score 4 + 3 = 7) after radical prostatectomy 19 y earlier presented with rising PSA (6.7 ng/mL). 18F-fluciclovine PET/CT performed for restaging of biochemical recurrence showed intensely tracer avid left external iliac lymph node (thick arrow; maximum-intensity-projection image in posterior view [A]) likely suggesting metastatic prostate carcinoma. Additionally, a tracer-avid (SUVmax 6.2) exophytic soft-tissue mass was noted in lower pole of left kidney (thin arrows; transaxial PET [B], CT [C], fused PET/CT [D]) that raised suspicion for primary renal malignancy. Patient underwent laparoscopic left partial nephrectomy, and histopathologic diagnosis was clear-cell RCC. PSA = prostate-specific antigen.
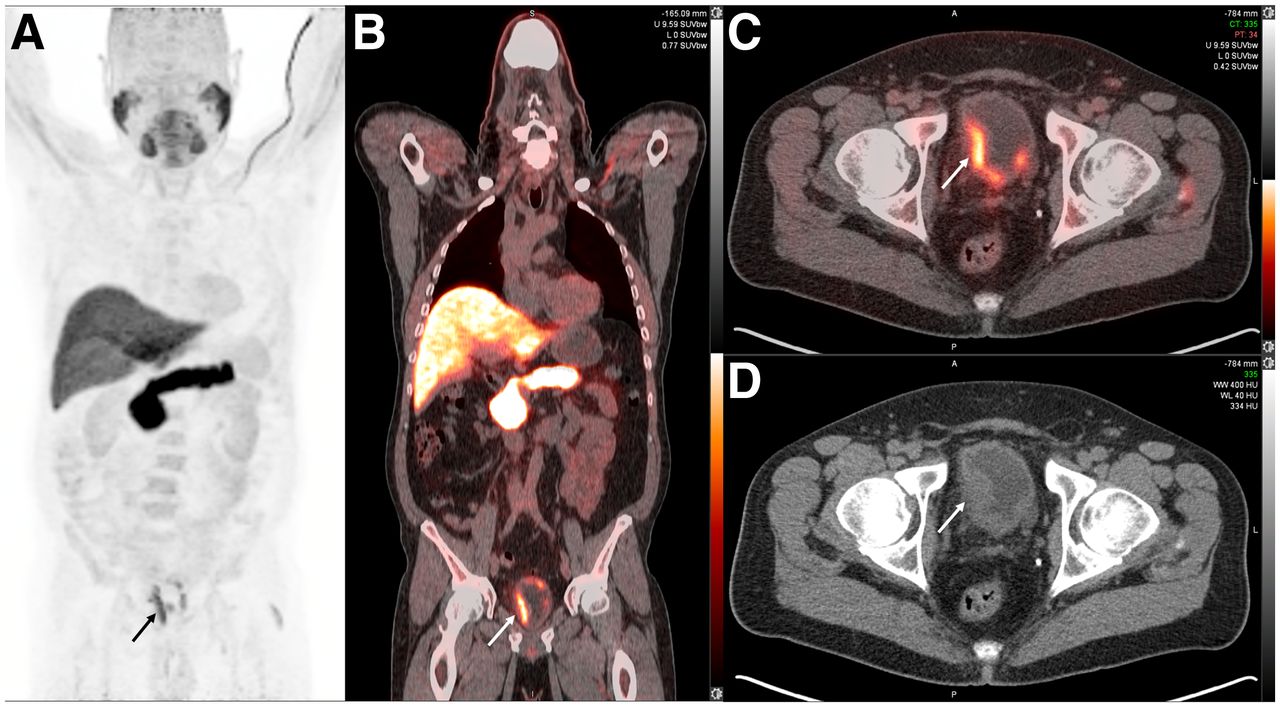
A 63-y-old man with adenocarcinoma of the prostate (Gleason score 4 + 3 = 7) after radical prostatectomy 7 y earlier presented with rising PSA levels (0.93 ng/mL). 18F-fluciclovine PET/CT performed for restaging of biochemical recurrence showed multifocal tracer-avid (SUVmax 9.8) soft-tissue nodules in wall of urinary bladder (arrow; maximum-intensity-projection image [A], coronal fused PET/CT [B], transaxial fused PET/CT [C], and CT [D]). Transurethral resection of nodules was performed, and histopathology showed high-grade papillary urothelial carcinoma. Patient was started on intravesical BCG (Bacillus Calmette–Guérin) therapy. PSA = prostate-specific antigen.

A 77-y-old man with adenocarcinoma of the prostate (Gleason score 4 + 3 = 7) after radical prostatectomy 4 y earlier with subsequent biochemical failure (15.4 ng/mL). 18F-fluciclovine PET/CT performed for restaging of biochemical recurrence showed tracer-avid presacral lymph node (dashed arrow; maximum-intensity-projection image in posterior view [A]) suggestive of metastatic prostate cancer. Additionally, linear increased tracer uptake (SUVmax 9.2) was noted in asymmetric mural thickening involving mid and distal esophagus (solid thick arrows [A], transaxial fused PET/CT [B], and CT [C]) and a soft-tissue nodule (SUVmax 3.4) in superior segment of right lung lower lobe (solid thin arrows [A], transaxial fused PET/CT [D], and CT [E]). Biopsy of esophageal lesion showed squamous cell carcinoma and biopsy of lung lesion showed distinct squamous cell carcinoma (not metastasis from esophageal primary). This patient was thus diagnosed with 3 distinct primary malignancies (prostate, esophagus, lung) with ongoing disease activity. Patient was started on carboplatin-based chemotherapy and external-beam radiation therapy.

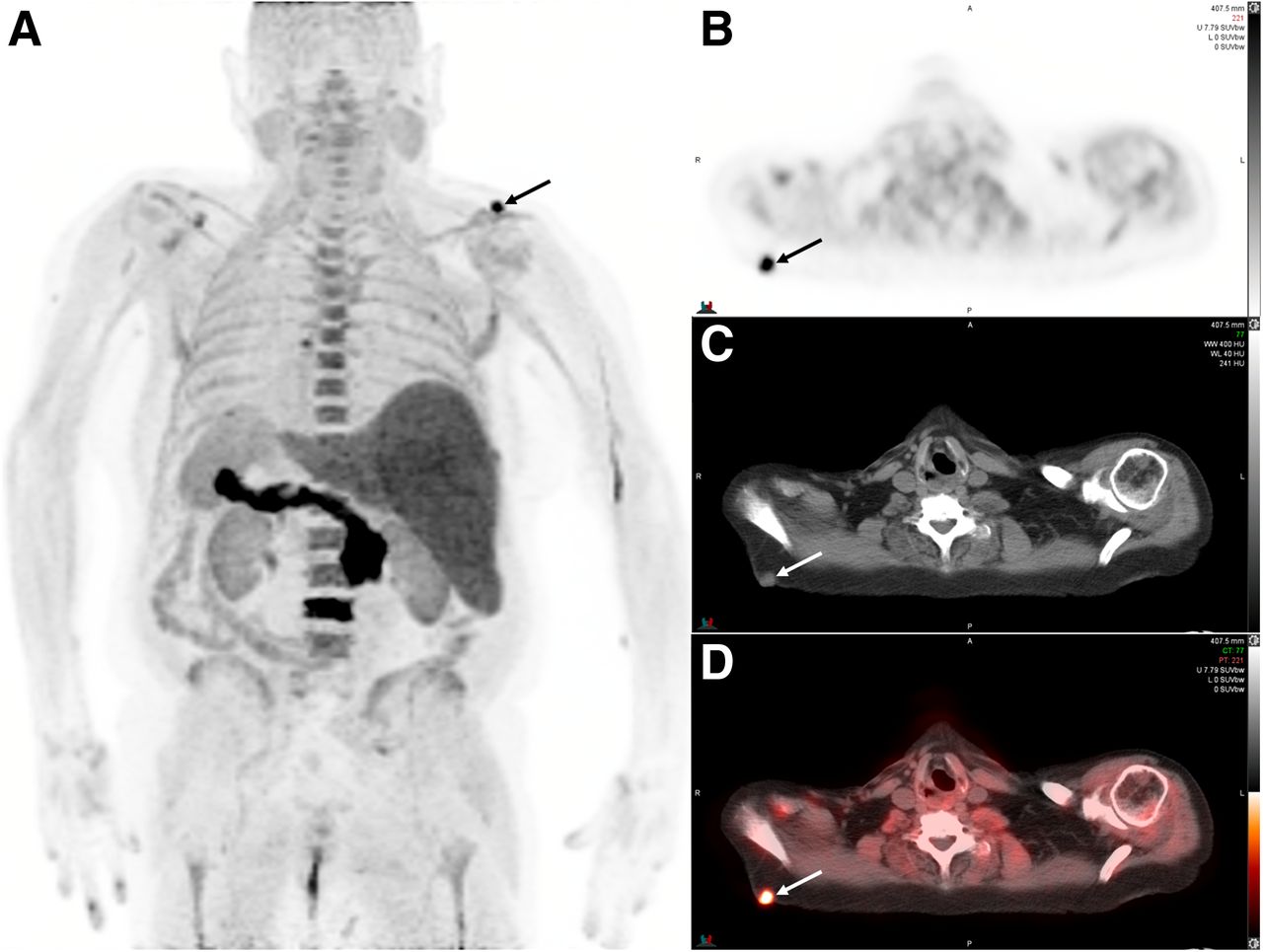
A 72-y-old man with adenocarcinoma of the prostate (Gleason score 5 + 5 = 10) after intensity-modulated radiation therapy to pelvis and prostate 3 y earlier and currently on hormonal therapy presented with increasing PSA levels (2.7 ng/mL). 18F-fluciclovine PET/CT performed for restaging of biochemical recurrence showed multiple osseous lesions suggestive of metastatic disease and markedly tracer-avid (SUVmax 13.6) subcutaneous soft-tissue nodule in posterior right shoulder region (arrows; maximum-intensity-projection image in posterior view [A], transaxial PET [B], CT [C], fused PET/CT [D]), which is an atypical site for metastatic prostate cancer. Subsequent biopsy of soft-tissue lesion was performed, and histopathology showed poorly differentiated squamous cell carcinoma. Patient underwent complete excision of lesion. PSA = prostate-specific antigen.
All the 11 patients with a tissue diagnosis confirming a malignancy had a significant change in management with regards to standard treatment for prostate cancer (Table 1), with the majority (7/11; 63.6%) undergoing a primary surgical treatment with/without additional medical therapy.
DISCUSSION
Overall, 55 (9.1%) of 601 prostate cancer patients who underwent 18F-fluciclovine PET/CT had a second neoplasm (48, malignant; 7, benign) detected at any time during the disease course, and 2.7% had a neoplasm that was first suspected on the PET/CT study. A Surveillance, Epidemiology, and End Results Medicare registry–based study of patients with prostate cancer treated with localized therapy showed that 9.9% patients had a second malignancy diagnosed after prostate cancer. The most common second malignancy was that of the lungs and bronchus (1.8%), followed by that of the urinary bladder (1.1%) (17). Among the 601 patients in the present study, a urinary bladder carcinoma (n = 12; ∼2%) was the most common second malignancy diagnosed at any time during their disease course (11, before PET/CT; 1, on PET/CT), whereas RCC was the most common second malignancy first detected on PET/CT.
The detection of a second neoplasm on 18F-fluciclovine PET/CT has several important implications. About 1 in 12 patients diagnosed with one of the common cancers develops a second malignancy, and mortality in approximately 55% patients is because of the second malignancy (18). The diagnosis of a second malignancy can often lead to a drastic change in the overall prognosis, morbidity, and mortality parameters and necessitates a change of the management (Table 1). It is important to consider the reader’s experience in interpreting PET/CT studies with a specific radiotracer. Experienced readers categorizing incidental findings as requiring further workup have a high probability of detecting a second neoplastic entity. A study of 1,727 patients with 18F-FDG PET/CT showed that actively investigated extrathyroidal lesions based on the readers’ recommendations were subsequently confirmed as neoplastic in more than 60% patients (19). In this context, knowledge of the common second malignancies detected with 18F-fluciclovine PET/CT can help the readers in being aware and facilitating additional investigations whenever appropriate. The uptake of 18F-fluciclovine has been demonstrated in several physiologic and pathologic processes. Table 2 summarizes the previously described 18F-fluciclovine–avid nonprostate pathologies on PET/CT, including benign, malignant, and nonneoplastic entities.
18F-Fluciclovine Uptake in Nonprostatic Disease Sites: Review of Published Literature
PET imaging is used to target specific components of the tumor microenvironment, such as metabolic handling of various substrates (e.g., glucose, amino acids, fatty acids) by the tumor cells, hypoxia, perfusion, angiogenesis, expression of receptors on the cell membrane, proliferation, apoptosis, and nontumor immune cells among others (20–23). The premise of targeted PET/CT imaging is based on the typical microenvironment and preferential metabolic features of different tumor lineages. It is known that a wide variety of tumors overexpress ASCT2 and LAT1 transporters because of their high nutritional demands. Glutamine and leucine, transported by ASCT2 and LAT1, respectively, contribute to the anaplerotic pathways feeding the Krebs cycle. The expression of LAT1 is also upregulated by hypoxia inducible factor HIF2α and the oncogene c-Myc (4). Because ASCT2 and LAT1 are involved with both influx and efflux of amino acids, the intratumoral retention of 18F-fluciclovine, and subsequent tumor detection, is dependent on the regional blood flow (for tracer delivery) and the relationship among the active amino acid transporters, yielding either a net influx or efflux of the radiotracer.
A lesion in an atypical location for the metastatic pattern of prostate cancer, different tracer avidity with respect to the primary cancer, disease bulk not correlating with the tumor markers (prostate-specific antigen), and morphologic findings on CT can often act as indicators suggestive of a second neoplastic site. Figure 3 shows a patient with 3 concurrent malignancies for which the avidity of the esophageal and lung lesions was markedly distinct, pointing toward a possible separate origin of these 2 lesions; this separate origin was subsequently confirmed on histopathology.
In this regard, 18F-fluciclovine PET/CT, with the advantage of whole-body survey, can act as an indirect screening modality for second malignancies in these patients, especially in those who are already at a higher risk due to familial, genetic, or environmental predispositions (24). The confirmation of a second benign neoplasm is also helpful as these lesions might be suspected for metastatic prostate carcinoma. In these cases, a knowledge of the benign neoplasms that are known to demonstrate avidity on 18F-fluciclovine PET/CT can be helpful (Table 2). Although the site and pattern of involvement can often point toward the possibility of a nonprostatic disease, the distinction between benign, malignant, and nonneoplastic entities might not always be straightforward. This is especially true of focal, tracer-avid lesions when the location and anatomic features are noncontributory in making a definitive diagnosis, and a tissue analysis is required. Conversely, diffuse tracer uptake in the lungs with obvious CT findings of pneumonia or diffuse tracer activity in an overactive muscle group can be easily interpreted.
Although the current literature does not have these data for 18F-fluciclovine PET/CT, a prior study on 18F-FDG PET/CT reported the detection rate of histopathologic proven second malignancy to be 1.2%, which is similar to 1.8% (11/601) in our study (12). Specifically in prostate cancer, 1.5% patients were reported to have a second malignancy on 11C-choline PET/CT, with primary lung carcinoma being the most commonly diagnosed (25). A study of 764 patients with prostate cancer reported the presence of a synchronous primary malignancy on 68Ga-PSMA-11 PET/CT in 5 (0.7%) patients (26). Of note, an additional 12 patients had suspicious lesions for which the final diagnosis was not reached. The relatively higher detection rate of second malignancies in our study could be attributed, at least in part, to the more ubiquitous expression of amino-acid transporters on tumor cells of different lineages, in comparison to PSMA. The most common incidentally detected second malignancy on 18F-fluciclovine PET/CT in the present study was RCC. A pilot study on the use of 18F-fluciclovine PET/CT in RCC found that most of the lesions had a low-grade tracer avidity, with the clear-cell variants showing tracer avidity equal to or less than the normal parenchyma whereas the avidity of 2 papillary RCC in a single patient was higher than the uptake in the background renal parenchyma (7). Four of the 5 histopathologically proven RCC in our study were clear-cell variants, with 2 of them showing avidity higher than the normal renal parenchyma (Fig. 2; SUVmax higher than the SUVmean of blood pool and bone marrow), which could be easily appreciated on the maximum-intensity-projection images. The single papillary RCC lesion had a lower tracer avidity, which notably has been shown to be relatively hypovascular on contrast CT studies in comparison to clear-cell RCC (27). The discrepancy of degree of tracer uptake between the different histologies of RCC may be better reviewed in prospective studies with a larger cohort. However, a distinct renal mass with any degree of avidity on 18F-fluciclovine PET/CT should raise suspicion and prompt further workup (7).
Meningioma was the only benign neoplasm first suspected on 18F-fluciclovine PET/CT (and confirmed on subsequent MRI), forming 18.7% of all 16 neoplastic entities. Prior studies have reported that approximately 2% patients with prostate cancer have an incidentally detected meningioma on 18F-fluciclovine PET/CT, forming one of the most common benign diagnoses (28). Meningiomas also show radiotracer uptake on somatostatin receptor imaging for neuroendocrine tumors, such as with 68Ga-tetraazacyclododecanetetraacetic acid-[1-Nal3]octreotide PET/CT, and on prostate cancer imaging with 68Ga-PSMA PET/CT (26,29). Meningiomas, especially when tracer-avid, can mimic metastases on a 18F-fluciclovine PET/CT (with non–contrast-enhanced CT), although the brain is a rare site for prostate cancer metastases (30). MRI of the brain is helpful in uncertain diagnoses.
One of the limitations of the present study is its relatively lower sample size in comparison to other similar studies performed with 18F-FDG PET/CT, although it is still the largest cohort reporting these findings on 18F-fluciclovine PET/CT. Another limitation is the retrospective design of the study, which did not permit review of all the imaging studies to identify the separate contributions of the PET and CT components. One of the main strengths of this study is the availability of tissue diagnosis or an MRI correlate in most of the patients with suspected second neoplasms. Future studies can be prospectively planned in a larger patient cohort, assessing possible factors (such as genotype, environmental factors, toxins) that could predispose to synchronous malignancies and identifying robust imaging-based features that can distinguish metastatic prostate cancer from second neoplasms, either benign or malignant.
CONCLUSION
18F-fluciclovine PET/CT identified a second neoplasm in 2.7% of the patients with prostate cancer, and 1.8% of all patients had a histopathologically confirmed second primary malignancy that was first detected on 18F-fluciclovine PET/CT. The most common second malignancy detected on 18F-fluciclovine PET/CT was RCC.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the detection rate of second neoplasms in patients with prostate cancer on 18F-fluciclovine PET/CT?
PERTINENT FINDINGS: In this retrospective study, we showed that 18F-fluciclovine PET/CT detected a second neoplasm in 2.7% of patients with prostate cancer. Of these, the histopathology yielded the diagnosis of a second malignancy in 68.7% patients; the most common diagnosis was RCC.
IMPLICATIONS FOR PATIENT CARE: The study shows that second neoplasms are not uncommon in patients with prostate cancer, and 18F-fluciclovine PET/CT can aid in their detection, which is vital for appropriate further management.
Footnotes
Published online Aug. 19, 2021.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 3, 2021.
- Revision received August 5, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.