


Abstract
59
Introduction: Head motion during a brain PET scan can cause motion blurring and loss of image quality. In this work we present a completely data-driven motion estimation approach with full event-by-event motion corrected list-mode (LM) reconstruction. A reader study and atlas-based quantitative analysis comparing the motion corrected (MoCo) and uncorrected (nMoCo) reconstructions were performed on 50 clinical FDG brain scans.
Methods: Ultra-fast LM reconstructions of very short frames (0.6 - 1.8 sec) were performed. Head motion was estimated using image registration [1]. Event-by-event motion corrected LM reconstruction was then performed on the entire acquisition. Normalization, deadtime, attenuation, scatter, and randoms corrections were performed during reconstruction. A cohort of 50 retrospective clinical metabolic FDG brain scans was obtained from 3 scanners: SIGNA PET/MR (n=21), DMI PET/CT (n=11), and D710 PET/CT (n=18) (GE Healthcare, Chicago, IL). Experienced readers evaluated the MoCo and nMoCo images in a blinded read using a Likert scale (1-5) for image sharpness and diagnostic quality. Atlas-based quantitation analysis was performed on the SUVmax values of 9 regions-of-interest (ROIs) [2]. Paired Wilcoxon tests were used to assess differences in reader scores and ROI-wise SUVmax. A Levene test was used to assess if the variance of the relative difference of MoCo and nMoCo was different between motion groups. Statistical tests were corrected for multiple comparisons.
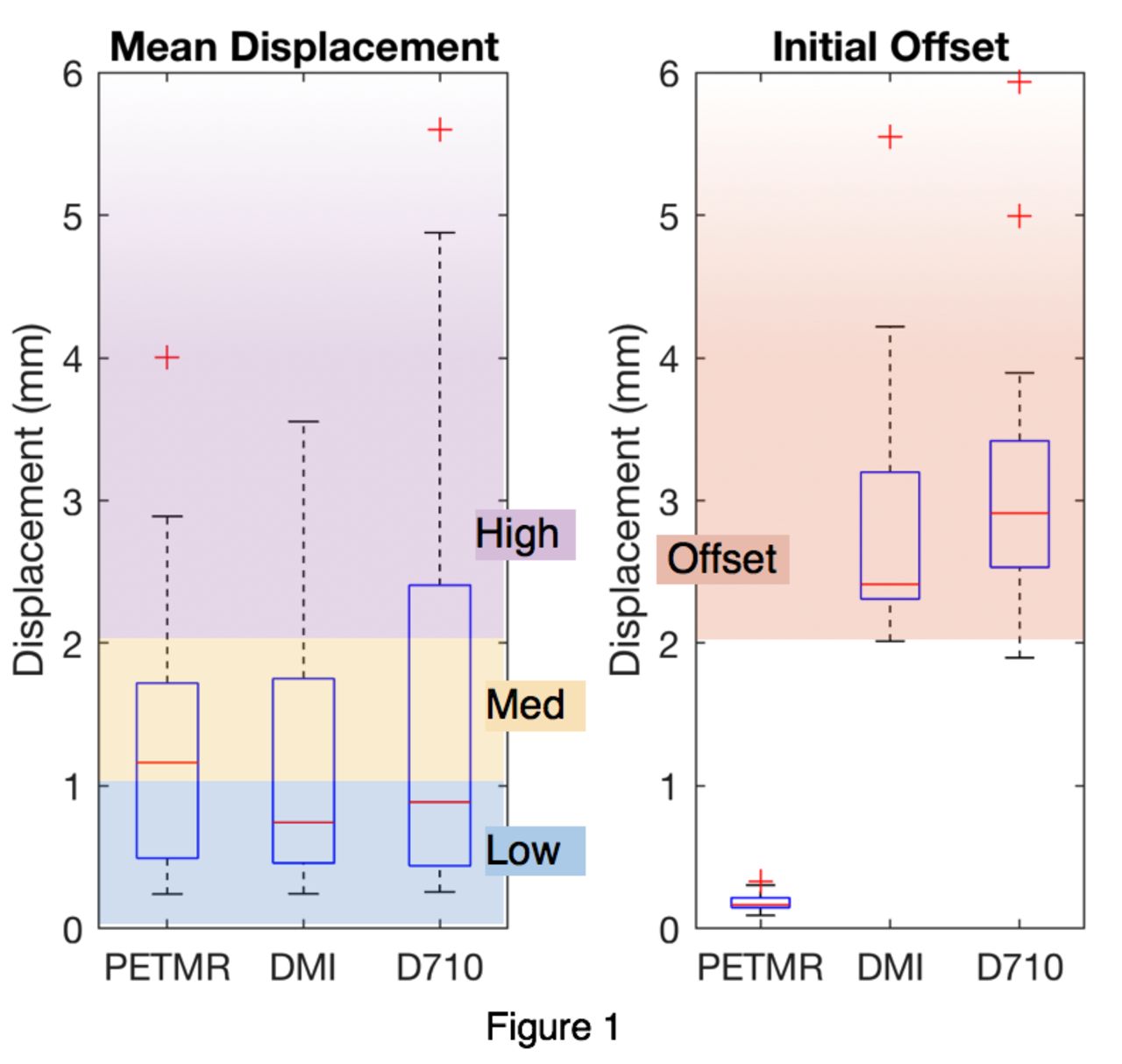
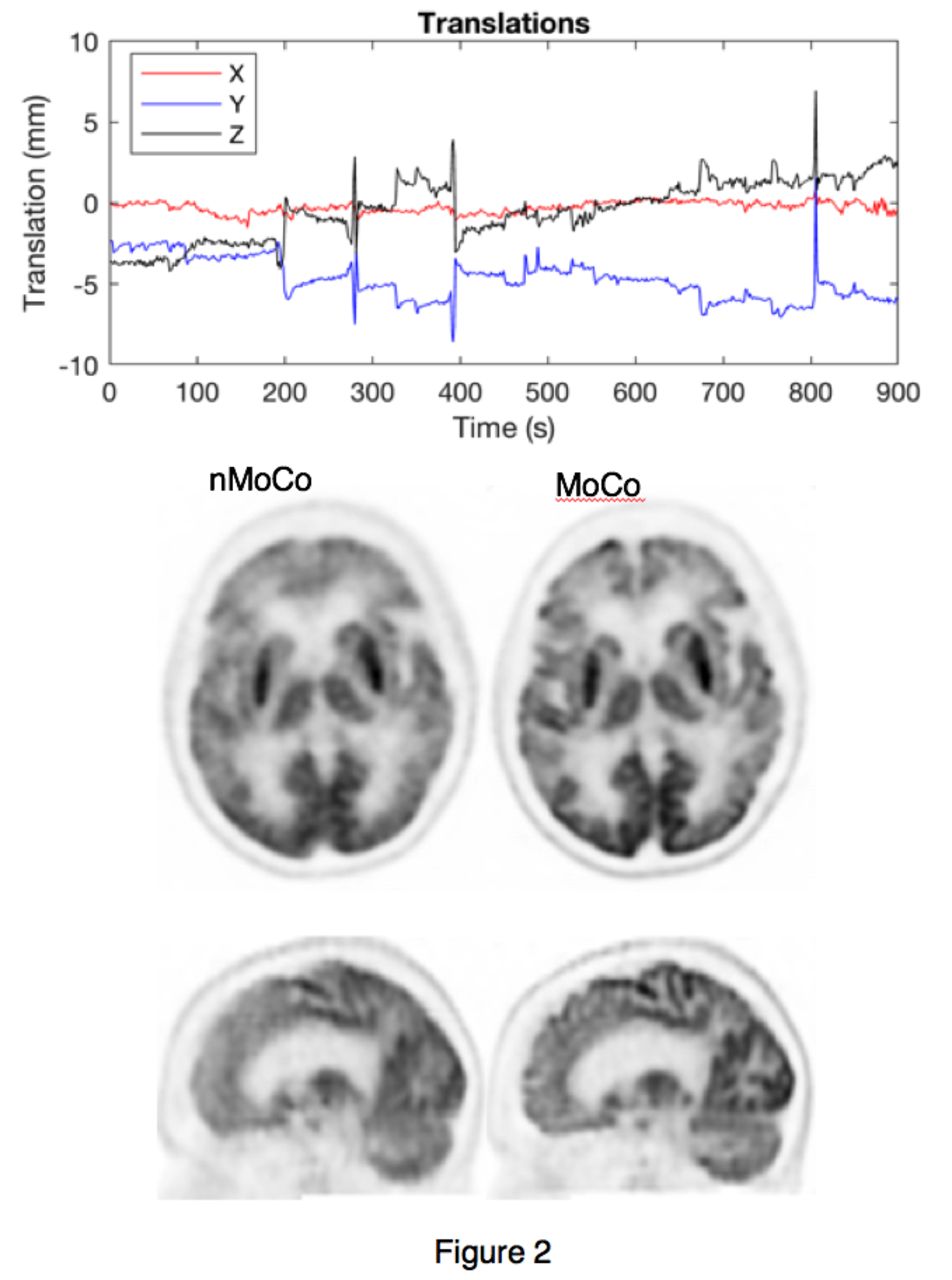
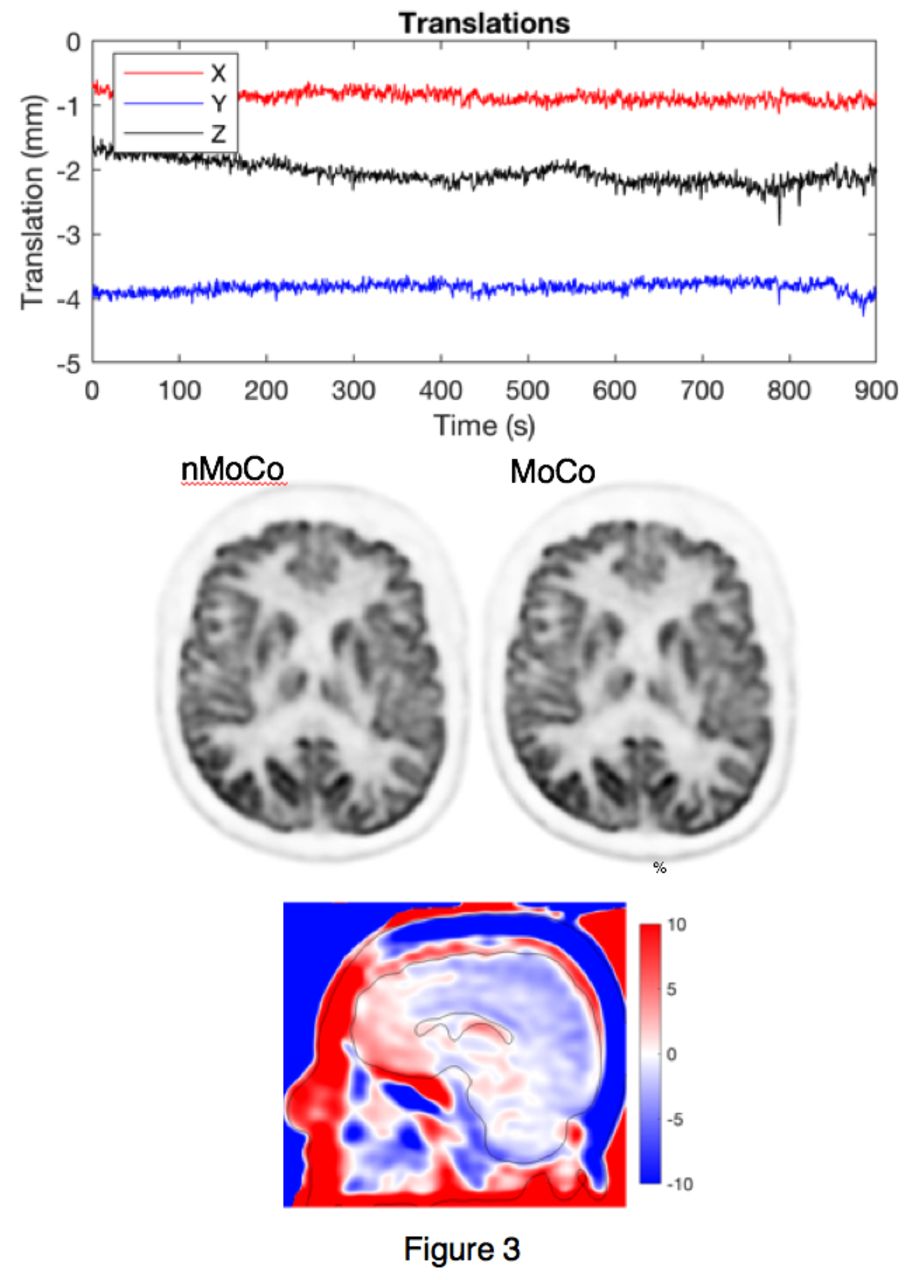
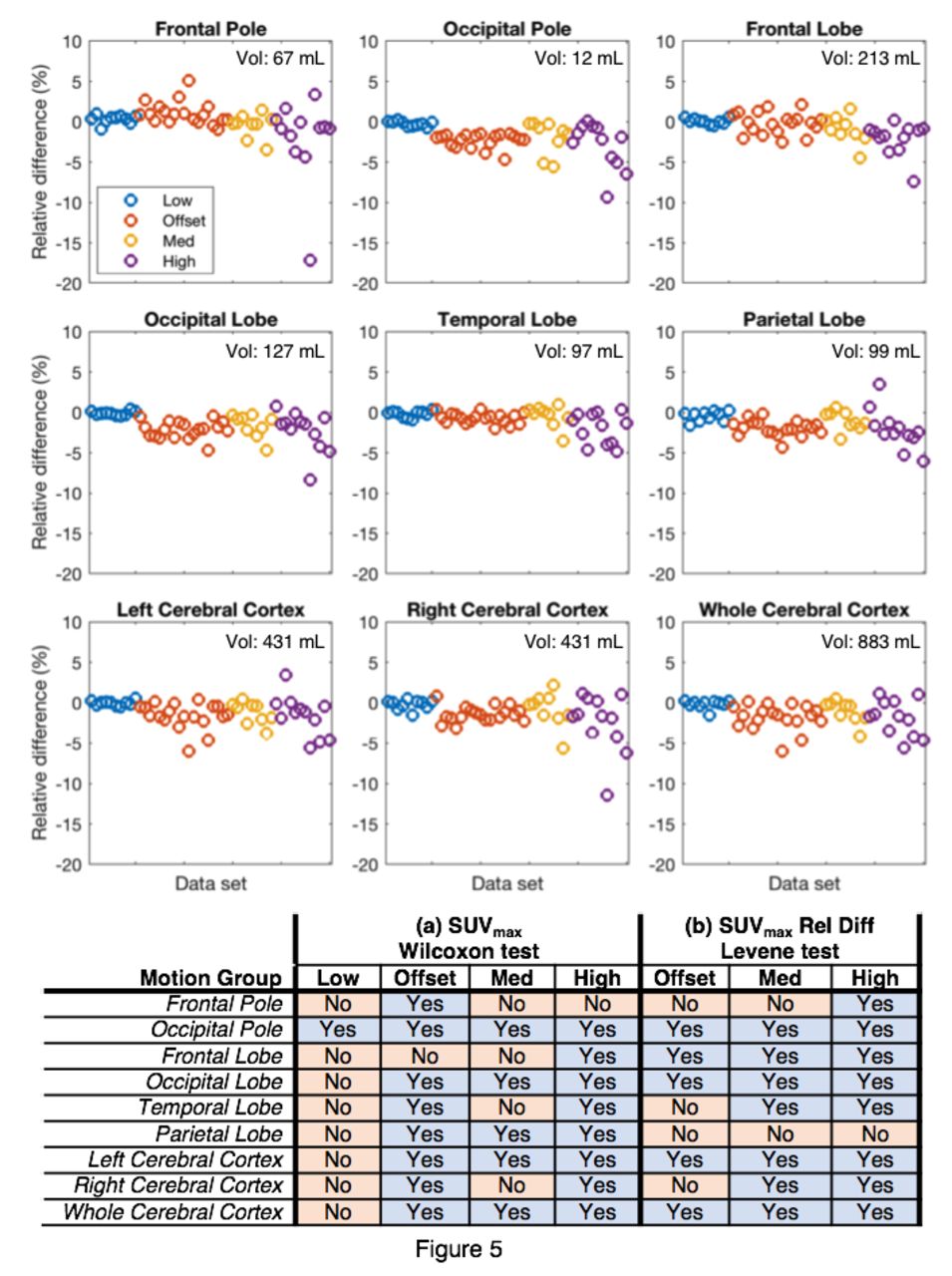
Results: The range of estimated motion in the cohort, as quantified by a point within the brain displaced by the motion, is shown in Figure 1. Figure 1 also shows how the cohort was divided into 4 motion groups. Figure 2 and 3 show examples of MoCo applied to 2 data sets. Figure 4 shows the results of the reader study. Figure 5 shows the results of the ROI analysis.
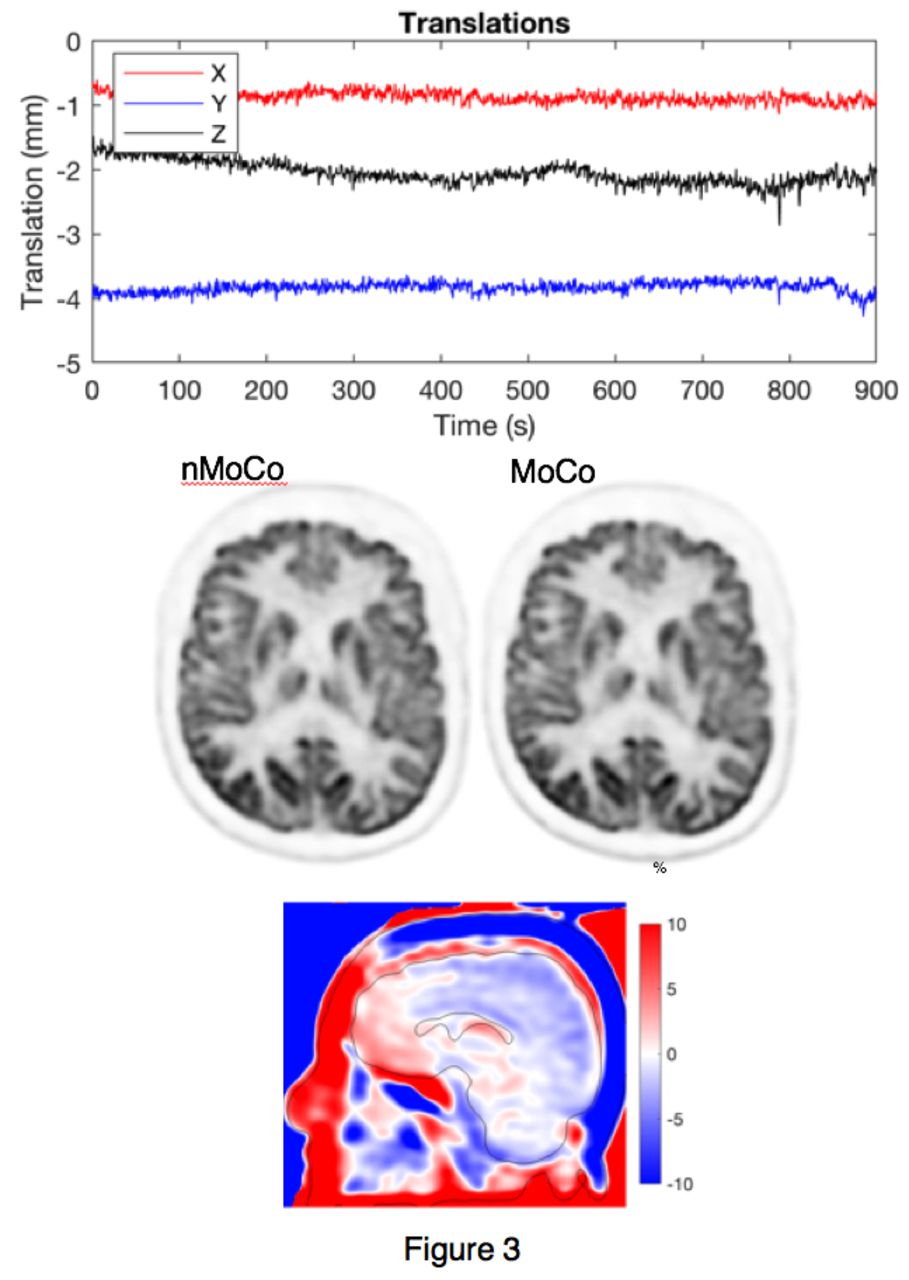
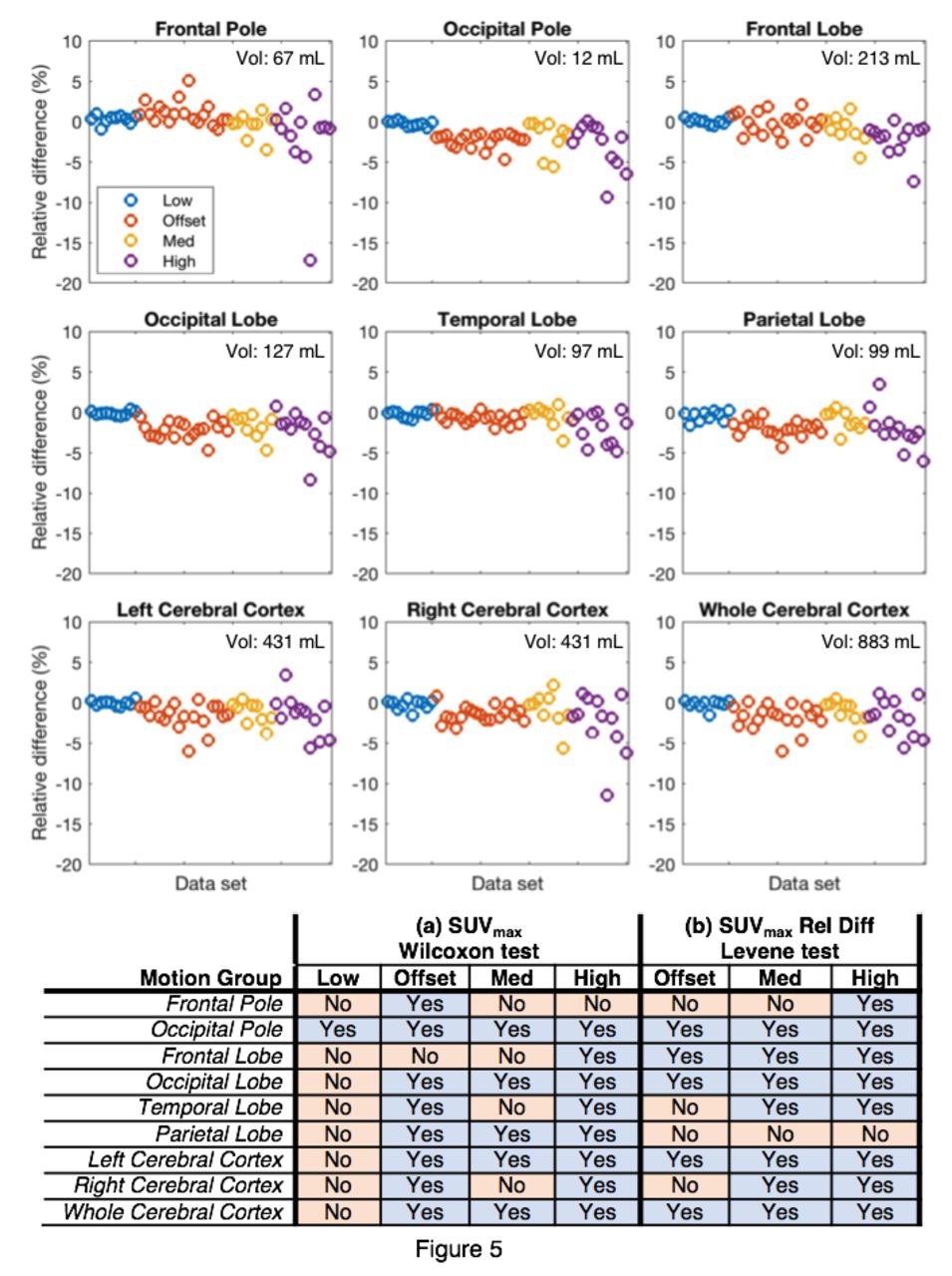
Conclusions: MoCo improved both quantitative and qualitive assessment of the images. Using an atlas-based approach we demonstrated that, when motion occurs, MoCo makes a significant difference in the quantitation of the reconstruction. The reader study demonstrated that MoCo improved diagnostic quality in 10% of the data sets, with 8% changing from diagnostically “unacceptable” to “acceptable” with MoCo. When there is little motion, MoCo reconstructions are not significantly different to the nMoCo reconstructions, as expected. The developed approach was completely data-driven, yielding motion estimates with ~1 Hz frame rate utilizing an event-by-event LM reconstruction, and is compatible with routine imaging workflows suggesting that motion-robust PET is clinically attainable. Fig. 1: (Left) Box plots of estimated motion. Shaded regions indicate motion groups: “Offset” includes low motion during the scan with an offset between PET and attenuation map of >2 mm. (Right) Initial offset between PET and attenuation map. Fig. 2: Example data set in the “High” motion group. (Top) Translations of the motion (rotations not shown). (Bottom) The nMoCo and MoCo images. The nMoCo image is visibly blurred. Fig. 3: Example data set in the “Offset” motion group. (Top) Translations of the estimated motion. (Bottom) The nMoCo and MoCo images, and a sagittal difference image showing a relative gradient. Fig. 4: Difference of the averaged reader scores between the MoCo and nMoCo images, grouped according to motion group for (Top) image sharpness and (Middle) diagnostic quality. (Bottom) Significant differences in sharpness and quality for MoCo and nMoCo reconstructions were found for the “High” motion group and the pooled cohort data (“All”). Fig. 5: (Top) Relative differences between the SUVmax values of the MoCo and nMoCo images in 9 ROIs. (Bottom) Significant differences in SUVmax were present in many ROIs between the MoCo and nMoCo images. Similarly, the variance of the relative difference between MoCo and nMoCo was significantly different for many ROIs in the “Offset”, “Med”, and “High” motion groups compared to the “Low” motion group.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}