


Abstract
A diverse health-care workforce is a necessary component of equitable care delivery to an increasingly diverse U.S. population. In nuclear medicine (NM), there is a paucity of data on the numbers of women and members of racial and ethnic groups that are underrepresented in medicine in the United States (URiMs). This study sought to characterize the current state of women and URiMs in academic NM, describe the demographics of Accreditation Council for Graduate Medical Education (ACGME)–accredited NM residency program faculty and trainees, and assess the extent of NM exposure during medical school. Methods: This study was reviewed by the Institutional Review Board and deemed exempt. In this cross-sectional study, a link to an online 15-item survey was emailed to 41 ACGME-accredited NM residency program directors (PDs) in the United States. Data were collected between September 2018 and December 2018 using a secure web application that serves as an electronic data capture tool for research studies. Results: 23 of 41 (56.1%) PDs responded to the survey, 18 of 23 (78.3%) of whom were men and 5 of 23 (21.7%) women. Three of 23 (13.0%) PDs reported being URiMs. Of the 60 residents in the 23 NM residency programs whose PDs responded, 37 of 60 (61.7%) were men (7/37 [18.9%] URiMs) and 23 of 60 (38.3%) women (5/23 [21.7%] URiMs). Fourteen of 60 (23.3%) residents were U.S. medical school graduates (U.S. grads). PDs described demographics of 121 current NM faculty members: 86 of 121 (71.1%) were men (8/121 [6.6% URIMs] and 35 of 121 (28.9%) women (7/121 (5.8% URiMs). Sixty-five of 121 (53.7%) were U.S. grads. Sixteen of 23 (69.6%) divisional chiefs were men, and 7 of 23 (30.4%) were women. Four of 23 (17.4%) divisional chiefs were URiMs, and 7 of 20 (35.0%) NM PDs reported that NM was part of the medical school curriculum. Conclusion: Women and URiMs are underrepresented in NM training programs. This diversity gap is more pronounced among NM faculty and to an even greater extent in leadership positions. A greater proportion of NM trainees are international medical graduates compared with NM faculty members, suggesting declining NM recruitment among U.S. grads. NM is included in the medical school curriculum at fewer than one third of academic centers with NM residency programs, typically toward the end of medical school. Increased and earlier exposure to NM, especially for women and URiMs, may improve recruitment and mitigate diversity gaps.
A diverse health-care workforce is one of the essential components to the provision of equitable and culturally competent care to an increasingly diverse U.S. patient population (1,2). Shared traits between patients and physicians including gender and race or ethnicity have been linked to better communication, adherence to medical recommendations, and overall health-care outcomes (3,4). Previous research indicates that improving patient–physician concordance of race, language, and social characteristics increases patients’ trust of providers and satisfaction with care (5,6). The importance of a diverse workforce will only continue to increase in importance: U.S. Census projections indicate that racial and ethnic minorities will become the majority by the year 2050, with people of Hispanic ethnicity comprising 99.8 million people or 26% of the population (7), and people identifying as being of 2 or more races expected to become the fastest growing group over the next several decades (8).
Significant inequities in medical imaging have been documented, with individuals from racial and ethnic minority backgrounds disproportionately less likely to complete recommended imaging for both acute and chronic health conditions (9). For example, after adjusting for income, education, insurance, and health-care setting, Black people and people of Hispanic ethnicity in the Cancer Care Outcomes and Research Surveillance study population were less likely than non-Hispanic White people to receive guideline-recommended PET imaging during staging for non–small cell lung carcinoma, with potential adverse impacts on diagnosis accuracy and long-term survival (10). Other studies have reported that women are more likely to receive inappropriate SPECT myocardial perfusion imaging, suggesting a gender disparity in referral for this test (11).
Although women make up nearly half of U.S. medical school graduates, they remain underrepresented in numerous medical specialties and comprise a minority of faculty positions in academic medical centers, less than a third of division and section chiefs, and less than 20% of department chairs and medical school deans (12). Likewise, members of racial and ethnic groups that are underrepresented in medicine in the United States (URiMs), previously described as underrepresented minorities (13), are underrepresented as medical students (14), as medical school faculty members (15), and in medical school leadership positions (16).
There is a paucity of data on the representation of women and URiMs in nuclear medicine (NM). Although we know that women are underrepresented in radiology in the United States, comprising 27.2% of radiologists (17), women are likely even more underrepresented in NM as they comprise less than 20% of physicians certified by the American Board of Nuclear Medicine. Although female residents comprised 44% of NM residents in 2018 based on Association of American Medical Colleges (AAMC) statistics (12), there are limited data available on the range of representation of women and URiM residents in NM training programs across the country, the representation of women and URiMs among NM faculty, the percentage of international medical graduates in NM training programs, and board certification pathways for faculty and current residents. There are also limited data on exposure to NM in medical school, with only 1 study recently reporting that 80% of current NM trainees first became interested in NM after medical school (18). The authors of this study also found significant differences in perception of NM exposure in the medical school curriculum between the faculty and NM trainees. To address these knowledge gaps, we sought to:
1. Characterize the current state of women and members of URiM racial and ethnic groups in Accreditation Council for Graduate Medical Education (ACGME)–accredited NM residency training programs,
2. Describe the demographics of ACGME-accredited NM residency program faculty and trainees including years in practice, country of medical school education, board certification status of faculty, and board certification plans for residents, and
3. Identify the extent of NM exposure during medical school.
We expect that insights gained could inform future strategies to address diversity gaps in NM.
MATERIALS AND METHODS
This study was deemed exempt by our institutional review board with a waiver of informed consent, and compliance with the U.S. Health Insurance Portability and Accountability Act was maintained.
In this descriptive cross-sectional study, a link to a 15-item online survey was sent via email to program directors (PDs) of the 41 ACGME-accredited NM residency programs in the United States. The anonymous survey included questions about divisional faculty, leadership and resident characteristics including gender, race and ethnicity, and country of medical school graduation as well as medical school exposure to radiology and NM (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). Although URiM is an evolving concept, our survey defined URiM as Black/African American, American Indian/Alaska Native or Native Hawaiian/Pacific Islander, or Hispanic/Latinx based on U.S. Census Bureau race and ethnicity categories and historically underrepresented racial and ethnic groups in medicine (13). Respondents could opt out of any question they preferred not to answer; IP addresses were not collected, and no protected health information was obtained for this research project. Survey responses were collected between September and December 2018 and stored in REDCap (a secure web application that serves as an electronic data capture tool for research studies) until downloaded for analysis.
RESULTS
Twenty-three of the 41(56.1%) PDs supervising 60 residents in ACGME-accredited NM residency programs in the United States responded to the survey (Fig. 1). All survey responses were complete.

Flowchart of study participants.
Resident Demographics
The percentage of NM residents who are women and the percentage of NM residents who are members of URiM racial and ethnic groups (Fig. 2 and Table 1) are lower than their respective percentages in the general population (Table 2).
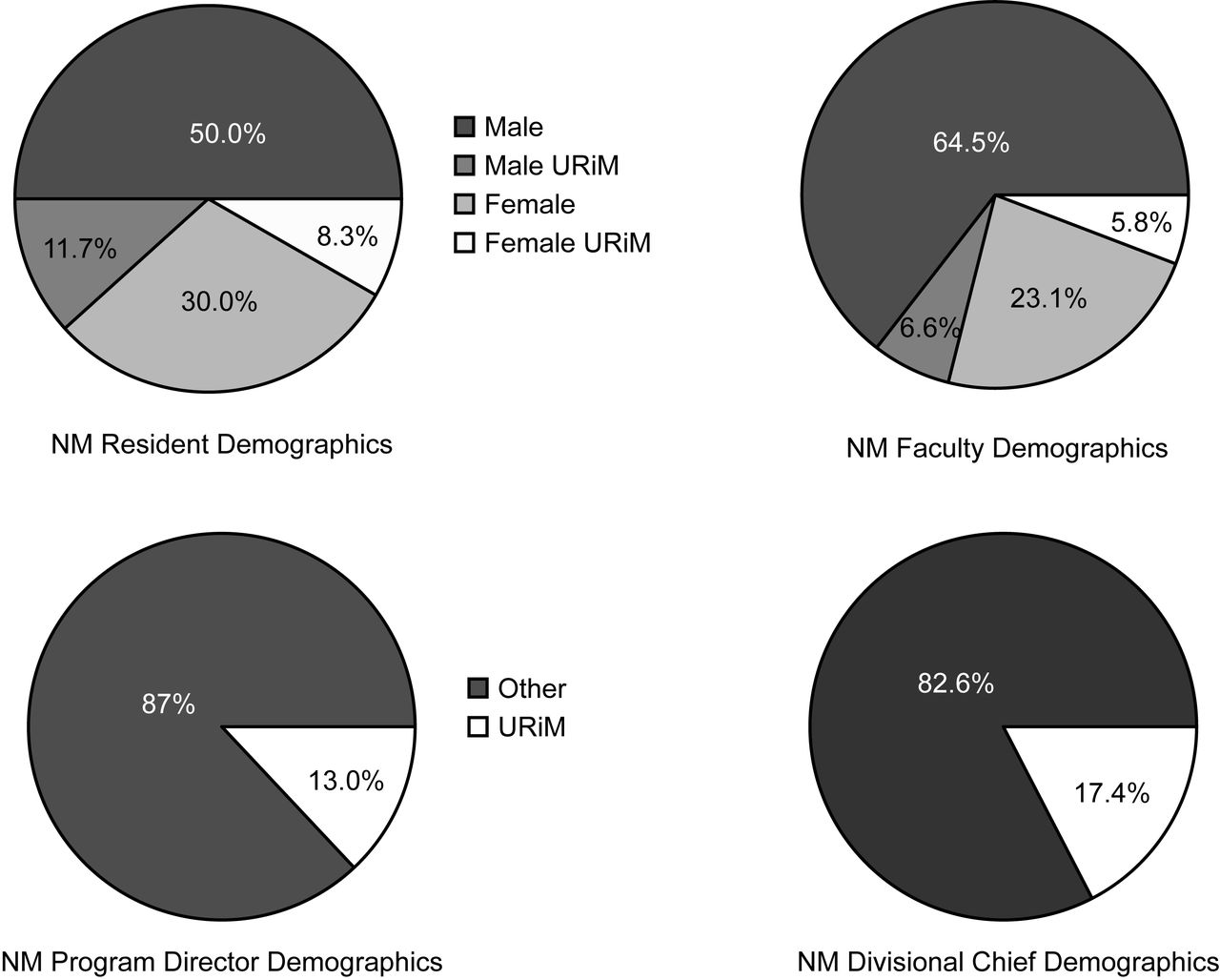
NM resident, faculty, program director, and divisional chief demographics.
Demographics of NM Residents and Faculty
Demographics of Residents, Faculty, and Department Chairs in Medicine and Demographics of U.S. General Population
Faculty Demographics
The percentage of current NM faculty members who are women and the percentage of NM faculty members who are members of URiM racial and ethnic groups (Fig. 2 and Table 1) are lower than their respective percentages in the general population (Table 2). This is also true at the leadership level (Fig. 2) where 5 of 23 (21.7%) PDs were women, 3 of 23 (13.0%) PDs reported being members of a racial or ethnic URiM group, 7 of 23 (30.4%) divisional chiefs were women, and 4 of 23 (17.4%) divisional chiefs were members of a racial or ethnic URiM group.
Figure 3 shows URiM representation in NM residents and faculty by gender.
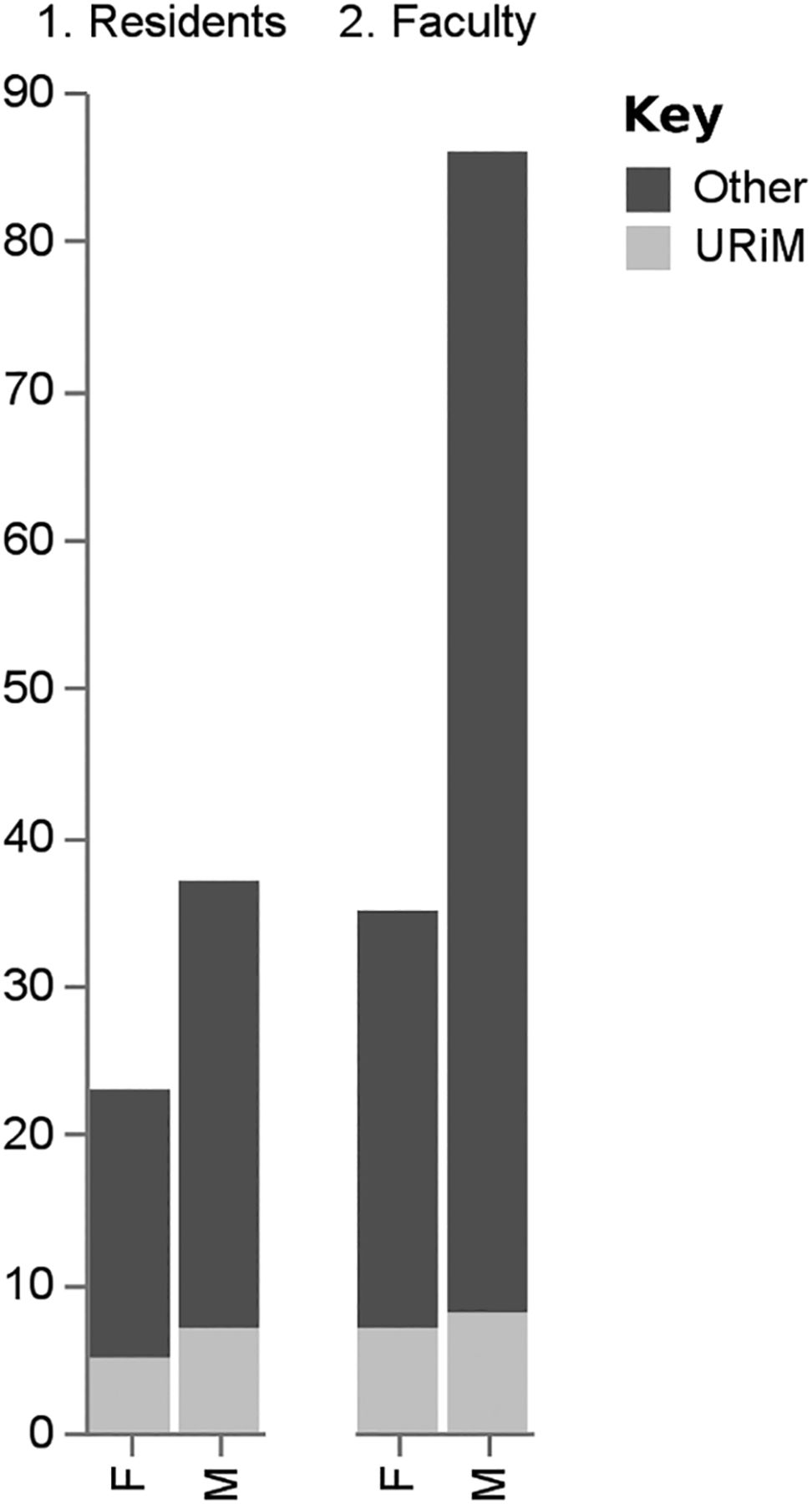
URiM representation in NM faculty by gender.
Training and Certification of Faculty Versus Residents
PDs described board certification status of 113 clinical NM faculty members. Of 113 NM faculty members, 2 of 113 (1.8%) were certified by the American Board of Radiology (ABR); 1 of 113 (0.9%) ABR plus subspecialty certification (ABR + CAQ); 61 of 113 (54.0%) American Board of Nuclear Medicine (ABNM); 41 of 113 (36.3%) ABR + ABNM; and 4 of 113 (3.5%) other (2 American Board of Internal Medicine [ABIM] + ABNM, 3 ABIM, 2 Certification Board of Nuclear Cardiology [CBNC], 1 European). Results are illustrated in Figure 4.
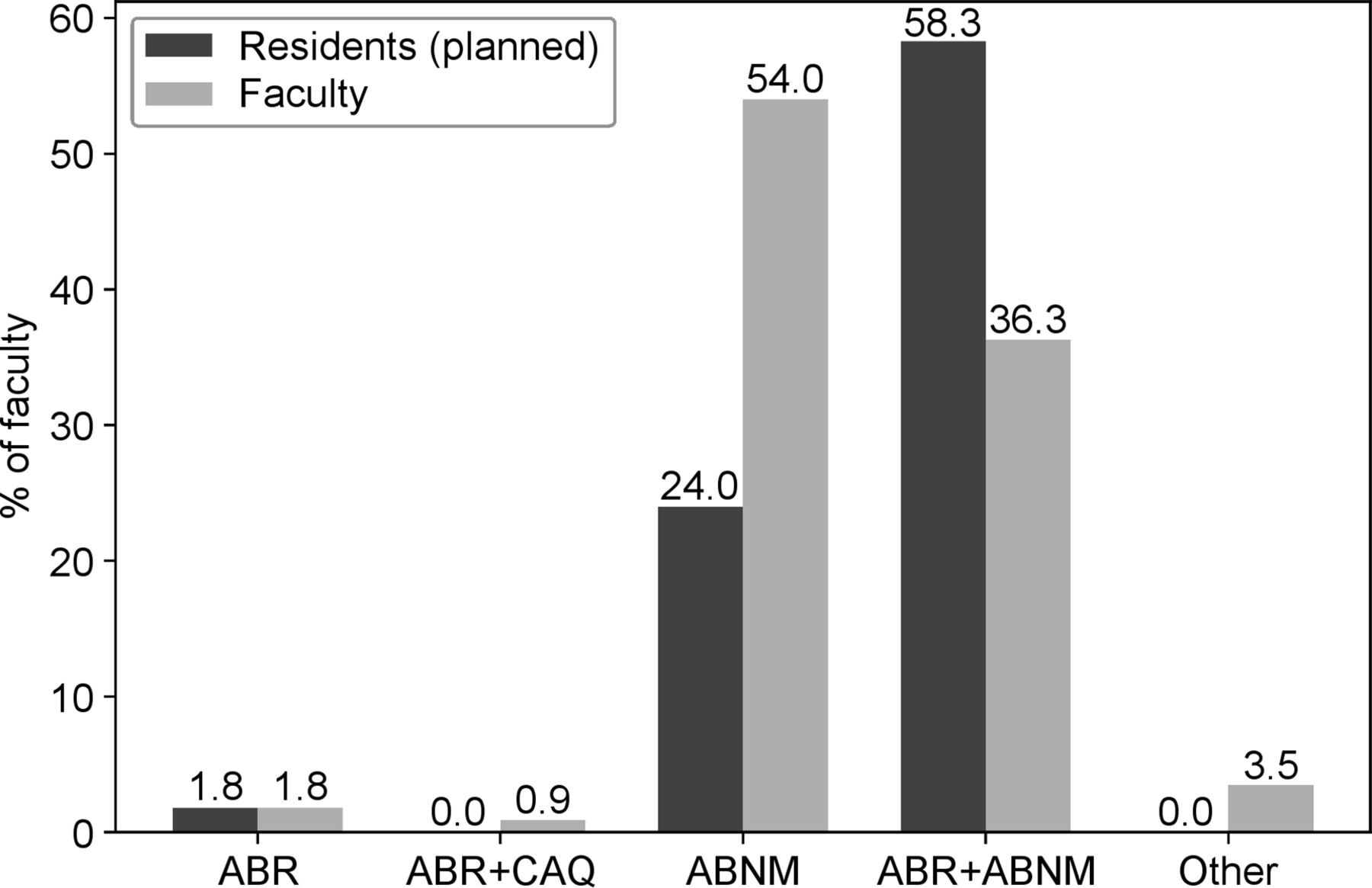
Board certification of 113 NM faculty at 23 training institutions.
PDs described country of graduation for 121 NM faculty members. The majority (65/121 [53.7%]) of NM faculty members graduated from medical school in the United States. PDs described experience of 137 clinical NM faculty members. Fifty-one of 137 (37.2%) had been out of training for more than 20 y, 33 of 137 (24.1%) 11–20 y, 31 of 137 (22.6%) 5–10 y, and 22 of 137 (16.1%) fewer than 5 y out of training.
By contrast, only 14 of 60 (23.3%) NM residents were graduates of U.S. medical schools. In addition, 1 of 60 (1.7%) planned to become board certified by ABR, 0 of 60 (0%) ABR + CAQ, 24 of 60 (40%) ABNM, and 35 of 60 (58.3%) ABR + ABNM.
Exposure to NM in Medical School
Only 7 of 20 (35.0%) NM PDs reported that NM is part of their medical school curriculum (3 PDs did not answer this question), with 5 of 7 (71.4%) institutions offering NM only as part of the radiology curriculum. Among schools where NM was offered as part of the radiology curriculum, it was mandatory in 4 of 5 (80%) programs. Most (6/7 [85.7%]) of the medical schools offering NM in the curriculum did so during years 3 and 4. Exposure to radiology and NM during medical school is detailed in Figures 5 and 6, respectively.

Exposure to radiology during medical school.

Exposure to NM during medical school.
DISCUSSION
Our study results indicate that compared with the general population, women and members of URiM racial and ethnic groups are underrepresented in NM.
Among women, this diversity gap exists at the resident level, is greater at the NM faculty level, and is even more pronounced in NM leadership positions. Our findings are consistent with other studies demonstrating underrepresentation of women in medical imaging both in the U.S. and globally, especially in higher rank positions. In a recent study of NM specialists in Canada and the United States, women comprised just 7.8% of first-in-command roles and 12.5% of second-in-command roles despite comparable academic performance in terms of number of publications, number of citations, years of active research, and h-index, which takes productivity and citation impact of the publications into account (19). Women in NM are also underrepresented compared with women in academic medicine at the resident, faculty, and PD level. The percentage of women division chiefs in our sample was slightly higher than the percentage of women department chairs in academic medicine (30.4% vs. 25.6%).
According to the AAMC, URiM is defined as “those racial and ethnic populations that are underrepresented in the medical profession relative to their numbers in the general population,” and historically underrepresented URiM groups include individuals who identify as Black, Mexican-American, Native American (i.e., American Indian, Alaska Native, and Native Hawaiian), and mainland Puerto Rican (13). As of 2014, 18% and 13% of the U.S. population identified as Hispanic or Black, respectively, but these URiM groups represented only 8.9% of the physician workforce (20). In our study, we found persistently low representation of URiMs in NM (defined as Black/African American, American Indian/Alaska Native or Native Hawaiian/Pacific Islander, or Hispanic/Latinx based on U.S. Census Bureau race and ethnicity categories and historically underrepresented racial/ethnic groups in medicine), particularly among faculty and leadership positions with just 6.6% of male faculty and 5.8% of female faculty belonging to a racial or ethnic URiM group. Although the percentage of NM residents who are members of URiM groups is slightly higher than the percentage of members of URiM groups in general academic medicine, members of these racial and ethnic groups as a whole are underrepresented in medicine compared with the general population. The percentage of NM faculty who are members of a URiM group is similar compared with the underrepresentation of these racial and ethnic groups in general academic medicine but underrepresented compared with the general population. The percentage of division chiefs in NM who are members of a URiM group is slightly higher than the percentage of general academic medicine department chairs who are members of a URiM group but remains grossly underrepresented compared with the general population.
Notably, we found a higher proportion of female and members of racial or ethnic URiM groups among current residents, with 38.3% being women and 20% members of URiM groups, compared with clinical NM faculty, suggesting a positive trend for future greater representation.
Our results demonstrate a lower percentage of U.S. medical school graduates among NM residents compared with faculty, supporting mounting evidence that fewer medical school graduates are entering the traditional NM training pathway in the United States. In the last decade, the number of ACGME-accredited NM residency programs has dropped by 23% and the number of NM residents has dropped by 48%; as of 2016 just 54% of NM residency slots and 35% of nuclear radiology fellowship spots were filled (21). In addition, the percentages of international medical graduate (IMG) residents and faculty in NM are much higher than the percentages of IMG residents and faculty in the general medical workforce.
Furthermore, whereas most NM clinical faculty members were U.S. medical school graduates certified by ABNM alone, current NM residents were predominantly international medical graduates planning to become board certified in ABR + ABNM. The increasing popularity of combining NM and radiology may be explained by job market forces. Physicians who are trained in both diagnostic radiology and NM/nuclear radiology (NR) have a competitive advantage over those trained solely in NM/NR because those with cross-training in diagnostic radiology can provide broader independent interpretations of imaging (21).
Although cross-trained diagnostic radiology and NM/NR physicians are well prepared to interpret imaging studies, the imaging-focused approach of dual NM/NR programs may not adequately train physicians to apply targeted NM therapies such as nuclear theranostics for optimally managing cancer and other medical conditions, for example, the use of peptide receptor radionuclide therapy to target somatostatin receptors diagnostically and therapeutically (22), radioiodine to forecast response to therapy among patients with advanced thyroid cancer and inform treatment pathways (23), and lutetium prostate-specific membrane antigen for metastatic prostate cancer (24). Beyond oncologic care, the use of theranostics is actively being pursued for the management of myriad conditions including pulmonary (25) and neurologic disorders (26). With increasing recognition of the potential of radiopharmaceutical therapy as a safe and effective targeted approach to treating numerous medical conditions, the clinical need for hospital-based radionuclide/radioligand therapy is expected to grow exponentially (27), making the training mismatch even more concerning, especially given the limited exposure to radionuclide/radioligand therapy topics in medical school curricula. Although our study shows insufficient NM exposure during medical school, our study did not examine specific medical student exposure to NM therapies, but we hypothesize that exposure to NM therapies is lacking similarly to general NM exposure in medical school curricula, if not more so, and future studies are warranted.
Our study identified low numbers of women and members of racial and ethnic URiM groups in NM, in addition to an overall decline in the percentage of U.S. medical school graduates pursuing NM. Physicians often cite exposure in medical school as a critical factor in specialty choice, and previous research has shown that women have less preclinical radiology exposure than do men (28). In our study, NM was included in the medical school curriculum at fewer than one third of academic centers with NM residency programs and was typically not offered until the third or fourth years of medical school. It is likely that students at medical schools without dedicated postgraduate NM training programs have even less NM exposure.
These findings are in line with a recent study that found that most NM experience came during radiology lectures or clinical clerkships. In this same study, there was a significant difference between the perception of NM exposure by NM trainees versus NM exposure reported by faculty. The NM trainee perception of exposure to NM in medical school was reported as 35% and 52% during preclinical and clinical medical school training, respectively, whereas that reported by faculty who teach NM was 76% and 91.7%, respectively (17). This difference of perception highlights the necessity for teaching NM in medical school, to do so early on, and for it to be a meaningful experience that allows students to imagine themselves becoming NM and molecular imaging physicians. Accordingly, incorporation of all facets of NM and molecular imaging into the medical school curriculum, from imaging interpretation to NM therapies, is warranted.
Female physicians have identified mentorship as an important factor in their career paths. Women with mentors have more publications and spend more time on research activity than those without mentors; in addition, women with a role model report higher overall career satisfaction (29). A lack of female role models in NM leadership and low exposure to NM in medical school may contribute to the underrepresentation of women in NM.
Possible barriers to members of racial and ethnic URiM groups and women choosing NM and reaching leadership positions in NM include lack of exposure to NM before medical school and in the first 2 y of medical school as well as lack of representation among NM faculty and leadership. As such, possible strategies to address diversity gaps in NM include increasing early exposure to NM, increasing NM mentorship and sponsorship, increasing awareness of structural racism and structural gender bias and how to combat them, and implementing leadership training, especially for women and members of racial and ethnic URiM groups.
Diversity gaps are not unique to medicine. They exist in many areas of society including in other fields requiring postgraduate training such as academia (in which the percentage of nonwhite professors at degree-granting postsecondary institutions is 22% and the percentage of women professors is 33% (30)) and law (in which the percentage of people of color who are partners is <10% and the percentage of women partners is <25% (31)) as well as in finance (in which the percentage of African American officials and managers in the securities subsector is <5% and the percentage of women officials and managers in the securities subsector is <35% (32)) and business (in which the percentage of Black chief executive officers of Fortune 500 companies is <1% (33) and the percentage of women Black chief executive officers of Fortune 500 companies is <8% (34)).
Our study had some limitations, most notably a small sample size of PDs answering on behalf of other faculty and residents. Responding to our survey was voluntary, and response bias is possible. However, PDs are well positioned to provide the type of factual programmatic information we sought in our research, so the information obtained is likely representative of respondents’ institutions. In addition, our study focused on women and URiM racial and ethnic groups and did not assess representation of other URiM groups such as LGBTQ+ individuals or individuals with disabilities, who deserve further attention in future studies. In addition, and importantly, URiMs are a heterogeneous group of people of different races and ethnicities who are grouped together in this study. Future studies examining specific representation of members of each racial and ethnic group and of people with cross-sectional identities are warranted. We also surveyed only PDs of AGCME-accredited NM residency programs; we did not look at nuclear radiology fellowships, NM therapy fellowships, nonaccredited NM fellowships, or radiology residency programs with participants in the 16-mo combined diagnostic radiology/nuclear radiology dual-certification pathway. Nevertheless, the data we were able to gather enable a better understanding of representation of women and members of racial and ethnic URiM groups in a majority cross-section of ACGME-accredited NM residency programs in the United States.
CONCLUSION
Increasing early exposure to NM before and during medical school, with a special focus on women and members of racial and ethnic URiM groups, may improve recruitment of diverse trainees through both traditional and newer training pathways as 1 component of advancing diversity, equity, and inclusion in academic NM. We hope that this study encourages readers to evaluate the diversity of their workforce and assess whether it matches their community.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: In NM training programs, what percentage of trainees and faculty members are women or members of racial and ethnic groups that are underrepresented in medicine in the United States (URiM)?
PERTINENT FINDINGS: This survey study found that women and members of racial and ethnic URiM groups are underrepresented in NM training programs; this diversity gap is more pronounced among NM faculty and, to an even greater extent, in leadership positions. NM is included in the medical school curriculum at fewer than one third of academic centers with NM residency programs, typically toward the end of medical school.
IMPLICATIONS FOR PATIENT CARE: Increasing early exposure to NM in medical school with a special focus on women and members of racial and ethnic URiM groups may improve recruitment of diverse trainees, which can improve the provision of equitable and culturally competent patient care.
Footnotes
Published online April 23, 2021.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication November 20, 2020.
- Accepted for publication April 13, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.