


Abstract
Part 2 of this series of Continuing Education articles on benign thyroid disorders deals with nodular goiter, hypothyroidism, and subacute thyroiditis. Together with Part 1 (which dealt with various forms of hyperthyroidism), this article is intended to provide relevant information for specialists in nuclear medicine dealing with the clinical management of patients with benign thyroid disorders, the primary audience for this series. Goiter, an enlargement of the thyroid gland, is a common endocrine abnormality. Constitutional factors, genetic abnormalities, or dietary and environmental factors may contribute to the development of nodular goiter. Most patients with nontoxic nodular goiter are asymptomatic or have only mild mechanical symptoms (globus pharyngis). Work-up of these patients includes measurement of thyroid-stimulating hormone, free triiodothyronine, free thyroxine, thyroid autoantibodies, ultrasound imaging, thyroid scintigraphy, and fine-needle aspiration biopsy of nodules with certain ultrasound and scintigraphic features. Treatment for multinodular goiter includes dietary iodine supplementation, surgery, radioiodine therapy (to decrease thyroid size), and minimally invasive ablation techniques. Hypothyroidism ranges from rare cases of myxedema to more common mild forms (subclinical hypothyroidism). Primary hypothyroidism often has an autoimmune etiology. Clinical presentations differ in neonates, children, adults, and elderly patients. Work-up includes thyroid function tests and ultrasound imaging. Nuclear medicine is primarily used to locate ectopic thyroid tissue in congenital hypothyroidism or to detect defects in iodine organification with the perchlorate discharge test. Treatment consists of thyroid replacement therapy with l-thyroxine, adjusting the daily dose to the individual patient’s metabolic and hormonal requirements. Subacute thyroiditis is a self-limited inflammatory disorder of the thyroid gland, often associated with painless or painful swelling of the gland and somatic signs or symptoms. Inflammation disrupts thyroid follicles resulting in a rapid release of stored thyroxine and triiodothyronine causing an initial thyrotoxic phase, often followed by transient or permanent hypothyroidism. Although subacute thyroiditis is often related to a viral infection, no infective agent has been identified. Subacute thyroiditis may be caused by a viral infection in genetically predisposed individuals. Work-up includes lab tests, ultrasound imaging, and radionuclide imaging. Thyroid scintigraphy demonstrates different findings depending on the phase of the illness, ranging from very low or absent tracer uptake in the thyroid gland in the hyperthyroid phase to a normal appearance in the late recovery phase. Since subacute thyroiditis is self-limited, treatment is directed toward relief of pain. High-dose nonsteroidal antiinflammatory drugs are usually the first-line treatment. If severe pain persists, a course of corticosteroids may be necessary. Permanent hypothyroidism develops in up to 15% of patients with subacute thyroiditis, even more than 1 y after presentation.
- diffuse and nodular goiter
- primary autoimmune hypothyroidism
- subacute, destructive thyroiditis
- lab tests for benign thyroid disorders
- ultrasound imaging
- radionuclide imaging
This is Part 2 of the continuing education series on benign thyroid disease. Part 1 of this series, published in the March 2021 issue of The Journal of Nuclear Medicine (1), dealt with hyperthyroid states due to Graves disease, toxic multinodular goiter, toxic adenoma, and destructive thyroiditis. This Part 2 paper deals with nodular goiter, hypothyroidism, and subacute thyroiditis. These two articles provide relevant information for specialists in nuclear medicine dealing with the clinical management of patients with benign thyroid disorders.
GOITER AND THYROID NODULES
Epidemiology and Clinical Presentation
Goiter, an enlargement of the thyroid gland (>20 cm3 in men and >15 cm3 in women) with or without nodules, is one of the most common endocrine abnormalities. If thyroid function is normal, the goiter is described as nontoxic and nodular. The incidence of new nodular goiter cases in adults in the United States is 0.1%–1.5% of the general population per year (2). Goiter is more common in women than men (3). In areas of iodine deficiency, the incidence of thyroid nodules increases with age (without a sex-related difference) (4), whereas in iodine-sufficient areas the prevalence of nodular goiter decreases with age (5). Constitutional factors, genetic abnormalities, and dietary or environmental factors may contribute to the development of nodular goiter (3–6). Thyroid nodules may become autonomous, possibly evolving to cause thyrotoxicosis.
Clinically, goiter is categorized as diffuse goiter, solitary nodular goiter, or the most prevalent phenotype, multinodular goiter. Most patients with nontoxic nodular goiter are asymptomatic or have mild mechanical symptoms (globus pharyngis). Nodular goiter is often discovered incidentally during an ultrasound scan performed for other reasons. Symptoms of compression of the trachea, esophagus, great vessels, and recurrent laryngeal nerve in the presence of a goiter suggest that a long-term nodular goiter has partially migrated to the retrosternal or upper mediastinal regions.
Etiology and Pathophysiology
Worldwide, the most important environmental factor for goiter development is iodine deficiency (3,4,7), and there is an inverse correlation between iodine intake and the prevalence of goiter (8). Other factors include genetic susceptibility, female sex, increased body mass, and smoking (7,9,10). Smoking promotes goiter development, probably because of the thiocyanate in cigarette smoke, which block iodination, leading to a compensatory increase in secretion of the thyroid-stimulating hormone (TSH) (11).
Lab Tests
TSH, free thyroxine (T4), and free triiodothyronine (T3) should be measured. If the TSH is reduced and free T4 and/or free T3 is elevated, the patient has progressed to a toxic nodular goiter. In iodine-deficient areas, nodules may become autonomous because of persistent stimulus from elevated TSH due to reduced thyroid hormone production.
The presence of antibodies recognizing thyroid peroxidase, thyroglobulin, or the TSH receptor suggests the coexistence of Hashimoto disease or Graves disease.
Ultrasound Imaging
Ultrasonography is used to determine thyroid volume and the echogenicity, margins, shape, content, calcifications, vascularity, size, and elasticity of nodules, in addition to the status of regional lymph nodes (Fig. 1; Supplemental File 1; supplemental materials are available at http://jnm.snmjournals.org). The European Thyroid Association (12), the American College of Radiology (13), and the American Thyroid Association (14) have issued guidelines (with slight differences) for stratifying the risk of malignancy for thyroid nodules according to the so-called Thyroid Imaging Reporting and Data System (TI-RADS). The ultrasound-based criteria (Tables 1 and 2) stratify thyroid nodules into 5 categories of risk of malignancy, a change from prior consensus guideline that stratified the ultrasound risk of malignancy into 3 categories (15); examples of thyroid nodules with different European Thyroid Association Thyroid Imaging Reporting and Data System (EU-TIRADS) scores are presented in Supplemental File 2. About 50% of the nodules can be classified as benign by ultrasound criteria alone, and nodules with low-risk features have a false-negative risk of only 0.3% (12). It is still debated which TI-RADS version provides a better outcome (16,17). Ultrasound guidance is crucial to localize sites for fine-needle aspiration biopsy (FNAB) (18) and minimally invasive therapeutic procedures (19).

Ultrasonography of multinodular thyroid gland (axial view). Right lobe shows single well-defined isoechoic nodule surrounded by hypoechoic rim (halo sign). Left lobe shows mixed nodule, cystic with echogenic solid component. MN = mixed nodule in left lobe; SDM = skin, dermis, and muscles forming superficial layer in neck; SN = solid nodule in right lobe; TL = tracheal lumen; TW = tracheal wall.
TI-RADS Ultrasound Features of Thyroid Nodules
FNAB of Thyroid Nodules
The prevalence of thyroid cancer in patients referred for goiter evaluation is 4%–18% (20). FNAB should be performed in suggestive nodules with high-risk ultrasound features, especially if combined with the scintigraphic features described further below. Table 3 summarizes the main features of the 2 most widely used systems for classifying the cytology findings according to the risk of malignancy, the Bethesda system and the British Thyroid Association system. Approximately 20% of FNABs of thyroid nodules have indeterminate cytology (Bethesda score III, or British Thyroid Association score Thy3a-f), with a rate of malignancy of 10%–30% (21). Molecular testing for gene mutations (e.g., BRAF, RAS, RET/PTC, and PPARγ) enhances the accuracy of FNAB in nodules with indeterminate cytology (22,23).
Prognostic Stratification of Cytology Findings After FNAB of Thyroid Nodules According to Bethesda Reporting System Vs. British Thyroid Association (BTA) Reporting System
Diagnostic and Therapeutic Radionuclide Procedures
Thyroid Scintigraphy with 123I-Iodide or 99mTc-Pertechnetate
Thyroid scintigraphy provides a map of functioning thyroid parenchyma (Fig. 2), including hypofunctioning nodules (cold areas on the scan) or autonomously functioning nodules (hot areas on the scan, with variable uptake in the extranodular thyroid parenchyma, up to complete suppression). Combined with ultrasonography, thyroid scintigraphy can determine which thyroid nodules should be characterized with FNAB (24). Nodules that appear as warm or hot on thyroid scintigraphy are rarely malignant (25); therefore, FNAB of such lesions is not indicated (Fig. 3).
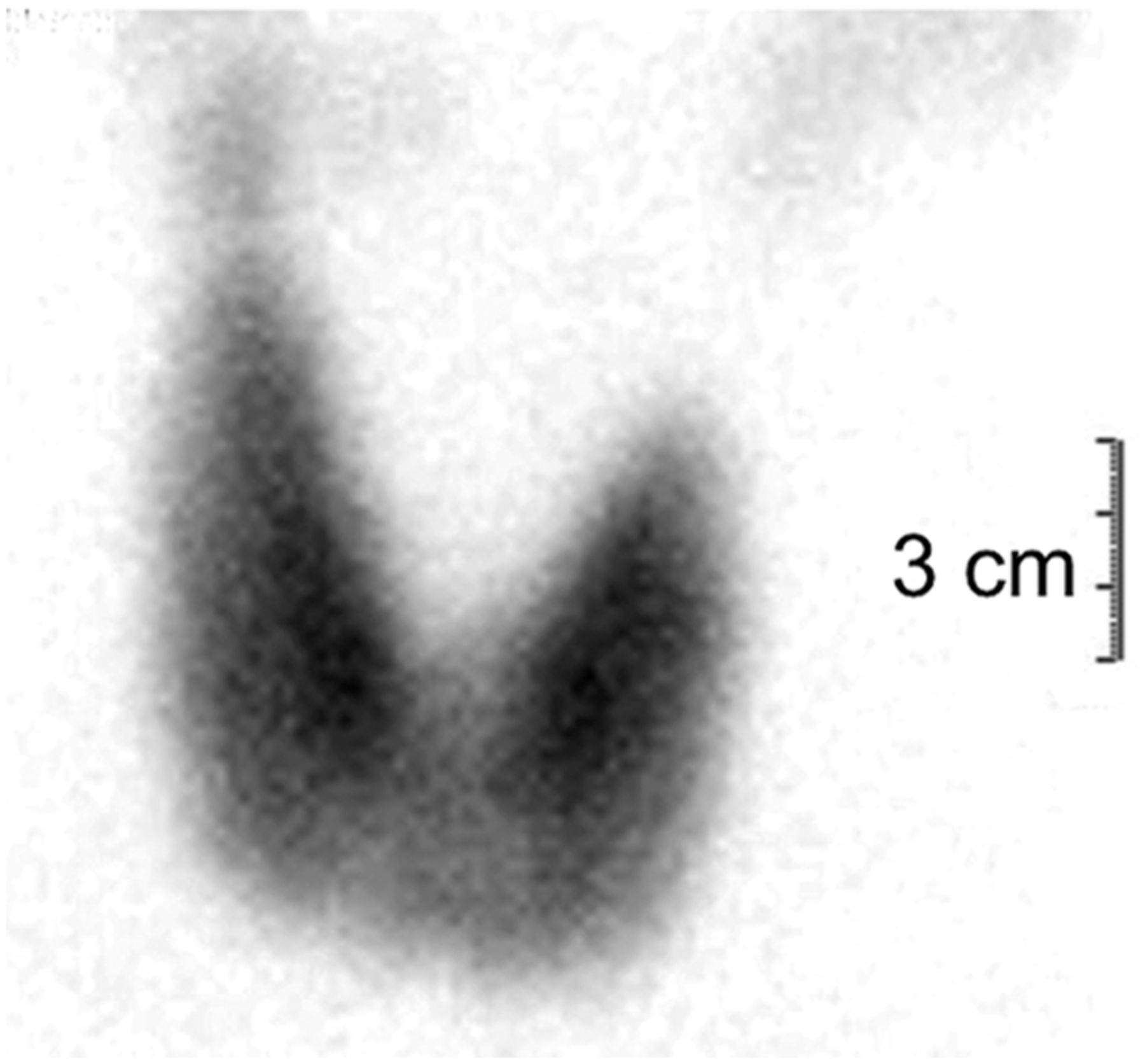
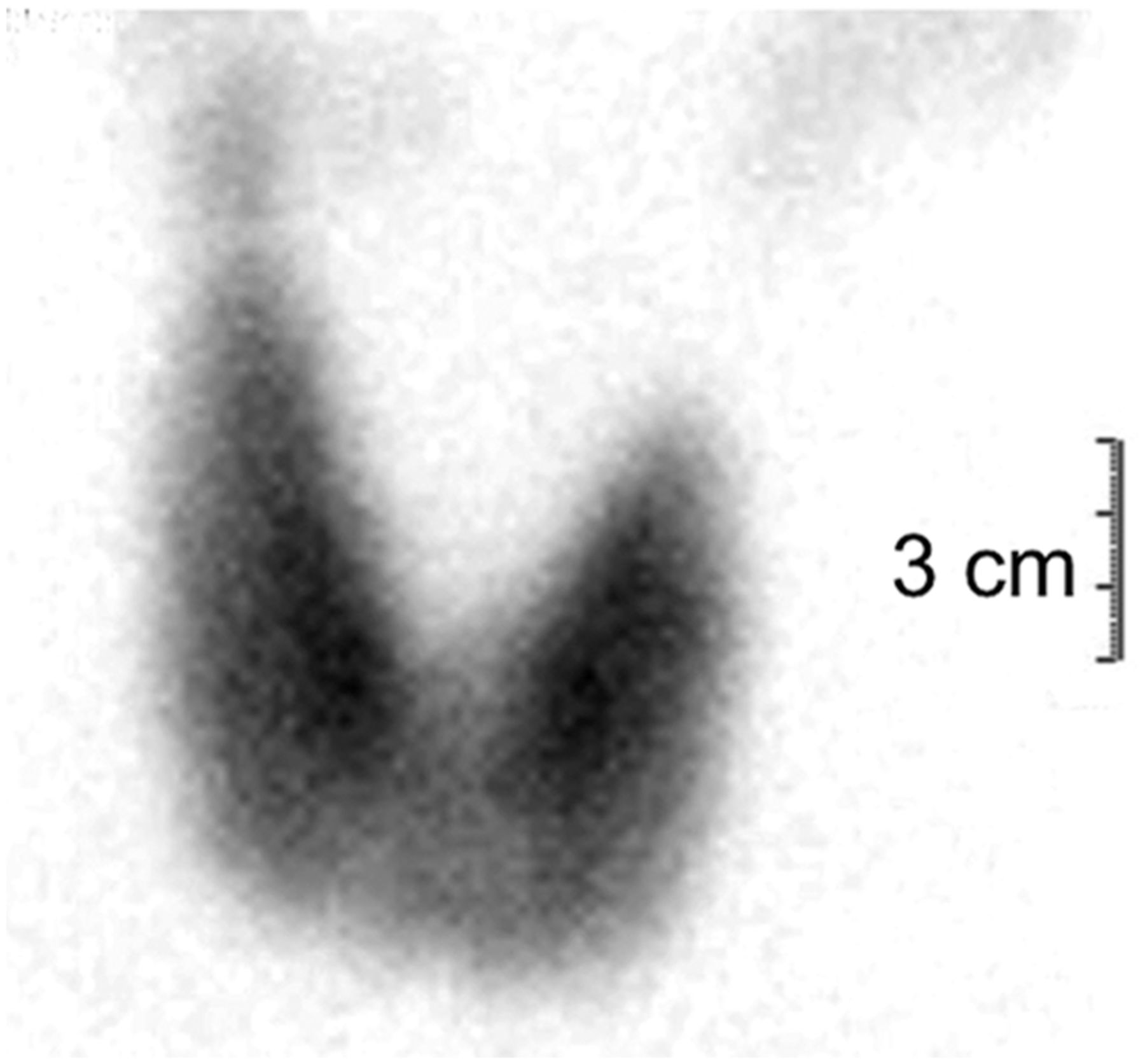
Thyroid scintigraphy (anterior view) acquired 15 min after intravenous injection of 99mTc-pertechnetate in patient with diffuse, nonnodular goiter and normal thyroid function, showing global hyperplasia of thyroid with homogeneous tracer distribution within gland. Right lobe is larger than left, with longitudinal axis measuring about 70 mm.

Thyroid scintigraphy in 2 patients with nodular goiter (anterior view). (Left) 99mTc-pertechnetate scan acquired 15 min after intravenous injection, showing moderately enlarged gland with reduced tracer uptake in lower half of left lobe, corresponding to palpable nodule (outlined in green); if suggestive ultrasound features are seen for this nodule, patient should be referred for FNAB. (Right) scan acquired with pinhole collimator 24 h after oral administration of 1.85 MBq of 131I-iodide to see whether patient is candidate for radioiodine therapy of multinodular goiter with autonomously functioning nodules; only nodule at apex of right lobe (outlined in red) shows increased tracer uptake, whereas nodules at base of right lobe and at isthmus (outlined in green) do not concentrate radioiodine (cold nodules); FNAB was performed because of intermediate-risk EU-TIRADS score and showed both nodules to be benign.
In areas with sufficient dietary iodine intake, thyroid scintigraphy is not necessary in patients with diffuse, nodular, or multinodular goiter when serum TSH is normal, because all such nodules usually appear as cold areas on the scan and should be evaluated with FNAB if exhibiting a high TI-RADS score and exceeding 10 mm in any diameter (26,27). However, in iodine-deficient areas, the serum TSH level alone may not be sufficient to exclude the presence of autonomously functioning thyroid nodules (28), and thyroid scintigraphy should be performed on all patients with nodular goiter. A metaanalysis showed a 50% prevalence (95% CI, 32%–68%) of normal TSH values in patients with autonomously functioning thyroid nodules (29).
PET/CT with 18F-FDG in Patients with Nodular Goiter
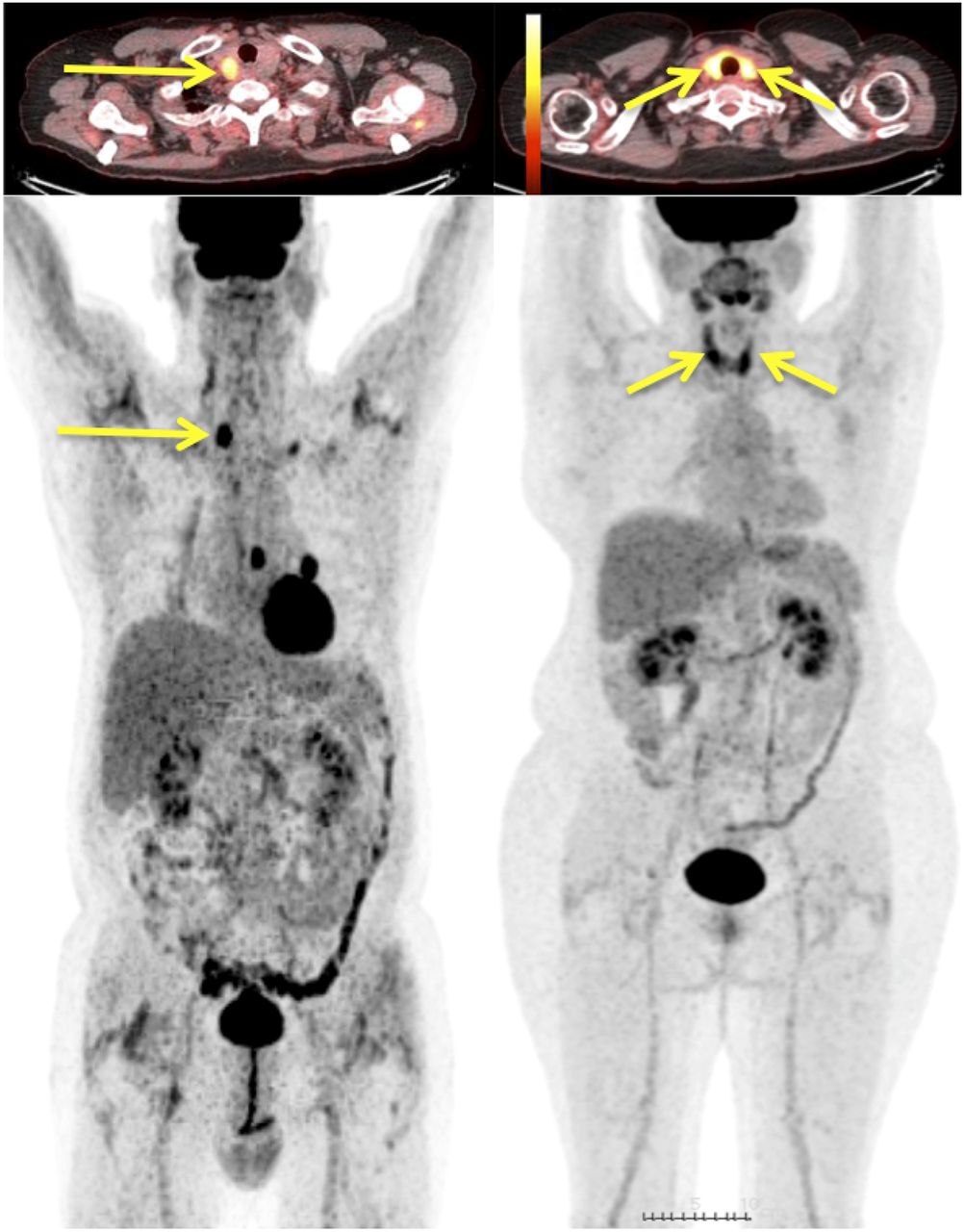
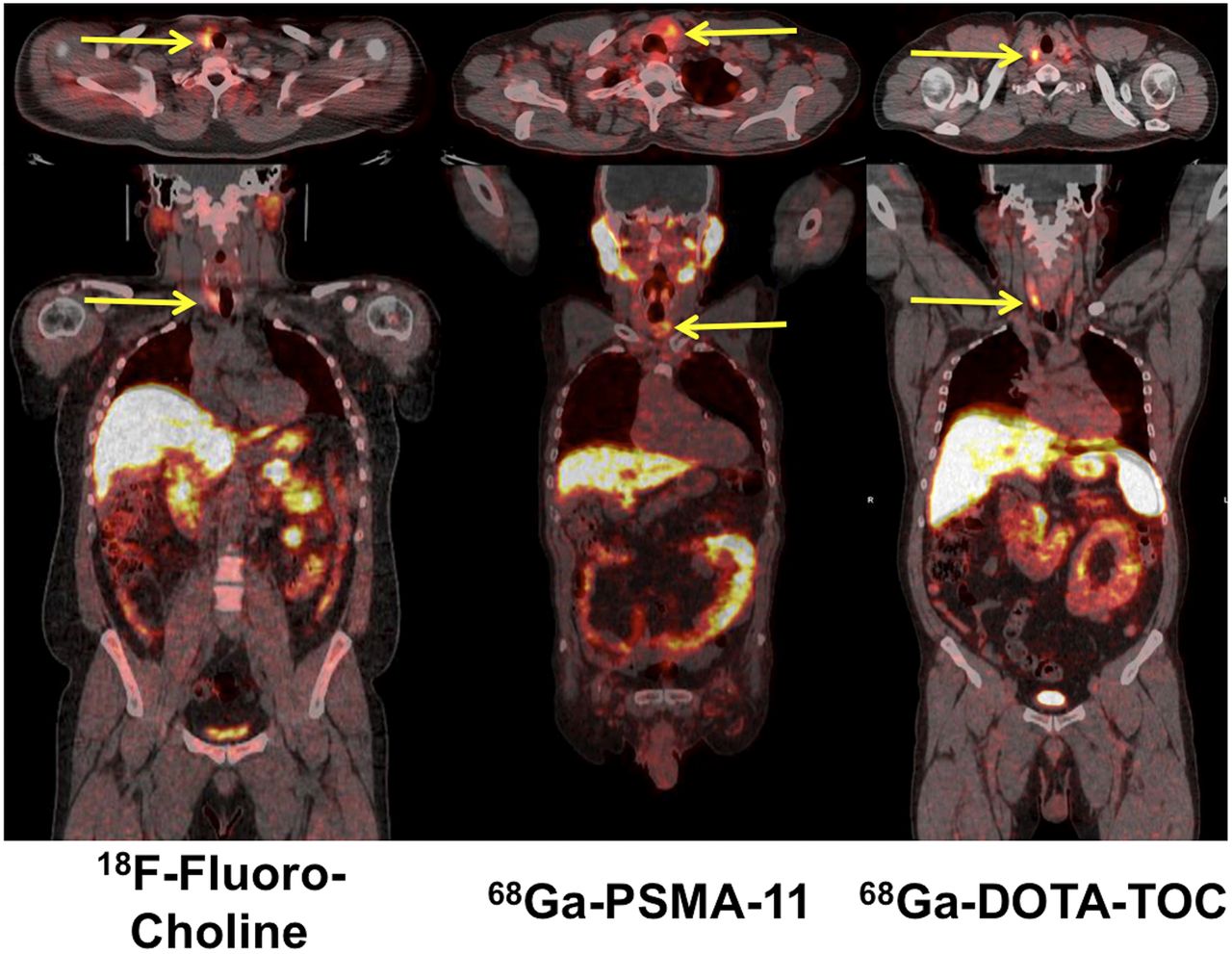
Incidentalomas—when an 18F-FDG PET/CT scan performed for reasons not related to the thyroid (usually in patients with nonthyroid cancers) shows increased tracer uptake in the thyroid gland—are seen in 1%–2% of all 18F-FDG scans. Two patterns of 18F-FDG uptake have been observed, diffuse and focal (Fig. 4). Diffuse 18F-FDG uptake in the thyroid gland is usually associated with autoimmune thyroiditis and has little or no clinical relevance (30–32). Focal 18F-FDG uptake in the thyroid gland can be found in nodular goiter, and about 35% of these incidentalomas are thyroid cancer (33). Therefore, these cases should be further investigated for unequivocal characterization (34). The occurrence of thyroid incidentalomas during a PET/CT scan is not unique to 18F-FDG, as they can be observed also with other PET tumor imaging agents, for example, 18F-fluorocholine, 68Ga-DOTATOC, and 68Ga-prostate-specific membrane antigen ligand (Fig. 5) (35–37).
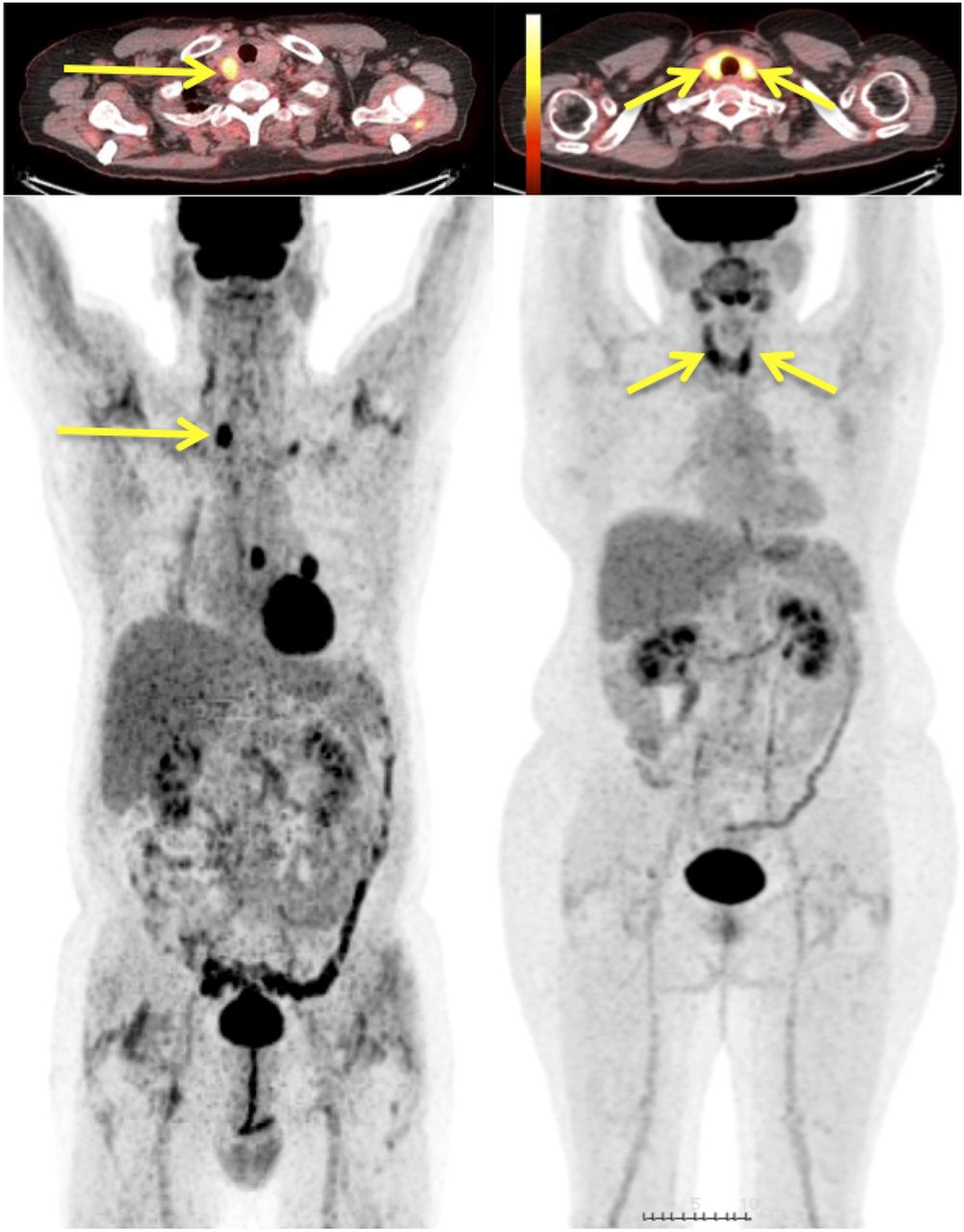
Thyroid incidentalomas observed in 2 patients undergoing 18F-FDG PET/CT for thyroid-unrelated oncologic conditions (top: axial PET/CT; bottom: whole-body maximum-intensity-projection image). Arrows indicate unexpected findings of focally increased tracer uptake (left) and diffuse tracer uptake (right). Although diffusely enhanced tracer uptake is generally associated with thyroiditis, any focal increase in tracer uptake must be further evaluated with ultrasound and possibly FNAB, because of relatively high rate of thyroid malignancy.
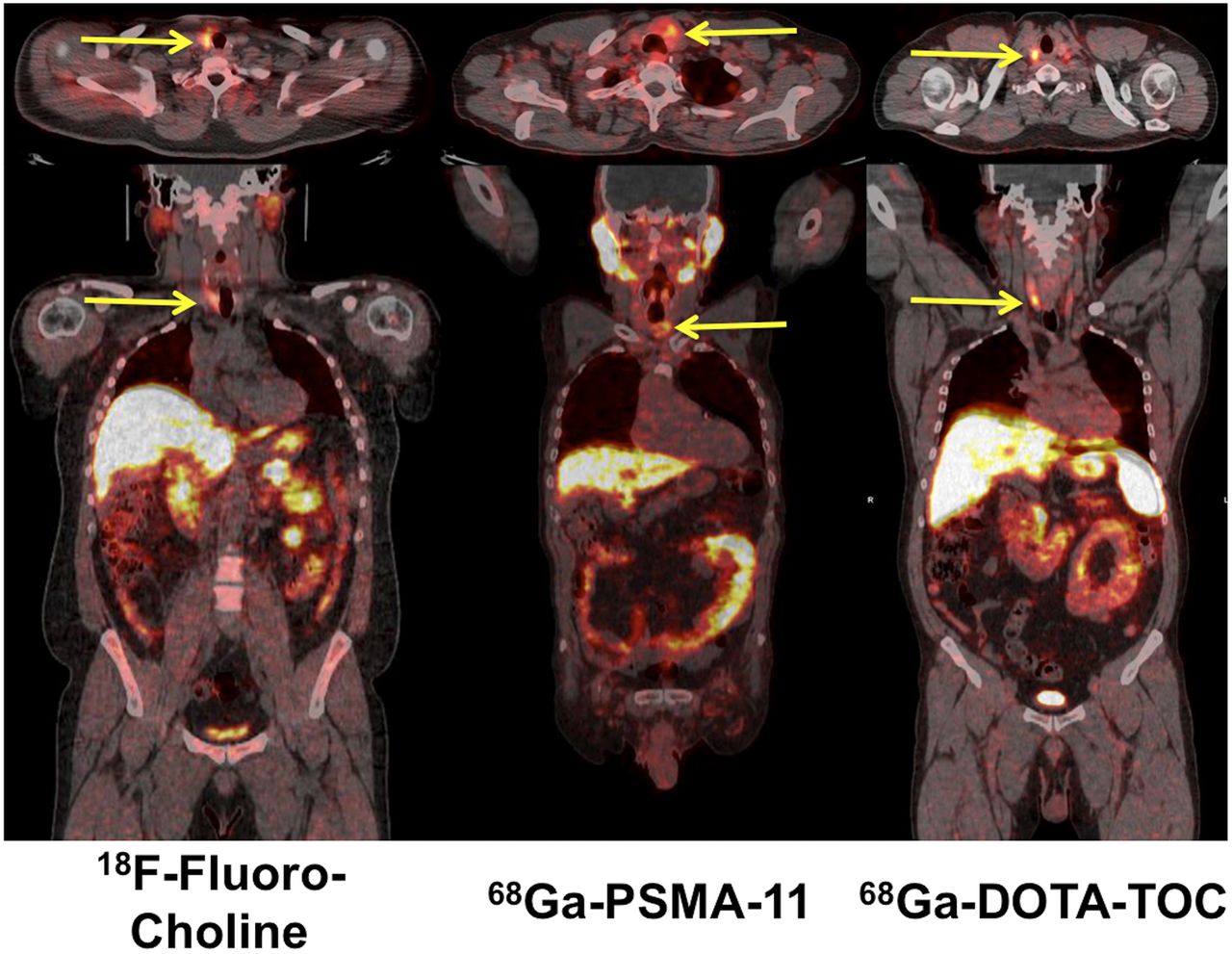
Thyroid incidentalomas (arrows) observed in 3 patients evaluated with PET tracers other than 18F-FDG for oncologic conditions (top: axial PET/CT; bottom: coronal PET/CT). (Left) Patient with biochemical recurrence of prostate cancer, who had previously undergone left hemithyroidectomy because of nodular goiter. Histology showed chronic autoimmune thyroiditis. Diffusely enhanced 18F-fluorocholine uptake in residual right thyroid lobe corresponds to autoimmune thyroiditis. (Center) Patient with focally increased 68Ga-prostate-specific membrane antigen 11 uptake within multinodular goiter prevalent in left lobe. (Right) Patient with focally increased 68Ga-DOTATOC uptake in right thyroid lobe. (Courtesy of Paola A. Erba and Roberta Zanca, Regional Center of Nuclear Medicine, University of Pisa, Pisa, Italy.)
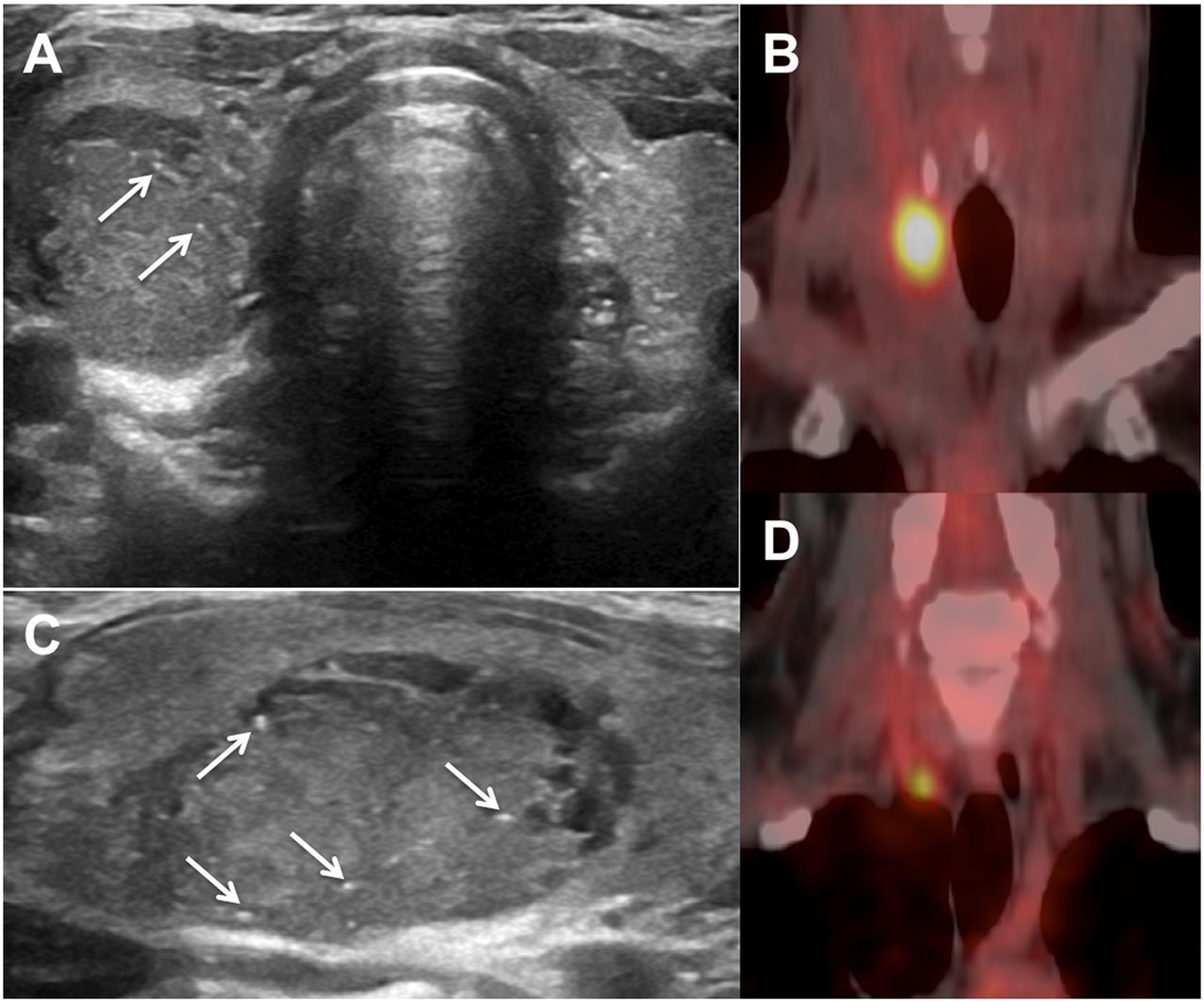
18F-FDG–avid thyroid nodules that cannot be classified with FNAB cytology are more likely to be malignant than a nodule without enhanced 18F-FDG uptake (Fig. 6); whereas a similar thyroid nodule without increased 18F-FDG uptake is highly unlikely to be malignant (38–40). Although any focal 18F-FDG uptake above the normal thyroid background is interpreted as positive and a high SUVmax increases the risk of malignancy (39,41), no specific SUVmax threshold has been identified to reliably discriminate malignant from benign thyroid nodules.

Evaluation of 30-y-old woman with family history of familial papillary thyroid carcinoma. Axial (A) and longitudinal (C) ultrasonography shows 25-mm mixed isoechoic–hypoechoic solid nodule of right lobe, with microcalcifications (arrows). Serum calcitonin was undetectable, and TSH was 2.7 μIU/mL; FNAB showed high-risk undetermined lesion (British Thyroid Association grade Thy3f). (B) Coronal 18F-FDG PET/CT showed intense focal uptake (SUVmax, 12) in thyroid nodule of right lobe. (D) Another coronal image showed additional focus of increased 18F-FDG uptake in deeper plane, corresponding to small lymph node of central compartment not detected at ultrasonography. Patient underwent thyroidectomy and lymph node dissection of central compartment, which revealed BRAF-mutated papillary thyroid carcinoma with multiple lymph node metastases. (Courtesy of Arnoldo Piccardo, Nuclear Medicine Department, “Galliera” Hospital, Genoa, Italy.)
Therapy of Nodular Goiter
Surgery
Compressive symptoms are a major indication for surgery, as stated by the American Thyroid Association and by the German Society for General and Visceral Surgery (42).
Radioiodine Therapy for Reduction of Goiter Volume
Patients who have either diffuse or nodular goiter with mechanical symptoms and cannot undergo surgery because of comorbidities (43) can be treated with radioiodine. A practical approach to determine the activity to be administered is based on the assumption of a target activity of 3.7 MBq (100 μCi) of radioiodine per gram of functioning thyroid tissue 24 h after administration. The initial estimate (i.e., 3.7 MBq × volume of functioning thyroid tissue as assessed by thyroid scintigraphy) is corrected by the 24-h radioiodine uptake value. More personalized dosimetry-based approaches to determine the activity of radioiodine for therapy (44) were discussed in part 1 of this continuing education article (1). Whereas in Graves’ disease the target absorbed dose necessary to ablate hyperfunctioning thyroid tissue is between 200 and 400 Gy, data derived from external-beam radiation therapy for cancers of the head and neck suggest that an absorbed dose of between 100 and 150 Gy is sufficient for ablation of normal thyroid parenchyma (45,46).
This treatment causes an average 30%–40% volume reduction within 1 y after treatment, with a further reduction of up to 50%–60% of the initial thyroid volume or mass in the following year (43). To increase radioiodine uptake in multinodular glands, an off-label use of recombinant human TSH, administered intramuscularly as a single 0.3-mg dose 24 h before radioiodine therapy, has been suggested (47–51). An advantage of pretreatment with recombinant human TSH is that the activity of administered radioiodine is reduced by about half the activity that should be administered without recombinant human TSH before treatment, with a consequent reduction in overall radiation dosimetry (52,53).
Besides the usual contraindication in pregnant or lactating women, some conditions must be fulfilled before submitting patients to this treatment. Evaluation for malignancy (ultrasonography, thyroid scintigraphy, and FNAB if necessary) must be performed before radioiodine therapy. The total thyroid volume or mass must be evaluated for bulky goiters extending to the upper mediastinum (which may require evaluation by MRI or by CT without contrast agent). The active thyroid volume or mass should be evaluated by thyroid scintigraphy, considering that cystic lesions and other low-uptake areas are not expected to respond to radioiodine therapy.
Since most patients treated with radioiodine develop hypothyroidism within 2–3 y after therapy, all patients receiving radioiodine therapy should be followed with semiannual serum TSH assays (42,54).
Medical Therapy of Nodular Goiter
Once their benign nature has been established, goiters with small nodules usually do not require treatment and can safely be monitored with regular follow-up. Since iodine deficiency has a key role in thyroid enlargement, iodine supplementation may reduce goiter size (55,56).
Historically, TSH-suppressive therapy with l-thyroxine was used with the aim of reducing stimulation of thyroid parenchyma and nodules. Although this approach was widely embraced in the past (56–59), the long-term outcomes of this approach are still controversial (59). Current American Thyroid Association guidelines do not recommend the routine use of l-thyroxine for the treatment of benign thyroid nodules (14), although it may remain a feasible option for young patients in cases of mild iodine deficiency (59,60).
Minimally Invasive Treatments for Nodular Goiter
Tissue ablation techniques have been developed to induce necrosis or apoptosis of specific thyroid nodules. Recent minimally invasive techniques induce thermal ablation with different forms of energy such as microwaves, radiofrequency, high-intensity focused ultrasound, or laser energy (14).
HYPOTHYROIDISM
Epidemiology and Clinical Presentation
Hypothyroidism is a systemic condition caused by transient or permanent thyroid failure (primary hypothyroidism), deficiency of thyrotropin secretion (TSH) (secondary, or central hypothyroidism), or resistance of peripheral target tissues (Supplemental File 3).
The spectrum of hypothyroidism ranges from severe overt hypothyroidism (myxedema) to milder forms—that is, subclinical hypothyroidism. Primary hypothyroidism accounts for 95%–99% of thyroid failure and usually has an autoimmune etiology. Deficiency of pituitary or hypothalamic function (secondary or tertiary hypothyroidism) and peripheral resistance to thyroid hormones, or their inactivation due to autoantibodies, are rare.
The prevalence of hypothyroidism in the United States (defined as TSH levels > 4.5 mIU/L) is 3.7% of the general population (61). In Europe it is 0.65% (95% CI, 0.38%–0.99%) for overt and 4.11% (95% CI, 3.05%–5.31%) for subclinical hypothyroidism (62).
Congenital Hypothyroidism
Congenital hypothyroidism is the most frequent congenital endocrine disorder (1:2,200–2,500 live births). Delayed diagnosis leads to growth retardation and severe neurologic and psychiatric impairment.
Children and Adolescent Hypothyroidism
Hypothyroidism in children and adolescents is characterized by retarded growth and short stature, variable but usually declining school performance, and signs or symptoms similar to those occurring in adults. In addition to the history and physical examination, laboratory evaluation should include TSH, free T4, and free T3. In the presence of abnormal findings, the patient should be referred to a pediatric endocrinologist.
Hypothyroidism in Adults
Thyroid hormone deficiency reduces function in almost every organ system depending on the degree of hypothyroidism (Table 4).
Major Pathophysiologic and Clinical Changes in Moderate or Severe Hypothyroidism
Hypothyroidism in the Elderly
The most frequent signs or symptoms in the elderly are fatigue, muscle weakness, cold intolerance, dry skin, hair loss, constipation, poor appetite, depression or mental deterioration, hearing loss, cardiomegaly, and congestive heart failure.
Drug-Induced Hypothyroidism
The large amount of iodine released from amiodarone (an iodine-rich drug used for treating tachyarrhythmias) may fail to escape the Wolff–Chaikoff effect (described in the next section) and thus cause iodine-induced hypothyroidism, especially in patients with preexisting autoimmune thyroiditis (63,64). Lithium therapy may cause hypothyroidism by blocking both release and synthesis of thyroid hormones (65). Interferon may precipitate hypothyroidism, either by aggravating preexisting autoimmune thyroiditis or by a direct cytotoxic effect on thyroid follicular cells (66). Tyrosine kinase inhibitors may induce hypothyroidism by mechanisms not fully understood (67).
Pathophysiology
The most frequent cause of hypothyroidism in adults is autoimmune thyroiditis (Ord–Hashimoto disease). It most probably results from a combination of a predisposing genetic background with exogenous and endogenous factors (68). Infiltration of thyroid tissue by amyloidosis, hemochromatosis, sarcoidosis, cystinosis, scleroderma, or leukemia may also cause hypothyroidism and goiter.
Hypothyroidism may result from either severe iodine deficiency or iodine excess. In severe iodine deficiency, large goiters and variable degrees of hypothyroidism may be observed at any age. Excess iodine intake (>1–2 mg/d) acutely inhibits iodine organification and thyroid hormone synthesis (Wolff–Chaikoff effect) as well as thyroid hormone release. In most euthyroid subjects, iodine excess does not cause hypothyroidism, because there is an adaptive mechanism (escape, usually at ∼10 d after iodine loading); nevertheless, patients with preexisting thyroid abnormalities may fail to escape the Wolff–Chaikoff effect and thus develop hypothyroidism.
Iatrogenic hypothyroidism can be observed after treatment of hyperthyroidism with antithyroid drugs or radioiodine, as well as after total thyroidectomy or external-beam radiation therapy of the head and neck region.
Lab Tests
TSH
Primary hypothyroidism is characterized by increased TSH and decreased free T4; in subclinical hypothyroidism TSH is increased (generally between 5 and 10 mIU/L) and free T4 is normal. In central hypothyroidism, low free T4 is associated with low–to–inappropriately normal TSH.
Antibodies
Thyroid peroxidase antibodies and thyroglobulin antibodies are positive in most patients with autoimmune thyroiditis.
Lipids
In both overt and subclinical hypothyroidism, the lipid profile shows increased low-density lipoprotein cholesterol levels, with increased or normal high-density lipoprotein levels. Triglyceride levels are normal or slightly elevated.
Ultrasound Imaging
In hypothyroidism, the thyroid volume can be normal, increased (goiter), or reduced (atrophic form of chronic autoimmune thyroiditis, hypoplasia, or hemiagenesis) (Supplemental File 4). Inhomogeneous hypoechogenicity is typical of chronic autoimmune thyroiditis. Ultrasonography can also identify ectopic thyroid tissue in congenital hypothyroidism.
Radionuclide Techniques in Hypothyroidism
Nuclear medicine currently has a limited role in hypothyroidism, since the diagnosis is based on signs or symptoms and on thyroid hormonal profile (TSH, free T3, free T4). The only current application of radionuclide imaging in hypothyroidism concerns congenital hypothyroidism (69). Thyroid scintigraphy with either 99mTc-pertechnetate or preferably 123I-iodide constitutes the best standard for ascertaining thyroid agenesis or locating ectopic thyroid tissue in the mediastinum or at the base of the tongue, especially in newborns/children.
When the thyroid gland is in its normal location in a patient with congenital hypothyroidism, the cause of hypothyroidism can be genetic mutation, over 25 of which have been described (70,71). The perchlorate discharge test explores defects in the intrathyroidal organification process of iodide as a cause of congenital hypothyroidism. Once iodide is trapped in the thyroid gland after active transport mediated by sodium/iodide symporter, iodine binds to thyroglobulin, therefore no longer requiring active transport for intracellular retention. Perchlorate ions inhibit sodium/iodide symporter–mediated iodide transport and cause loss of iodide not bound to thyroid hormones. Evaluating the release of radioiodine caused by perchlorate allows evaluation of nonorganified intrathyroidal iodide and thus assessment of an iodide-binding defect (69).
Thyroid Replacement Therapy in Hypothyroidism
Approximately 85 μg of l-thyroxine are secreted by the thyroid gland daily. Of the total daily T3 production (about 33 μg in adult healthy humans), approximately 80% arises from peripheral conversion from T4, and only about 20% derives from direct thyroidal secretion. Synthetic l-thyroxine is recommended as the preparation of choice to treat hypothyroidism, because of its efficacy, favorable side-effect profile, ease of administration, good intestinal absorption, long serum half-life, and low cost. l-thyroxine is converted in vivo into its active metabolite T3. Nevertheless, a subgroup of hypothyroid patients does not achieve good results with l-thyroxine therapy alone (72); in these patients, combination therapy with l-thyroxine and liothyronine (l-T3) might be considered (73,74).
Hypothyroid patients with minimal endogenous thyroid function require l-thyroxine doses of 1.6–1.8 μg/kg of body weight (ideal body weight being a better predictor than actual body weight). Patients with l-thyroxine dose requirements much higher than expected should be evaluated for gastrointestinal disorders such as Helicobacter pylori–related gastritis, atrophic gastritis, celiac disease, lactose intolerance, and intestinal giardiasis. Serum TSH monitoring is advisable when starting medications such as phenobarbital, phenytoin, carbamazepine, rifampin, and sertraline.
Symptoms, such as cold intolerance or dry skin, lack sensitivity and specificity and therefore are not recommended for judging the adequacy of replacement in the absence of biochemical assessment. About 6–8 wk after a change in l-thyroxine dosage, serum TSH should be checked.
Subacute Thyroiditis
Subacute thyroiditis is a self-limited inflammation of the thyroid gland, often associated with painless or painful swelling of the gland and somatic signs or symptoms including fever and malaise (75). Painless subacute thyroiditis may be overlooked or misdiagnosed, especially when occurring in the postpartum period, occasionally related to postpartum psychosis or depression (76).
Originally described in 1895 by Mygind as “thyroiditis akuta simplex” (77), the pathology of subacute thyroiditis was first depicted in 1904 by the Swiss surgeon Fritz de Quervain, whose name is associated with the disorder. The inflammatory process causes disruption of thyroid follicles resulting in a rapid release of stored T4 and T3 causing an initial thyrotoxic phase, often followed by transient or permanent hypothyroidism.
Epidemiology and Clinical Presentation
The incidence of subacute thyroiditis is 4.9/100,000 people per year (78). Its prevalence is highest in middle-aged women (range of female-to-male ratio, 4:1–7:1). Subacute thyroiditis often occurs after an upper respiratory viral illness, thought to trigger the disease.
Anterior neck pain is the cardinal feature of de Quervain subacute thyroiditis. The inflammation can start in one lobe and then migrate to the contralateral lobe. Dysphagia is occasionally reported. The gland is firm and tender on palpation. In the early phases there can be signs of thyrotoxicosis (tachycardia, tremor, increased skin warmth), sometimes requiring the use of a β-blocker. The thyrotoxic phase may be followed by hypothyroidism, which is usually transient, although it can occasionally be permanent. In patients with hypothyroid symptoms, l-thyroxine replacement should be started, with frequent TSH monitoring to assess possible tapering or continuation of replacement therapy.
Etiology and Pathophysiology
Although subacute thyroiditis has been related to a viral infection (79), so far no infective agent has been clearly identified (80). The destructive events of subacute thyroiditis may trigger thyroid autoimmunity in subjects with a genetic background, occasionally resulting in chronic autoimmune thyroiditis with hypothyroidism (81) or in Graves disease (82).
About 72% of patients with subacute thyroiditis present the HLA-BW35 antigen (83), and familial subacute thyroiditis can be associated with HLA-B35 (84), suggesting that the disease may be caused by a viral infection in genetically predisposed individuals. Therapies potentially affecting the immune system may be associated with subacute thyroiditis (85), as in patients with chronic hepatitis B or C treated with interferon or ribavirin (66).
Lab Tests
Laboratory exams show a moderate leukocytosis, elevated erythrocyte sedimentation rate, and elevated serum C-reactive protein levels. In the thyrotoxic phase, suppressed serum TSH is associated with normal or elevated free T3 and free T4. The thyrotoxic phase typically lasts 4–8 wk. Thyroglobulin levels are elevated because of the destruction of thyroid follicles.
Ultrasound Imaging
Thyroid ultrasound shows heterogeneous, diffuse, hypoechoic and confluent areas, with no increase in the vascularity on color Doppler imaging (86). These abnormalities often revert to a near-normal pattern when the condition resolves (Fig. 7).

Ultrasound and scintigraphy images of 46-y-old woman with subacute thyroiditis arising in preexisting chronic autoimmune thyroiditis. At presentation, patient had tender goiter and pain while swallowing but no fever. Leukocyte count and erythrocyte sedimentation rate were abnormally increased, but C-reactive protein level was normal. TSH level was 0.01 mIU/L, with increased free T3 (almost 2-fold upper normal limit) and free T4 (1.5-fold upper normal limit). (Left) Axial (top) and longitudinal (bottom) ultrasound scans at baseline show markedly hypoechoic area in left thyroid lobe, with poorly defined margins. Anterior 99mTc-pertechnetate scintigraphy scan at presentation shows minimal tracer uptake in thyroid gland, with physiologic visualization of parotid and submandibular salivary glands; arrowhead indicates sternal notch. Axial (top) and longitudinal (bottom) ultrasonography scans obtained 1 y later show almost complete recovery of abnormalities observed on baseline ultrasound. Thyroidal hormonal profile was completely normal at this time.
Radionuclide Imaging
Thyroid scintigraphy is characterized by very low or absent tracer uptake in the thyroid gland in the thyrotoxic phase, a pattern shared by other conditions of destructive thyroiditis (e.g., type 2 amiodarone-induced thyroid dysfunction). Depending on the phase of the illness, tracer uptake can be absent in the whole gland or in part of the gland. Even when subacute thyroiditis affects primarily one lobe of the thyroid, the scan may show a completely absence of tracer uptake in the whole gland (Fig. 7) because of suppressed TSH levels due to a thyrotoxic phase of the disease.
Therapy of Subacute Thyroiditis
Since subacute thyroiditis is self-limited, in most cases the thyroid gland spontaneously resumes normal thyroid hormone production. Treatment is directed toward relief of thyroid pain. High-dose nonsteroidal antiinflammatory drugs are usually the first-line treatment (75). If neck pain does not improve after a few days, or if the patient presents with severe neck pain, corticosteroids may be considered (80), which leads to improvement within 2 d. After 5–7 d of high-dose prednisone, the dose is tapered over the next 2–4 wk. As the dose is tapered, most patients have no recurrence of symptoms, but occasionally symptoms do recur and the dose must be increased again.
Thyroid hormone supplementation is generally not necessary for the transient hypothyroid phase of subacute thyroiditis, unless patients are symptomatic. However, permanent hypothyroidism develops in up to 15% of patients, even more than 1 y after presentation (75).
Footnotes
Published online Feb. 2, 2021
Learning Objectives: On successful completion of this activity, participants should be able to have acquired knowledge on (1) the clinical manifestations, underlying pathophysiology, imaging modalities, and therapy of non-toxic nodular goiter; (2) the clinical manifestations, underlying pathophysiology, imaging modalities, and therapy of hypothyroidism; and (3) on the clinical manifestations, underlying pathophysiology, imaging modalities, and therapy of subacute thyroiditis.
Financial Disclosure: The authors of this article have indicated no relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, SAM, and other credit types, participants can access this activity through the SNMMI website (http://www.snmmilearningcenter.org) through July 2024.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.
- 49.
- 50.
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.
- 58.
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- Received for publication October 19, 2020.
- Accepted for publication January 27, 2021.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}