


Abstract
311
Introduction: Kinetic modeling and Patlak analysis of dynamic positron emission tomography (dPET) data can be used for a more accurate assessment of radiotracer uptake and metabolism. One promising use for dPET is with gallium-68 (68Ga) prostate specific membrane antigen (PSMA) PET for prostate cancer patients where dPET outperforms static PET in identifying cancerous lesions. This technique can further be employed as part of a theranostic approach were 69Ga-PSMA is used for imaging and Lutetium-177-PSMA (LuPSMA) is used for therapy. One factor holding back further research and clinical adoption of techniques, such as the one outlined above, is the need to acquire the arterial input function (AIF) when performing dPET imaging. The purpose of this study was to refine the design and then simulate a previously validated non-invasive positron detector, hereinafter called NID, developed to determine the AIF for dPET.
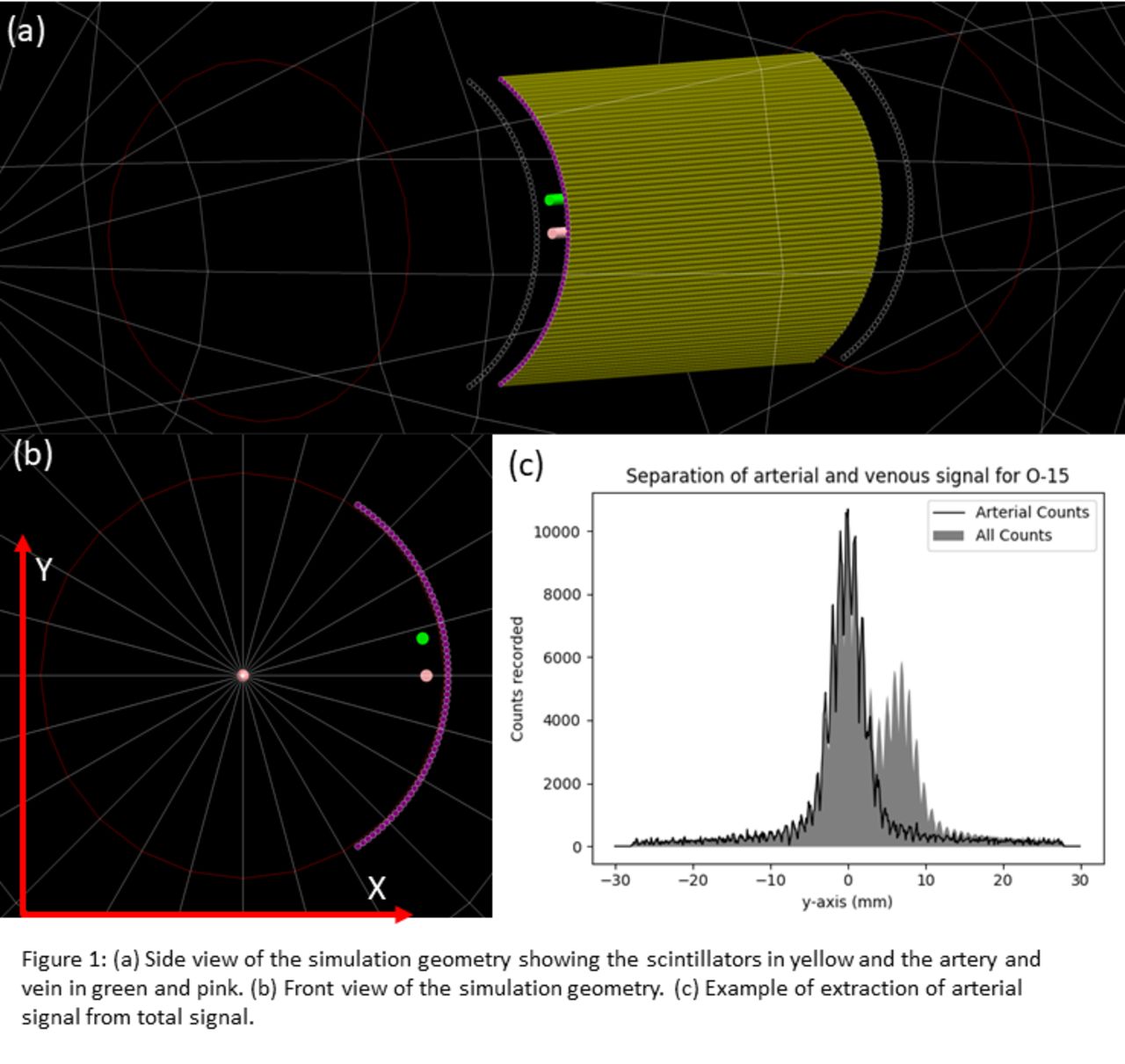
Methods: The NID was simulated using the Geant4 Monte Carlo toolkit. Particle transport was performed by using the Penelope low-energy electromagnetic physics and optical photon processes. The NID consisted of 64 plastic scintillating fibers, 0.97 mm in diameter and 10 cm long. These fibers had a 0.03 mm cladding layer and a 0.0250 mm plastic protective layer. Each end of the fibers was coupled to a photomultiplier tube (PMT) to collect photons in the visible range. These fibers were arranged in a single band wrapped around a 64.13 mm in diameter polyethylene cylinder that represents a patient’s wrist. Two 2.30 mm diameter cylinders were placed inside the wrist to simulate the radial artery and vein of a patient. These cylinders were 6 mm apart and 2 mm below the surface of the wrist. Figure 1 (a) shows a side view of the simulation geometry and figure 1(b) shows a front view of geometry. Simulations were performed by simulating decay events of either oxygen-15 (15O) or fluorine-18 (18F) where the decaying particles were randomly distributed between the artery and vein. Interactions were recorded when energy was deposited in the scintillator core. Total deposited energy in the scintillator was calculated and the location of interaction for each event was scored. The number of optical photons that accumulated in each PMT were also calculated. The data was analyzed using a python algorithm to separate the arterial signal from the venous signal. The location of interaction was determined by taking the PMT that had the highest signal per event.
Results: With 15O, the arterial signal produced a full width half max (FWHM) of 5.28 mm in the y-direction. The extracted arterial signal was 104 % of the true arterial signal. With 18F, the arterial signal produced a FWHM of 10.32 mm. The extracted arterial signal was 112 % of the true arterial signal. Figure 1(c) shows the peak signal separation for the 15O simulations. The algorithm was able to correctly determine the location of interaction in the scintillator with an accuracy of 98%.
Conclusions: The results from this study show that the NID has sufficient spatial resolution to distinguish between the radial artery and radial vein in a patient and is thus suitable to determine the AIF during dPET scans.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.