


Article Figures & Data
Figures
- FIGURE 1.
Examples of structural and functional imaging used in diagnosis of infection. (A) Plain radiography of 55-y-old man with diskitis–osteomyelitis after corpectomy. (B and C) CT and MRI of 23-y-old man with chronic diskitis–osteomyelitis. (D) Ultrasound of 4-y-old boy with perforated appendicitis and associated abscess. (E) 99mTc-methylene diphosphonate bone scan of right ulnar osteomyelitis. (Reprinted with permission of (25).) (F) 111In-WBC SPECT/CT of infected right knee arthroplasty. (Reprinted with permission of (25).) (G) 67Ga-citrate scan of 61-y-old man with infected endovascular graft of aortic arch. (Reprinted with permission of (74).) (H) 18F-FDG/PET of 66-y-old man with infected thoracic aorta endograft. (A–D) Red arrowhead indicates point of infection; (E–H) red arrowhead indicates increased tracer uptake.
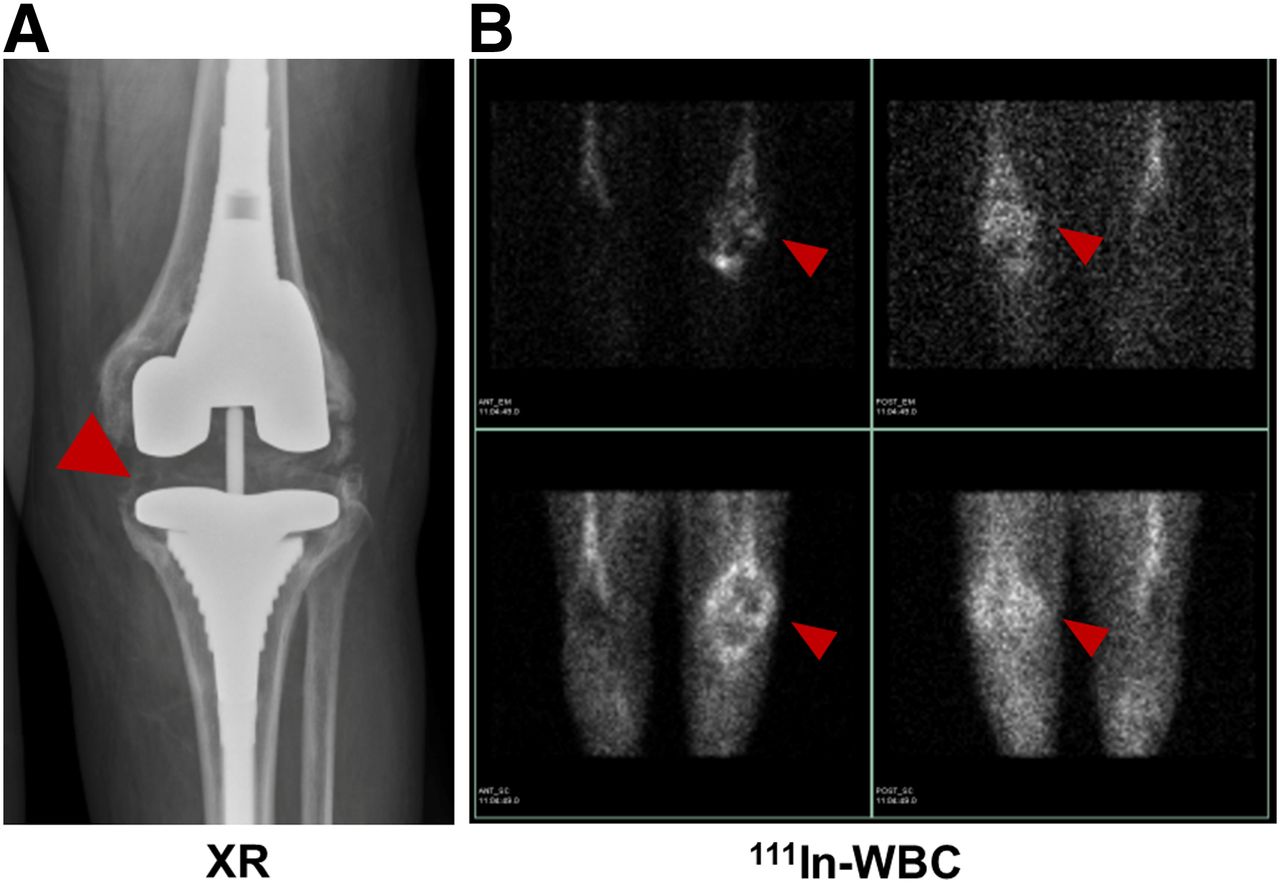
- FIGURE 2.
64-y-old woman with knee replacement and periprosthetic osteomyelitis (red arrowhead) as depicted via plain radiography (A) and radiolabeled 111In-leukocyte imaging (B, top row) demonstrates brightest uptake at medial aspect of tibial plateau. 99mTc-sulfur colloid imaging (B, bottom row) demonstrates no corresponding uptake in region of medial tibial plateau. Therefore, findings are consistent with osteomyelitis.
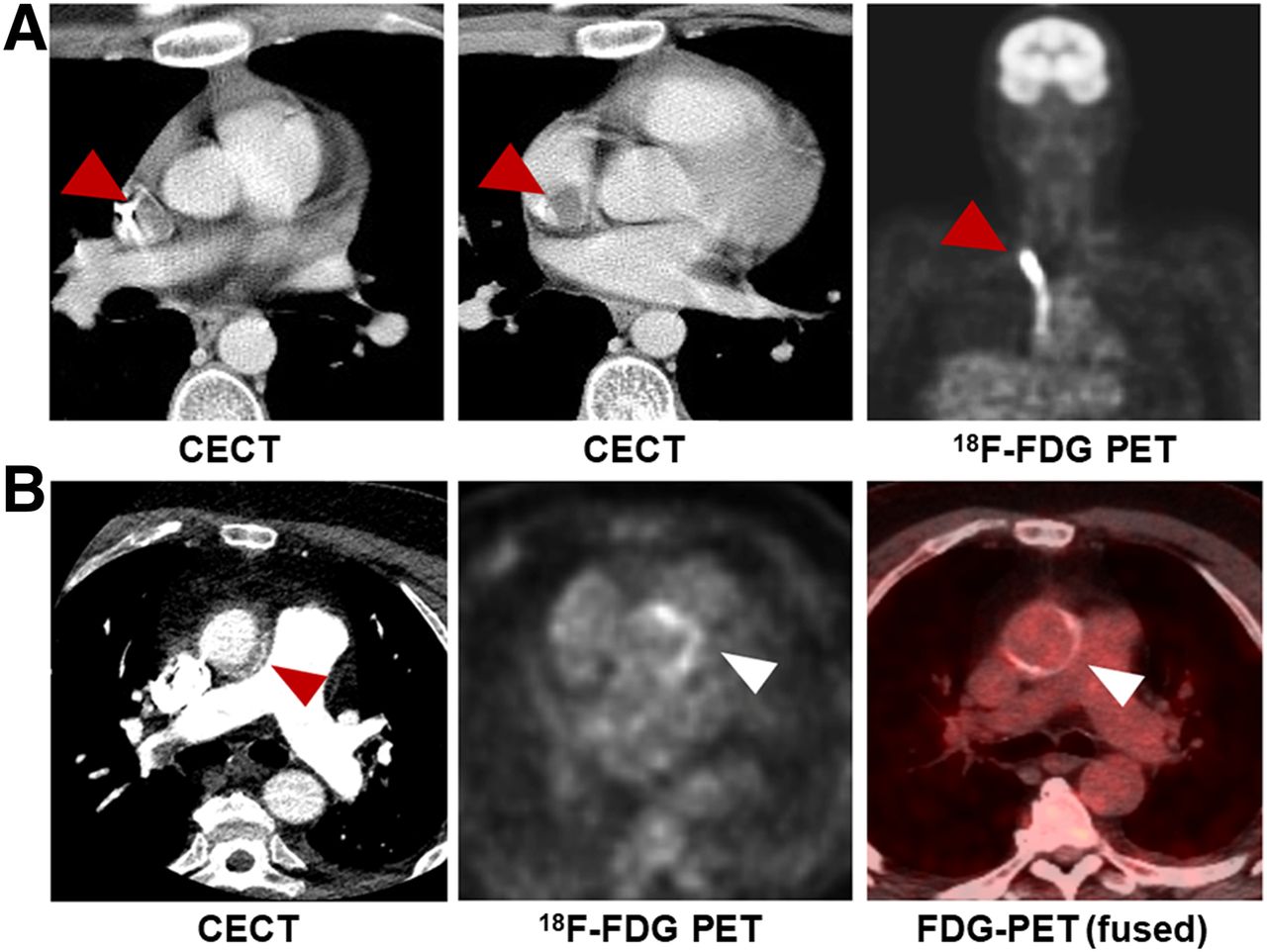
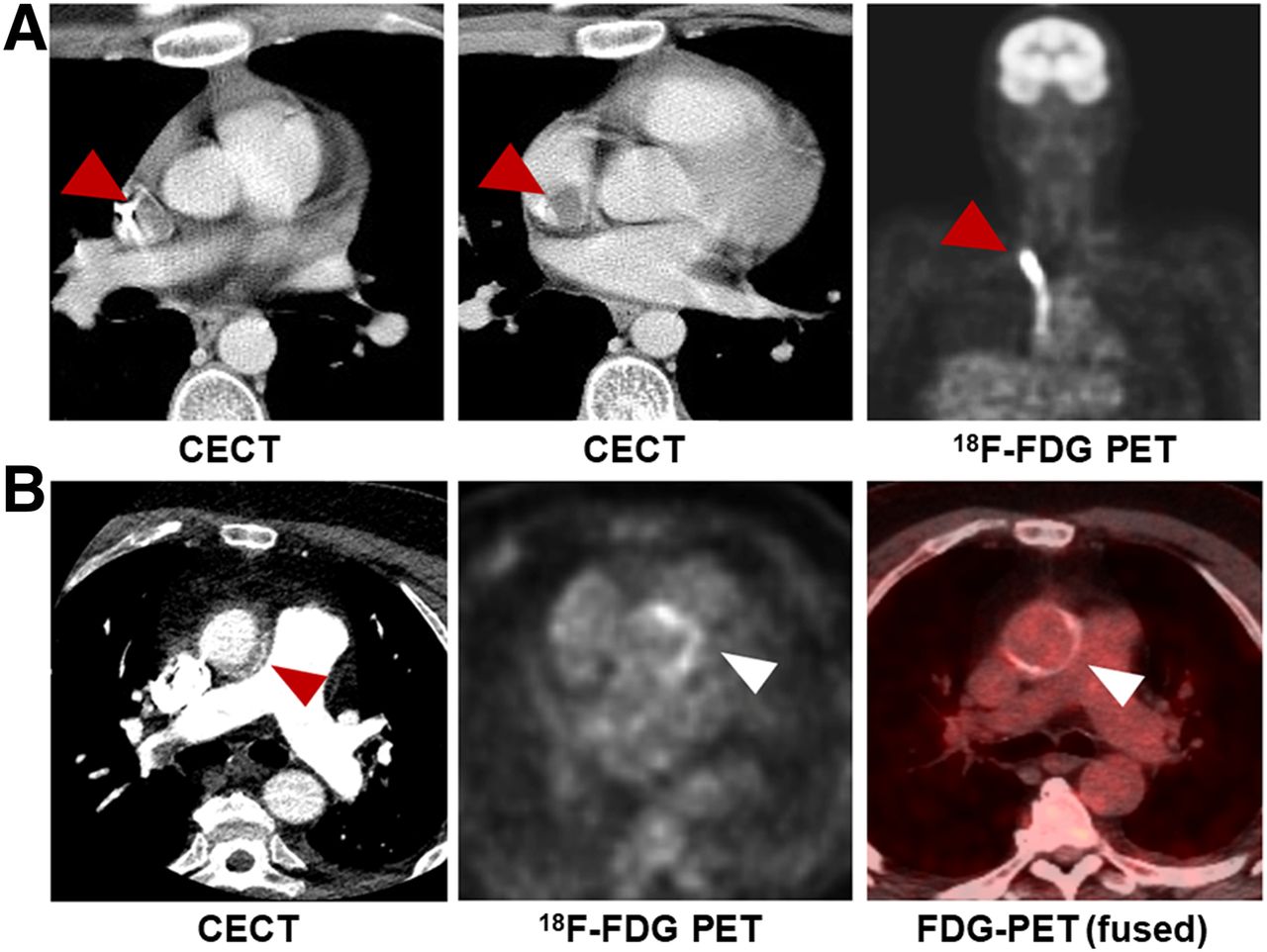
- FIGURE 3.
Examples of 18F-FDG PET in cardiovascular disease. (A) A 17-y-old boy with non-Hodgkin lymphoma, found to have catheter-associated thrombus consistent with infection, with arrowheads indicating increased FDG uptake in and around catheter. (B) A 59-y-old man with aortic valve prosthesis infection caused by E. faecalis, requiring surgical replacement. Arrowheads indicate increased uptake by valve. CECT = contrast-enhanced CT.
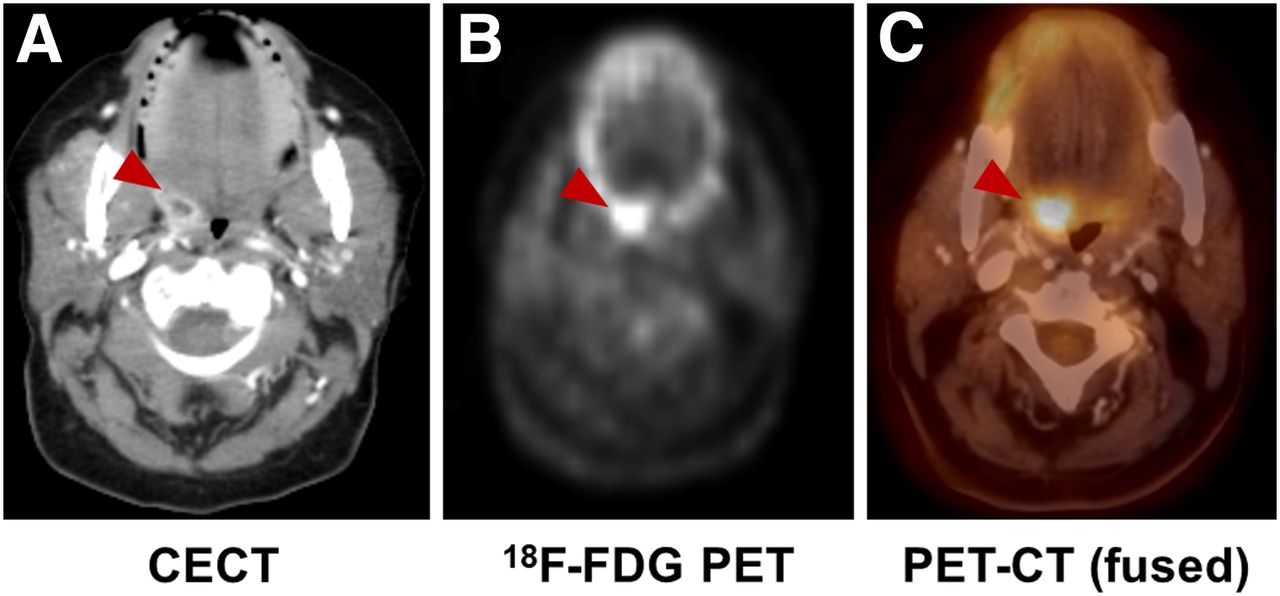
- FIGURE 4.
Incidental finding of infection in 65-y-old woman with fallopian tube cancer. (A) Contrast-enhanced CT shows tonsillar abscess (arrowheads). (B and C) Focal increase in uptake on 18F-FDG PET and 18F-FDG PET/CT in same location (red arrowhead).
- FIGURE 5.
Examples of novel non–sugar-based infection-targeted radiotracers for PET. (A and B) Increased uptake of radiotracers in infection compared with sterile inflammation in 2 rodent models: 18F-fluoropropyl-trimethoprim (FPTMP) uptake in mice infected with E. coli (arrowhead shows sterile inflammation, arrow shows infection) (A, reprinted with permission of (53)) and 18F-PABA uptake in rat infected with S. aureus (red arrows show sterile inflammation, yellow arrows show infection) (B, reprinted with permission of (64)). (C) 11C-d-Ala uptake in rat intervertebral disk infected with S. aureus (red arrowheads) and mouse lung infected with P. aeruginosa (red arrowheads). (Reprinted with permission of (73).) (D–F) Chemical structures of 18F-FPTMP (D), 18F-PABA (E), and 11C-d-Ala (F). ID = injected dose.
- FIGURE 6.
Examples of novel sugar-based infection-targeted radiotracers for PET/CT. (A–C) Increased uptake of radiotracers in infection compared with sterile inflammation in 3 rodent models: 18F-maltohexaose uptake in rat infected with E. coli (left arrows show infection, right arrows show sterile inflammation) (A, reprinted with permission of (57)), 18F-fluoromaltotriose uptake in mice infected with E. coli (yellow arrow shows infection site) (B, reprinted with permission of (59)), and 2-deoxy-2-18F-fluorosorbitol (18F-FDS) uptake in mice infected with E. coli (yellow arrows show infection, red arrows show sterile inflammation). (C, reprinted with permission of (61)). (D–F) Chemical structures of 18F-maltohexaose (D), 18F-fluoromaltotriose (E), and 18F-FDS (F), obtained from chemical reduction of 18F-FDG. CFU = colony-forming unit; ID = injected dose.




Tables
Radiotracer Target Main infectious indications Half-life Administered activity (MBq) Advantages Disadvantages Bone scan (99mTc-MDP) Active bone formation PBI* 6 h 500–1,110 Sensitive Low specificity SOM Low cost Susceptible to confounders (surgery, trauma) Late PJI Accessible Septic arthritis Good spatial resolution Necrotizing external otitis Low radiation dose WBC scan (99mTc-WBC) Leukocytes PBI† (violated bone) 6 h 185–370 Sensitive, especially for neutrophilic induced inflammation Depends on host immune system; sensitivity decreases after antibiotic treatment Diabetic foot Blood exposure Early PJI Requires sterility Infective endocarditis Time consuming Vascular graft infection Poor resolution FUO High radiation dose 67Ga-citrate Transferrin SOM 78.3 h 150–220 Suitable for immunodeficiency Delayed imaging Bacterial siderophores Opportunistic infections Poor resolution Neutrophilic lactoferrin FUO High radiation dose Necrotizing external otitis Expensive Requires cyclotron 18F-FDG PET Energy consumption PBI* 110 min 185–740 Sensitive Depends on host immune system SOM Suitable for acute and chronic inflammation Expensive Infective endocarditis High resolution Lacks widespread availability Vascular graft infection Relatively short scan Susceptible to confounders (e.g., surgery) FUO SUV quantification Requires patient preparation High radiation dose Tracer Mechanism Target bacterial pathogen Pathogens tested in vivo (CFUsadministered) Maximum infection-to-inflammation ratio Stage (published reports) 18F-FPTMP Inhibition of bacterial dihydrofolate reductase G+, G− E. coli (106–108) ∼3 (108 E. coli CFU) Preclinical S. aureus (108) P. aeruginosa (107) 18F-FAG Bacterial cell wall G+, G− E. coli (107) ∼2 Preclinical 18F-maltohexaose Maltodextrin transporter G+, G− E. coli (105–109) 7 (109 CFU) Preclinical 18F-fluoro-maltose Maltodextrin transporter G+, G− E. coli (108) 1.3 Preclinical 18F-fluoro-maltotriose Maltodextrin transporter G+, G− E. coli (106-108) 3.4 (108 E. coli CFU) Preclinical L. monocytogenes (2 × 105) P. aeruginosa (106) S. aureus 18F-FDS Bacterial energy consumption G−* E. coli (107) 7.3 (E. coli) Clinical S. aureus (107–108) P. aeruginosa (106.5) 11C-PABA Folic acid biosynthesis G+, G− E. coli 2.6 Clinical 18F-PABA Folic acid biosynthesis G+, G− S. aureus (107–108) 7.95 (108) Preclinical 11C-d-Met Bacterial cell wall G+, G− E. coli 2 Clinical S. aureus 11C-d-Ala Bacterial cell wall G+, G− E. coli (5 × 106) 3.5 (S. aureus) Preclinical S. aureus (5 × 106) P. aeruginosa (2 × 106) ↵* Enterobacteriaceae.
CFU = colony forming units; 18F-FPTMP = 18F-fluoropropyl-trimethoprim; G+ = Gram-positive bacteria; G− = Gram-negative bacteria; 18F-FAG = 2-deoxy-2-18F-fluoroacetamido-d-glucopyranose; 18F-FDS = 2-deoxy-2-18F-fluorosorbitol; 11C-d-Met = d-methyl-11C-methionine.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}