


Abstract
1137
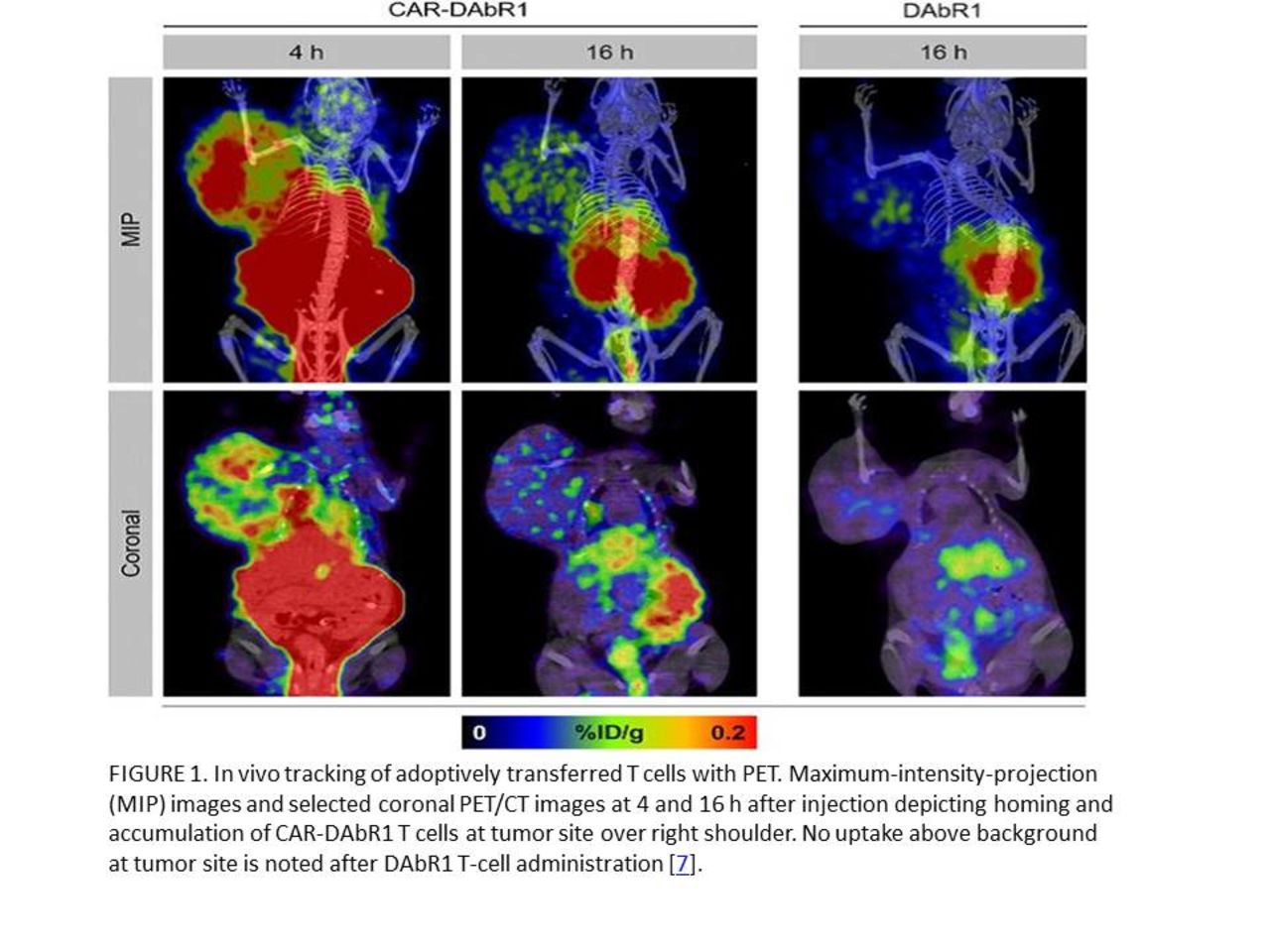
Introduction: Significant progress in chimeric antigen receptors (CAR) T cell therapy has been made and is led by the clinical success of CD19-CAR T cells against refractory B-cell malignancies[1]. Therapy efficacy relies on the successful trafficking of cells to their intended targets and the evaluation of this process could predict success or failure of the treatment. Only molecular imaging allows for spatially correlated surveillance of the cells of interest throughout the entire body. Beyond target accumulation at a single time point, the residence and potential secondary sites of T cell trafficking can also be monitored by positron emitting tomography (PET)[2]. In this educational exhibit we are going to discuss about different methods of monitoring transferred cell migration to the target organs, their advantages and disadvantages.1-Serum profiling of cytokines associated with T cell activation, direct enumeration of tumor-specific T cell numbers in peripheral circulation, and tumor biopsies. Changes in serum cytokine levels, reflect systemic immune response, illustrating not only the activation of adoptively transferred T cells, but also their effects on neighboring immune cells and dying tumor cells. In the case of a biopsy, sampling is restricted to a small part of a single site of disease[3].2-Bioluminescence imaging with use of luciferase reporter genes and optical imaging with use of dye-labeled cells are not practical for whole-body imaging because of the limited tissue penetration of light. Moreover, bioluminescence imaging requires transfection of luciferase, whose immunogenicity cannot be excluded[1].3-Magnetic resonance imaging with iron nanoparticle loaded cells has limited sensitivity due to the negative contrast of iron superimposed on a highly heterogeneous background[1].4-Radiolabeling of cells has multiple advantages and disadvantages. Administered radiolabeled cells can be monitored in the whole body with very high label-to-background ratios by using single photon emission computed tomography (SPECT) and PET. Indium 111- oxine labeling requires relatively high levels of radioactivity, which induces cellular damage. Moreover, imaging is limited to a few days after T-cell transfer, owing to radioisotope decay[3-5].5-Compared with SPECT, PET is at least 10 times more sensitive, potentiating reduction of radio-exposure of the cells by one log:a-Fluorine 18 (18F) fluorodeoxyglucose (FDG) has been used to label cells ex vivo, however, the half-life of 18F is short; moreover, dormant or inactivated cells with low glucose metabolism take up insufficient 18F FDG, and the cells can release 18F FDG via phosphatase activity[6].b-To lower radiation exposure while still obtaining high sensitivity, resolution, specificity, and sufficient duration to track the cells over multiple days, a long PET radioisotope is required. Zirconium 89 (89Zr) is a cyclotron-produced PET isotope with a half-life of 3.27 days and 89Zr-oxine has been used for labeling T-cells. However, the labeling process has the possibility to alter the T cells, and as the T cells multiply the label is diluted, limiting the duration of longitudinal studies[7].c-Stable transduction of T cells with a specific reporter gene allows for extended longitudinal studies using serial infusions of reporter-specific probes. This reporter gene should have a high binding affinity for a molecular imaging agent, would not be immunogenic, and would not result in detriment to efficacy of CAR-T-cell function when exposed to radiotracers. Stable expression of a reporter gene enables serial longitudinal imaging of cell trafficking, and as the reporter gene is passed on to the progeny cells, imaging of expanding cell populations is possible, thereby providing information about cell viability. The use of an antibody fragment provides a unique set of capabilities to CAR T cells, as PET, SPECT, or therapeutic isotopes can be delivered to the engineered immune cells[2, 8].

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.