


Abstract
398
Introduction: Cancer antigen 125 (CA-125) is used for monitoring disease status in post treatment patients of ovarian cancer as rising concentrations predict recurrence in most cases. Many studies have demonstrated that 18F-FDG PET/CT imaging is sensitive & a better modality when compared to conventional anatomical imaging in detection of recurrent disease in patients with raised CA-125 levels.
Objectives: The retrospective study was designed to determine: 1) If FDG PETCT can serve as an accurate maker to define and predict disease burden 2) If there exists any linear relationship between raised CA-125 levels and degree of disease burden 3) A possible CA-125 cutoff value which could predict whether the active disease predominantly involves lymph nodal stations or intra abdominal soft tissue (omental/peritoneal/mesenteric) sites.
Methods: 42 patients (35-74 years, Median 52 years) with suspected disease recurrence based on raised CA-125 levels referred for PET/CT examination were studied. Patients were classified into three groups based on range of CA-125 levels: Group A (35-175), Group B (175-350) and Group C (more than 350). Number of lesions per patient was counted in the following manner: Each lymph nodal station was given a score of 1; Each segment of liver was given a score of 1 irrespective to of number of lesions present in that segment.; Peritoneal soft tissue deposit along the surface of an organ was given a score of 1 and omental, mesenteric and serosal deposits were assigned a score of 1 individually. Data analysis was done using appropriate statistical tests. To arrive at a possible cutoff value for CA-125, various levels of CA-125 were analysed using Chi square test.
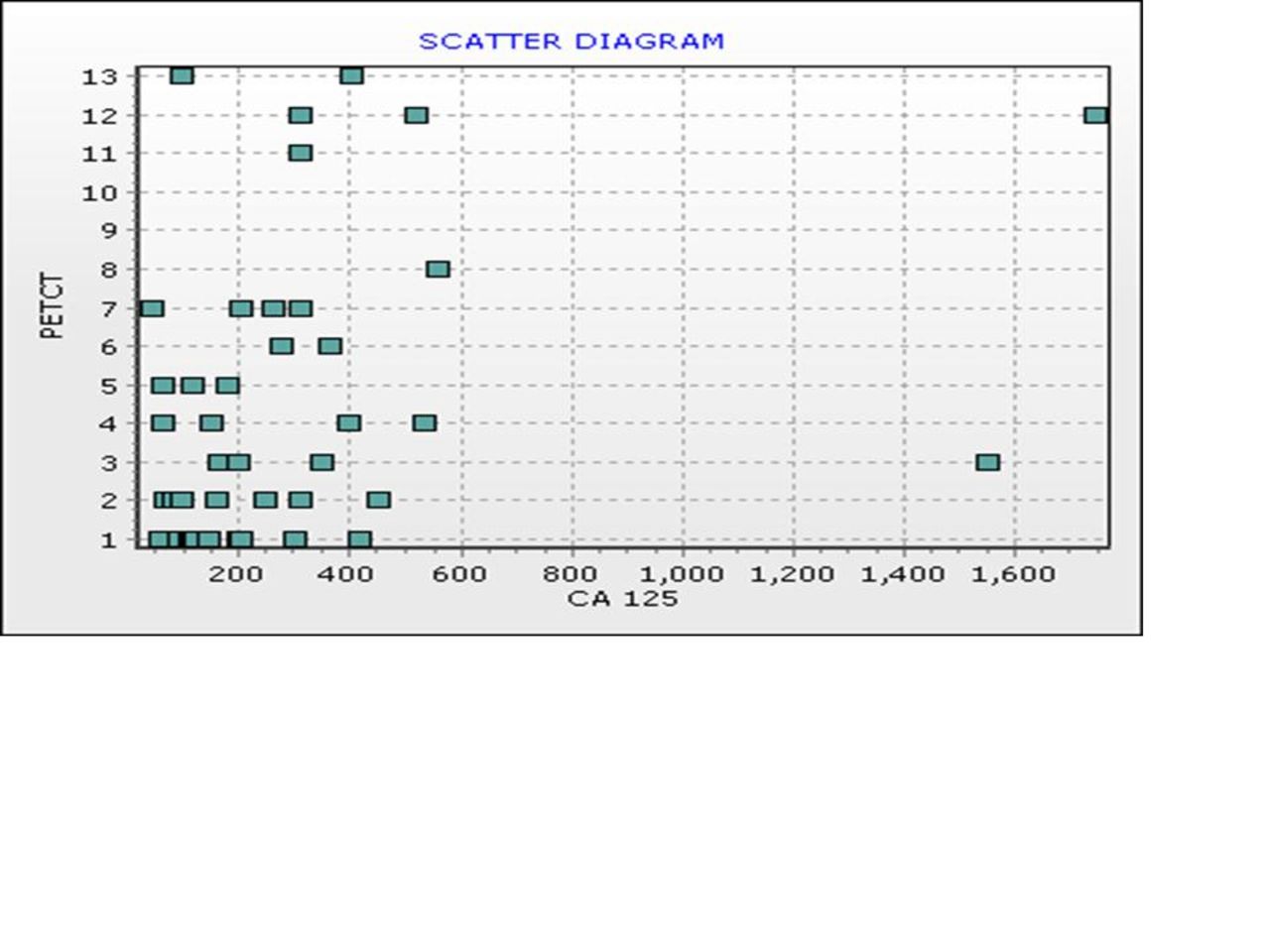
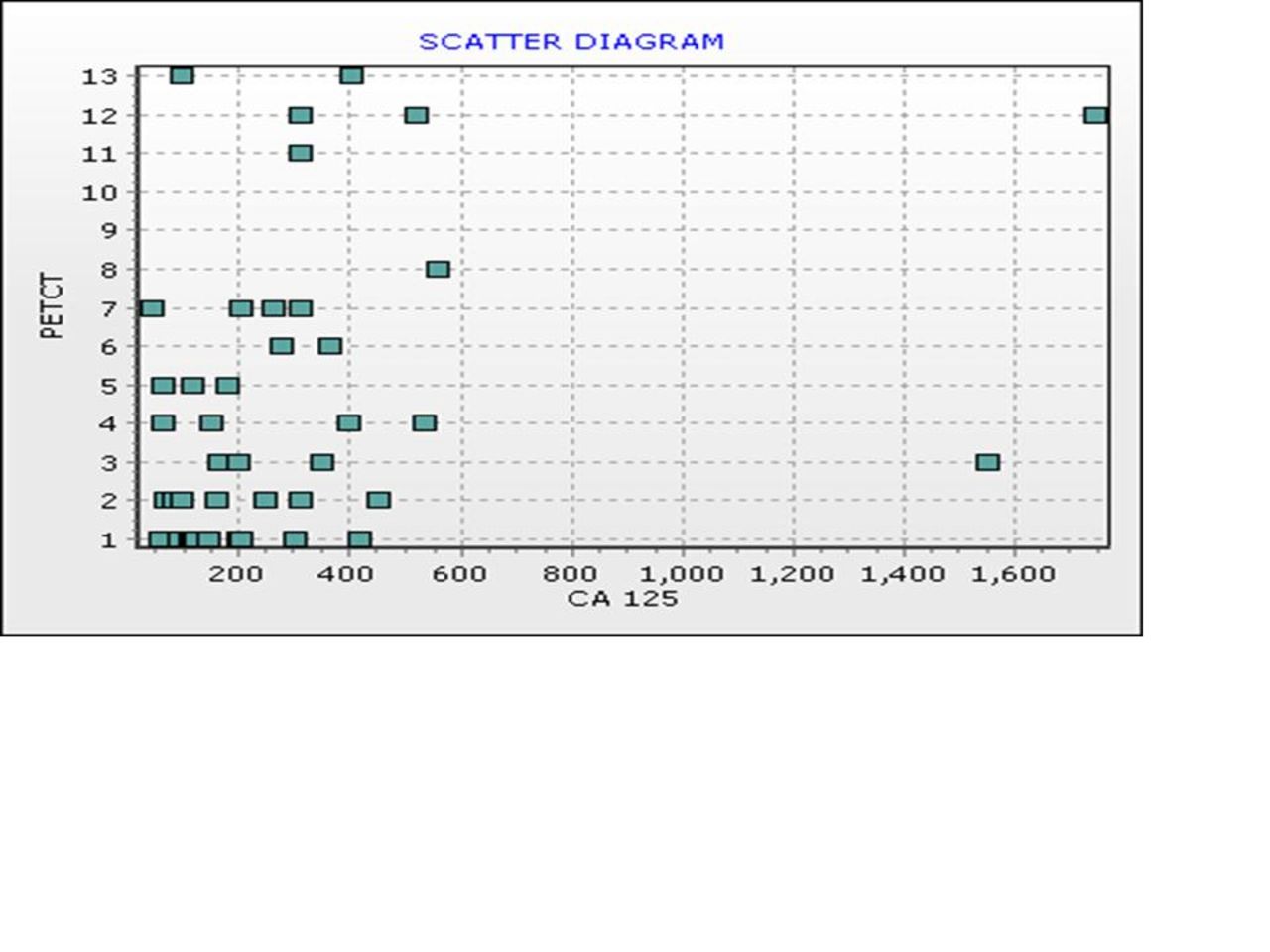
Results: PET/CT detected a total of 57 lesions in Group A (n=18), 68 in Group B (n=14) and 65 lesions in Group C (n=10) respectively. No significant statistical difference was found in total no of lesions detected in all the three groups with different levels of CA-125 (One Way ANOVA: p value 0.071). When comparing total no of lesions detected on PET/CT in groups with marked difference in CA-125 levels - Group A (CA-125: 35-175) and Group C (CA-125: >350), no significant statistical difference was seen (Proportional test: p value 0.380). Also, when number of lesions detected on PET/CT in each patient was correlated with the respective CA-125 levels and data analysed using Spearman Correlation coefficient, no correlation (r = 0.342) between the CA-125 levels and disease burden was observed. Scatter diagram given below depicts X axis: number of PET/CT lesions and Y axis: Level of CA-125. Using Chi square test, a cut off CA-125 value of 350 was established to be significant (p value <0.001) in suggesting whether the active disease predominantly involves lymph nodal or intra abdominal soft tissue sites. In our study, lymph nodal metastases were more common in patients with CA-125 value less than/equal to 350 (n=32/42, 76.2%) & soft tissue deposits were more common in patients with CA-125 levels more than 350 (n=10/42, 23.8%).
Conclusions: Whole body FDG PETCT imaging serves as a reliable, accurate marker of disease recurrence in treated cases of Ca Ovary with raised CA 125 levels. There exists no relationship between CA-125 levels and degree of disease burden. This suggests that PETCT can detect higher degree of disease burden even in patients with low levels of raised CA-125 and vice versa. A cutoff of 350 of CA-125 may be useful to predict the predominant disease distribution pattern i.e. lymph nodal stations versus soft tissue deposits in these patients.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.