


Abstract
1627
Objectives: Radiation Safety
Purpose: Detail the successful decrease of radioactivity contamination levels in Nuclear Medicine restrooms with the addition of Hands-Free utilities and altered water pressure.
Background: When considering excretion of a many commonly used nuclear medicine radiotracers, a large majority are eliminated via urination. Our group queried whether levels of residual, potentially harmful radioactive material on commonly contacted surfaces in department bathrooms were present, and if so how could we intervene to attempt decreasing risk of inadvertent contamination from patients to employees, or other hospital-goers.
Methods: First, we established a threshold for significant radioactivity using the Society of Nuclear Medicine and Molecular Imaging mandated measurements and critical radioactive thresholds in designated examination rooms and nuclear medicine work rooms (>200 counts above background). For twenty weekdays, at mid-day we obtained radioactive contamination measurements of commonly contacted surfaces in the nuclear medicine(NM) and PET/CT bathrooms from the door handle, light switch, faucet, soap dispenser, floor, flush handle, and toilet seat(using the usual swipe testing technique). Once our results were gathered, we met with our hospital engineering department, and environmental services to discuss a plan to bolster safety in these restrooms. Our intervention included the installation of motion sensor based light switch, toilet flusher, automatic soap dispenser, and sink faucet. Additionally, we added disposable toilet seat covers and decreased the flush pressure of both toilets by approximately 30% in an effort to decrease a splash effect. Using the same technique as before, we re-evaluated for surface radioactive contamination on the same surfaces and assessed for change in contamination. All our measurements were corrected for background.
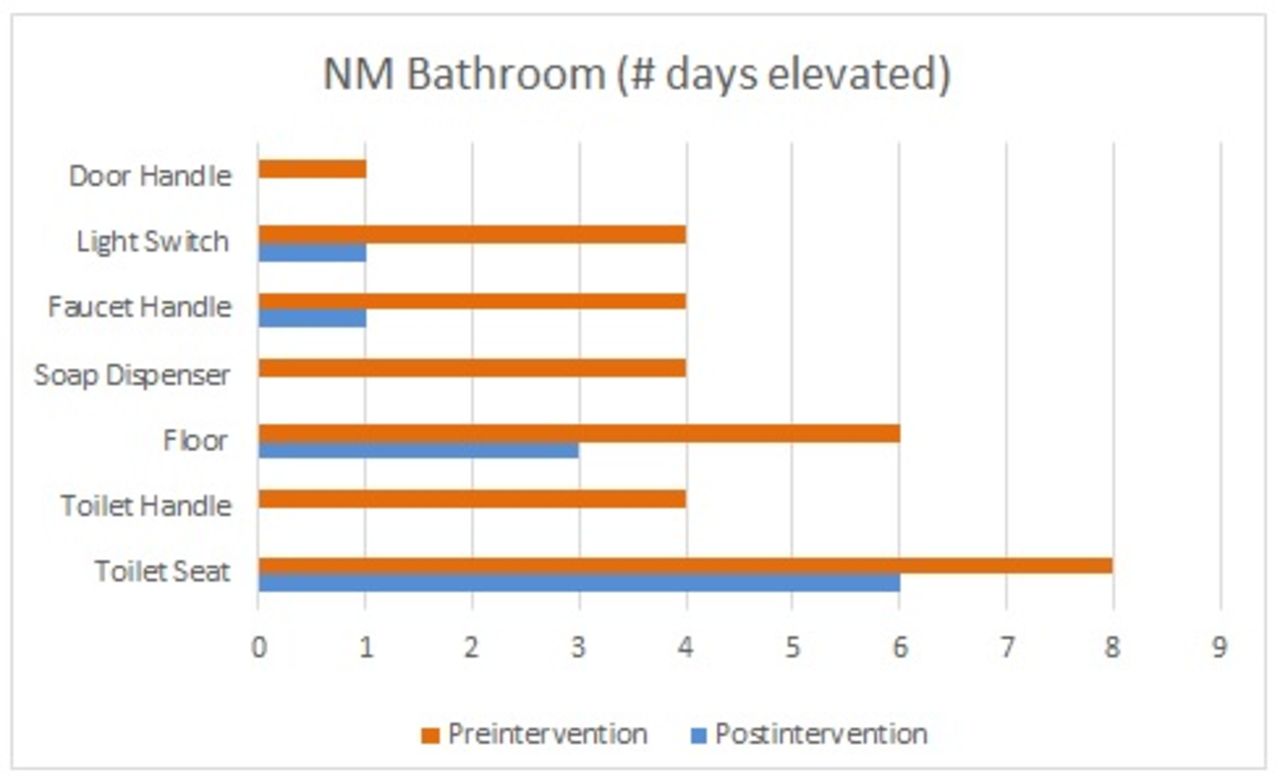
Results: Prior to the Hands-Free conversion, the number of days of critical radioactive thresholds was determined in each bathroom on the door handle, light switch, faucet, soap dispenser, floor, flush handle, toilet seat and repeated after conversion as shown in the graphs below. Among the two observation periods, the max contamination was observed up to approximately 518,000 cpm above background (on a post intervention toilet seat). While it is difficult to completely resolve surface contamination, there were significant improvements on all surfaces overall. After the conversion, the level of the absolute percent decrease in number of days with critical contamination for each surface were: NM (100, 75, 75, 100, 50, 100, 25) and PET/CT (100, 66, 75, 100, 43, 33, 66) respectively. While most of the contamination was related to Tc-99m, other radionuclides were also identified reflecting those used in the department.
Conclusions: Restrooms located in close proximity to the nuclear medicine department carry a potential risk of transient contamination due to the mostly urinary excretion of radioactive tracer. As a patient may unknowingly leave radioactive contaminated bodily excretions on most of the bathroom surfaces, this can cause potential cross contamination to hospital staff and other hospital goers. We have demonstrated that eliminating the requirement of hand contact and with bathroom surface fomites and decreasing “splash back” from powerful water flushing that there is a potential to decrease and/or actually eliminate the risk of inadvertent radioactivity transfer in keeping with ALARA.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.