


Abstract
1163
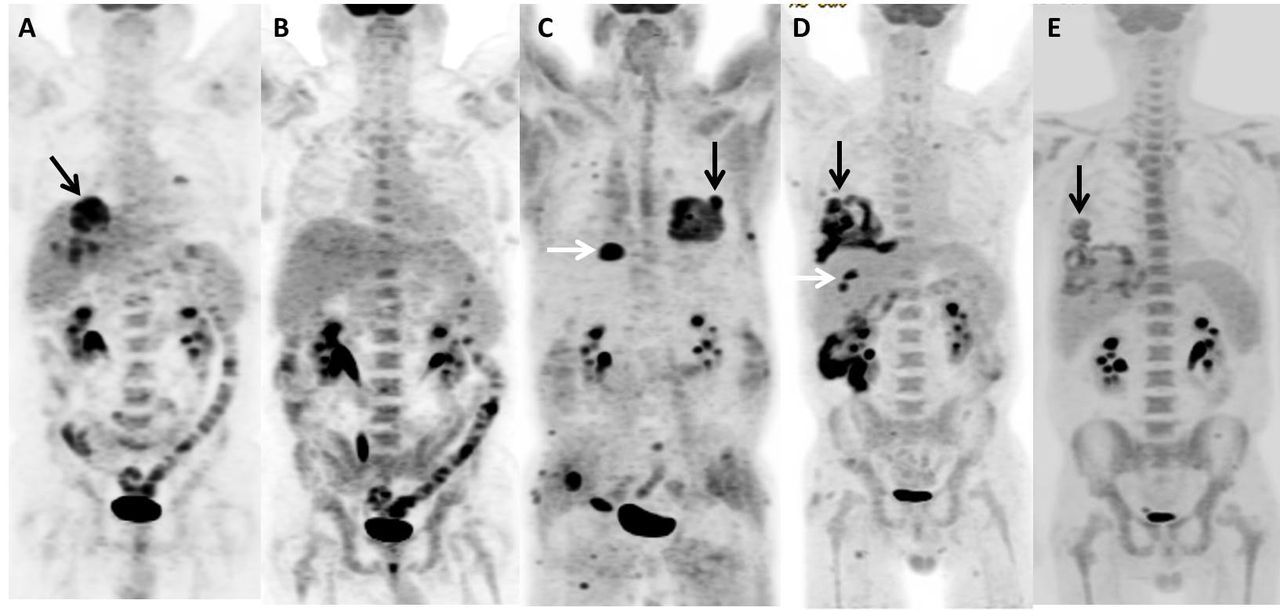
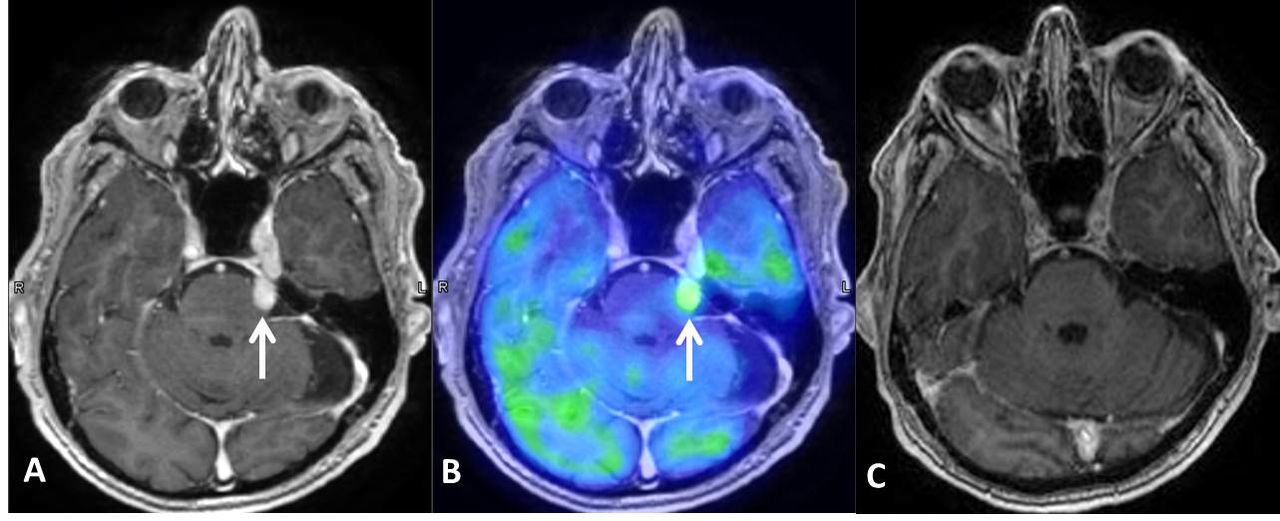
Objectives: Lymphomatoid granulomatosis (LYG) is a rare T-cell rich, Epstein-Barr virus (EBV) - positive B-cell lymphoproliferative disorder and predominately involves the lung, followed by skin, central nervous system (CNS) and kidney. Histopathological diagnosis of pulmonary LYG (PLYG) relies on the cytologic atypia and density of clonal EBV-positive B cells from the lung specimen, with the latter determining its grade and guiding clinical management. High grade (WHO grade 3) LYG is prone to progress to malignant lymphoma and has favorable response to chemotherapy. The aim of this study is to define the role of 18F-FDG PET/CT in surveillance of high grade PLYG in its clinical course. Methods We retrospectively reviewed the patient’s chart and sequential 18F-FDG PET/CT imaging findings in a cohort of histopathological confirmed pulmonary LYG patients. The clinical presentation, pulmonary and extra-pulmonary tissue sample microscopic findings, including Epstein-Barr virus -encoded RNA (EBER) in situ hybridization results, were also analyzed. Results There were five WHO grade 3 pulmonary LYG patients included in this study, with age range 49 - 56 years old. All patients had lung biopsy proven WHO grade 3 (>50 EBV-positive B cells/high power field). Another two patients with biopsy proven WHO grade 1(<5 EBV-positive B cells/high power field) were identified during chart review, but not included. The clinical behavior in this small cohort varied from indolence to nonspecific constitutional symptoms, including cough, fever, rash, weight loss, chest pain and neurological abnormalities. On pre-treatment 18F-FDG PETCT scan, all patients presented with multiple hypermetabolic pulmonary nodules, mass lesions, airspace consolidation, with and without associated small amount non-hypermetabolic pleural effusion. The imaging findings mimicked pulmonary neoplasm and infectious/inflammatory etiologies. The degree of FDG uptake of pulmonary lesions also varied. Following rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone (R-CHOP) chemotherapy, all patients demonstrated favorable response initially. However, subsequent 18F-FDG PETCT scans showed recurrent hypermetabolic lung lesions in 4 patients, with 2 of them had biopsy proven recurrent grade 3 PLYG; and 2 had biopsy proven fungus infection related to immunocomprised status. One patient with relapsed grade 3 PLYG also exhibited concurrent multiple subcutaneous hypermetabolic lesions on 18F-FDG PET/CT and left trigeminal nerve involvement on brain MRI. The most FDG avid cutaneous lesion was biopsy proven grade 1 cutaneous LYG. Following alternative chemotherapy regimen, both the lung and cutaneous lesions demonstrated favorable response to therapy. The left trigeminal nerve lesion also resolved after palliative radiation therapy (Figures 1-3).
Conclusions: Discordant grading between PLYG and concomitant cutaneous LYG based on EBV positivity is a diagnostic and prognostic pitfall. Tissue sample diagnosis of lung lesion is more accurate than cutaneous lesion in disease grading, and should be performed in the scrutiny of lymphomatous transformation. The 18F-FDG PET /CT is a valuable imaging tool in monitoring disease activity, depicting multi-system distribution pattern and evaluation of response to chemotherapy, as well as guiding lesion biopsy to further aid clinical management.



In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.