


Article Figures & Data
Figures
- FIGURE 1.
SSTR-RADS-1A. Coronal 68Ga-DOTATOC PET whole-body maximum-intensity projection (A) demonstrating physiologic tracer distribution. No sites of abnormal uptake can be appreciated. Normal biodistribution of agent is seen, including uptake in pituitary gland, thyroid, adrenal glands, bowel, liver, and spleen (18,19). Radiotracer is excreted via urinary tract. Arrow indicates physiologic finding in uncinate process, which is also demonstrated by axial 68Ga-DOTATOC PET (B), axial CT (C), and axial 68Ga-DOTATOC PET/CT (D).
- FIGURE 2.
SSTR-RADS-1B. Image of patient with increased Chromogranin A levels, referred for initial staging. Axial 68Ga-DOTATOC PET (A), axial CT (B), and axial 68Ga-DOTATOC PET/CT (C) demonstrating increased uptake in prostate (arrow), for example, caused by prostatitis or due to benign prostatic hyperplasia.
- FIGURE 3.
SSTR-RADS-2. Likely benign skeletal finding with uptake in patient with NET of pancreatic origin (G1, Ki-67 = 2%). Axial CT (A), axial 68Ga-DOTATOC PET (B), axial 68Ga-DOTATOC PET/CT (C), and coronal CT (D) showing lytic-appearing lesion involving inferior endplate of lumbar vertebral body (arrow). Strongly suspected to be degenerative (a Schmorl’s node), this intravertebral disk herniation would be classified as SSTR-RADS-2.
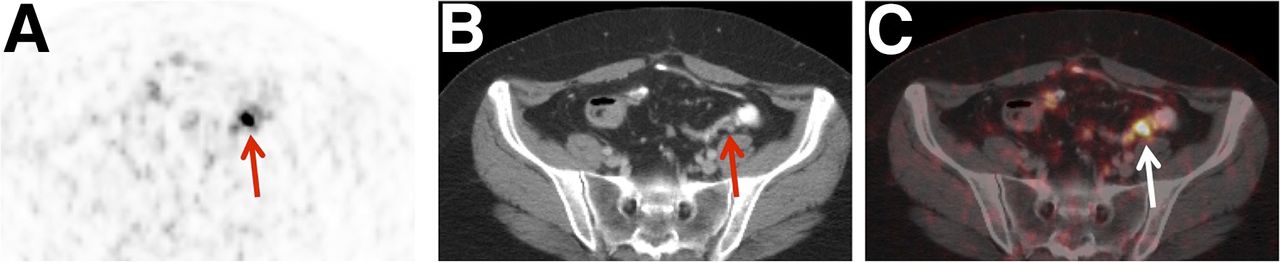
- FIGURE 4.
SSTR-RADS-3A. Low-level uptake in mesenteric lymph node in midabdomen of patient diagnosed with ileal NET (G1, Ki-67 = 2%). Axial 68Ga-DOTATOC PET (A), axial CT (B), and axial 68Ga-DOTATOC PET/CT (C) show small (short-axis diameter, <0.5 cm) mesenteric lymph node (arrow). Degree of focal uptake was above blood pool but lower than liver (not shown), and follow-up imaging (after 3 mo) was recommended. Depending on local practice pattern, biopsy might be considered (although biopsy of this site is difficult).
- FIGURE 5.
SSTR-RADS-3B. Moderate uptake in bone lesion in patient with small bowel NET (G2). Axial 68Ga-DOTATOC PET (A), axial CT (B), and axial 68Ga-DOTATOC PET/CT (C) show radiotracer uptake in right fifth rib (arrow). Because of CT findings along with moderate uptake on PET, follow-up imaging was recommended.
- FIGURE 6.
SSTR-RADS-3C. Patient with right invasive, lobular breast cancer (pT3, N1, M1 (liver)). Axial 68Ga-DOTATOC PET (A), axial CT (B), and axial 68Ga-DOTATOC PET/CT (C) demonstrating intense uptake in remaining right breast (a site highly atypical for NET lesion) (arrow, level 3).
- FIGURE 7.
SSTR-RADS-3D. Non–radiotracer-avid liver lesion in patient with G2 NET of pancreatic origin with history of cold and hot somatostatin analog treatment (2 cycles of PRRT; cumulative activity, 15.4 GBq of 177Lu-DOTATOC). Axial CT (A), axial 68Ga-DOTATOC PET (B), and axial 68Ga-DOTATOC PET/CT (C) show a 2.8-cm hepatic metastasis with negligible uptake above liver background (arrow). 18F-FDG PET was recommended to assess underlying intratumoral heterogeneity/dedifferentiation, with eventual need for PET-guided biopsy being likely.
- FIGURE 8.
SSTR-RADS-4. Patient with ileocecal NET (Ki-67 2%, G1), with radiotracer-avid lymph node in lower left abdomen that is too small to consider definitively disease-involved on conventional imaging. Axial 68Ga-DOTATOC PET (A), axial CT (B), and axial 68Ga-DOTATOC PET/CT (C) images show degree of uptake consistent with metastatic NET lesion (arrow, level 3). However, because short-axis diameter of lymph node was 0.6 cm (i.e., <1.0 cm), this node would generally not be considered pathologically enlarged on CT.
- FIGURE 9.
SSTR-RADS-5. Image of patient with extensive SSTR-positive liver lesions. Axial CT (A and B), axial 68Ga-DOTATOC PET (C), and axial 68Ga-DOTATOC PET/CT (D) clearly demonstrating 2 intrahepatic lesions with intense radiotracer uptake (level 3) and corresponding findings on CT (arrow). This scan would be categorized as SSTR-RADS-5. PRRT could definitely be considered.
- FIGURE 10.
Defining overall SSTR-RADS score. Example of patient with colorectal NET (Ki-67 < 2%, G1 NET). Axial/coronal (insert) CT (A), axial 68Ga-DOTATOC PET (B), and axial 68Ga-DOTATOC PET/CT (C) reveal equivocal tracer uptake in degenerative, intravertebral disk herniation (most likely a Schmorl’s node, SSTR-RADS-2, arrow). However, axial 68Ga-DOTATOC PET (E) and axial 68Ga-DOTATOC PET/CT (F) clearly demonstrate intense uptake in liver lesion in segment III, which cannot be detected on axial CT (D) (SSTR-RADS-4), highly consistent with liver metastasis. Additionally, intense uptake in pathologically enlarged lymph node close to hilum of liver (arrow) can also be identified on both imaging modalities. As latter would be classified as SSTR-RADS-5, “highest” SSTR-RADS lesion will also designate overall PET score (i.e., SSTR-RADS-5 in this case, “overruling” other lesions). PRRT could be considered.









Tables
SSTR-RADS Finding Uptake level* PRRT?† 1 (benign) Known to be benign (confirmed by previous biopsy or with pathognomonic appearance on conventional/anatomic imaging). 1A Benign lesion, characterized by biopsy or in accordance to anatomic imaging and without any abnormal uptake (Fig. 1). 1 Not to be considered. 1B Benign lesion, characterized by biopsy or in accordance to anatomic imaging but with increased (focal) uptake (e.g., prostatitis, benign prostatic hyperplasia [Fig. 2], or thyroid adenoma [Supplemental Fig. 1]). 2–3 Not to be considered. 2 (likely benign) Soft-tissue site atypical of metastatic NET (e.g., axillary lymph nodes); equivocal uptake in bone lesion atypical for NET (e.g., strongly suspected to be degenerative, Fig. 3). 1 Not to be considered. 3 Further workup (biopsy, if sampling is possible) or follow-up (f/u) imaging might be required. 3A Suggestive of, but not definitive for, NET. 1–2 Not to be considered. Equivocal uptake in soft-tissue sites typical for NET metastases, such as in regional lymph nodes (LNs, Fig. 4). Biopsy or initial f/u imaging (SSTR PET or whole-body MRI after 3 mo) might confirm diagnosis, also depending on Ki-67/grading (21). 3B Suggestive of, but not definitive for, NET. 1–2 Single lesions: locoregional procedure; increased number of lesions: PRRT. Uptake in bone lesions not atypical for NET (Fig. 5). Initial f/u imaging (SSTR PET or whole-body MRI f/u after 3 mo) might confirm diagnosis, also depending on Ki-67/grading (21). 3C Suggestive of an SSTR-expressing, non-NET benign tumor or malignant process. 3 Not to be considered. Intense uptake in a site (highly) atypical for NET, for example, breast uptake (Fig. 6) (20). Tissue confirmation of tumor histology should be considered. 3D High likelihood for malignant NET lesion, but negative on a SSTR PET scan. Not available Not to be considered.‡ Anatomic imaging representing lesion highly suggestive of being malignant (dedifferentiated NET or another type of malignancy), but demonstrating no SSTR uptake (e.g., single dedifferentiated liver metastasis, Fig. 7, or a non-NET malignancy) (6,25). 18F-FDG PET might be of value (11,26,27). Tissue confirmation of tumor histology should be considered. 4 (NET highly likely) Positive uptake in site typical for NET lesion but lacking definitive findings on anatomic imaging. 3 To be considered.¶ Intense uptake in common site typical for NET lesion, but without confirmatory findings on anatomic imaging (e.g., bone lesions or small LN, which is nonsuggestive on a conventional CT scan, Fig. 8). Because of high sensitivity and specificity of SSTR PET imaging, further confirmation by biopsy might be not necessary. 5 (NET almost certainly present) Intense uptake in site typical for NET with corresponding findings on conventional imaging. 3 Definitely to be considered. An example would be a SSTR-expressing liver lesion with corresponding findings on a CT scan (Fig. 9). ↵* Uptake levels, a 3-point qualitative assessment for defining the level of uptake (Table 2).
↵† PRRT using 177Lu-/90Y-radiolabeled somatostatin analogs. Inclusion and exclusion criteria according to The Joint International Atomic Energy Agency, European Association of Nuclear Medicine, and Society of Nuclear Medicine and Molecular Imaging Practical Guidance as well as The European Neuroendocrine Tumor Society Consensus Guidelines still apply (3,23).
↵‡ Depends on grading, overall tumor burden, kidney and bone marrow function, and overall SSTR expression (e.g., G2 NET patient with entirely all lesions demonstrating SSTR expression, but a single dedifferentiated lesion; a combined treatment of PRRT together with a locoregional procedure could be considered) (28,29).
↵¶ On the assumption that an SSTR PET–avid lesion in a typical distribution has a very high probability of representing NET, PRRT might be considered.
- TABLE 2
A 3-Point Qualitative Assessment Scoring for Defining Uptake Level in an SSTR-Avid Lesion on a SSTR PET Scan
Uptake score Relative uptake Level 1 Uptake ≤ blood pool Level 2 Uptake > blood pool but ≤ physiologic liver uptake Level 3 Uptake > physiologic liver uptake
Supplemental Data
Files in this Data Supplement:





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.