


Article Figures & Data
Figures
- FIGURE 1.
18F-FDG PET/CT scan of 72-y-old man with proven chronic Q fever, infected endovascular aortic graft, and psoas abscess (arrows). Patient had vascular surgery 6 mo after initiation of antibiotic therapy with doxycycline and hydroxychloroquine because of severity of infection. Four years later, patient was still on antibiotic treatment because of persisting chronic Q fever infection.
- FIGURE 2.
18F-FDG PET/CT scan of 67-y-old man with history of acute Q fever and analysis because of severe fatigue. Serology for C. burnetii showed increased antiphase 1 IgG; PCR on blood was negative for C. burnetii. Transesophageal echocardiography was negative for endocarditis, but 18F-FDG PET/CT showed highly increased 18F-FDG uptake of patient’s native mitral valve (arrows). Patient was treated for almost 2 y with antibiotic therapy because of chronic Q fever endocarditis.
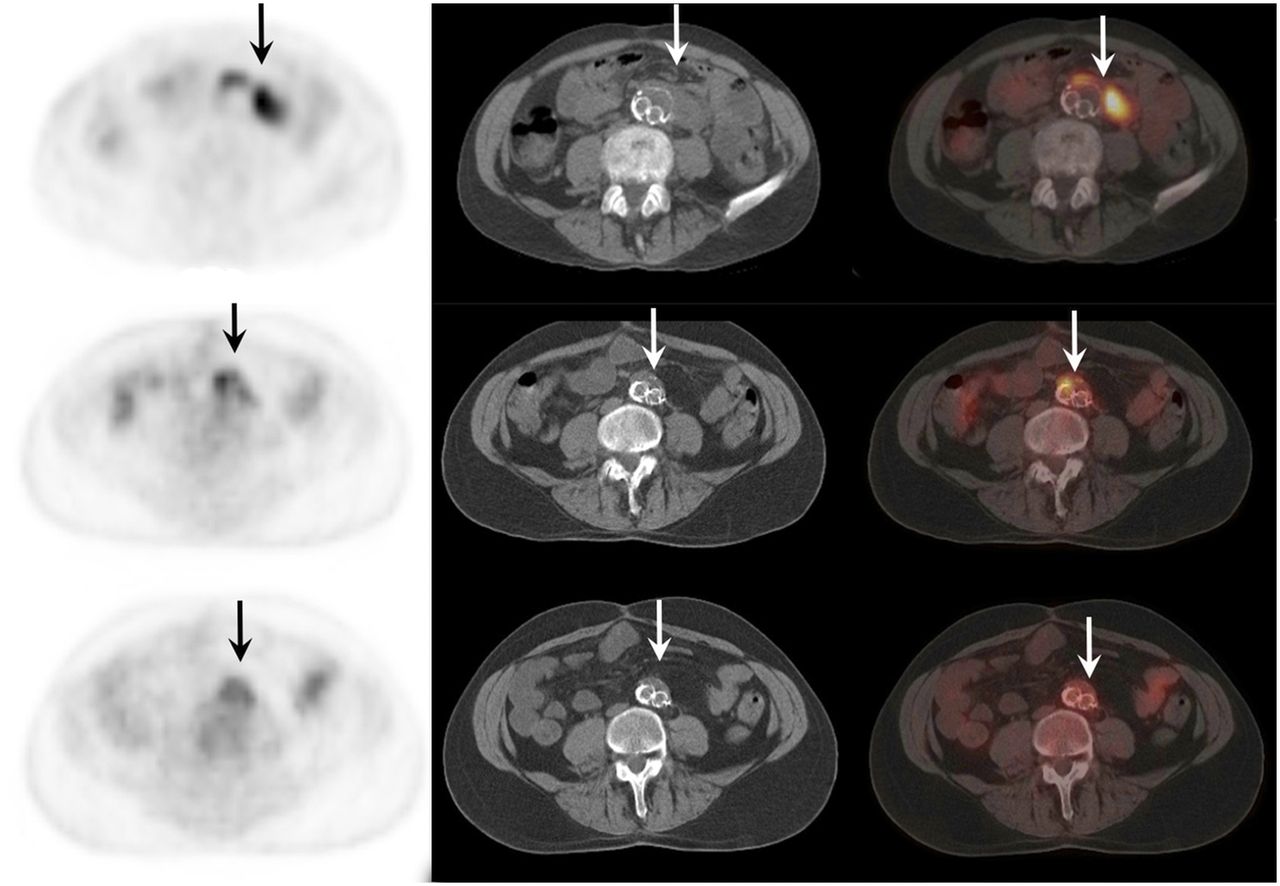
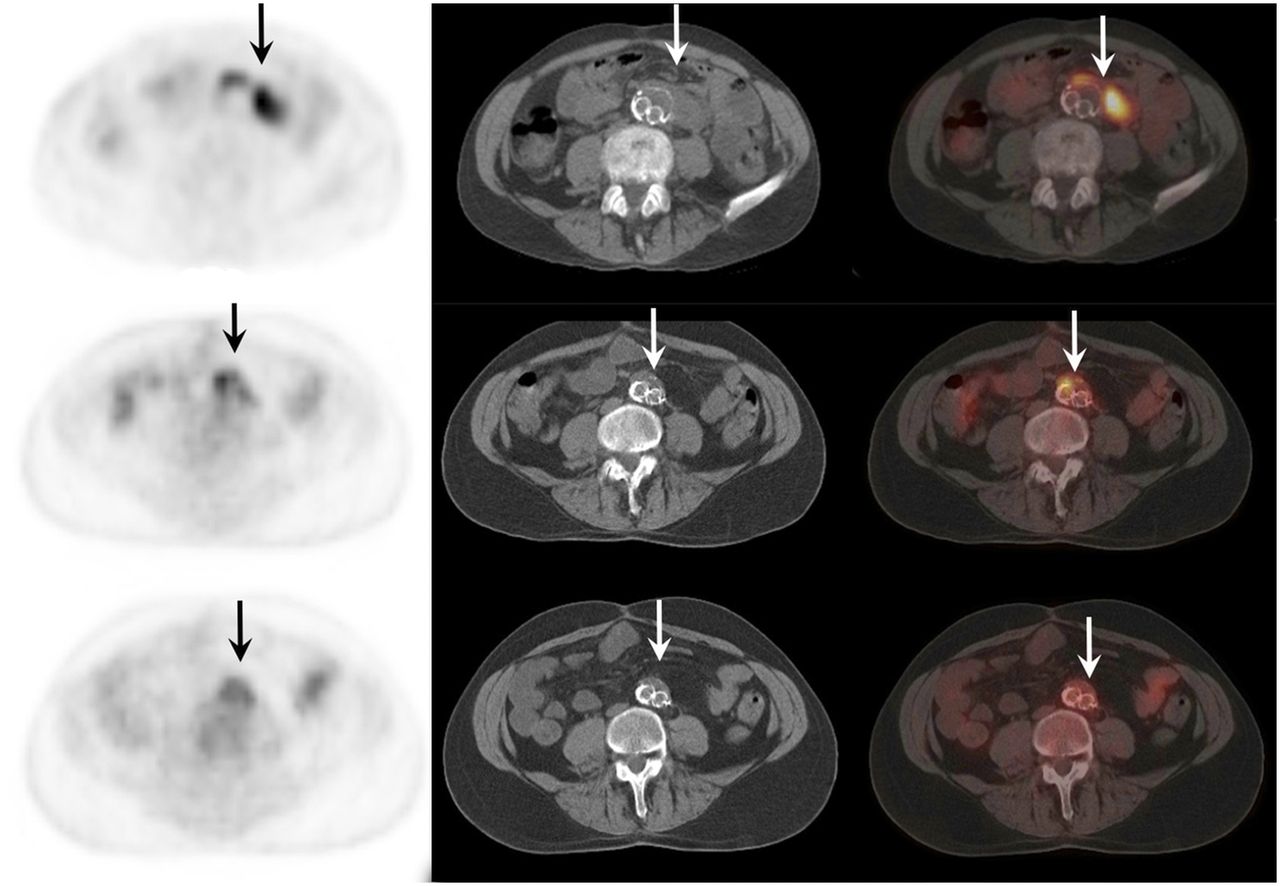
- FIGURE 3.
18F-FDG PET/CT scan of 64-y-old man with proven chronic Q fever, infected aneurysm, and infected vascular graft in aorta (arrows). Upper scan shows vascular infection before initiation of antibiotic treatment with doxycycline and hydroxychloroquine. Middle scan shows same area after 1 y of treatment. Lower scan, obtained 2 y after start of treatment, no longer shows vascular infection and therefore antibiotic treatment was discontinued. Four years later, patient died because of septic cholangitis. Autopsy did not show any Q fever foci, and PCR on several tissues, including aorta, was negative for C. burnetii.


Tables
Chronic Q fever Characteristics Proven Positive C. burnetii PCR in blood or tissue OR IFA phase I IgG of ≥1,024 for C. burnetii phase I IgG with either definite endocarditis according to modified Duke criteria or proven large-vessel or prosthetic infection by imaging techniques (18F-FDG PET/CT, MRI, CT, ultrasound) Probable IFA phase I IgG of ≥1,024 for C. burnetii phase I IgG AND valvulopathy not meeting modified Duke criteria OR known aneurysm or vascular or cardiac valve prosthesis without signs of infection by imaging techniques (TTE/TEE, 18F-FDG PET/CT, MRI, CT, ultrasound) OR suspected osteomyelitis, hepatitis, or pericarditis as manifestation of chronic Q fever OR pregnancy OR symptoms and signs of chronic infection such as fever, weight loss, night sweats, hepatosplenomegaly, and persistent ESR or CRP OR granulomatous tissue inflammation as proven by histologic examination OR immunocompromised state Possible IFA phase I IgG of ≥1,024 for C. burnetii phase I IgG without manifestations meeting criteria for proven or probable chronic Q fever IFA = immunofluorescence assay; TTE = transthoracic echocardiography; TEE = transesophageal echocardiography; ESR = erythrocyte sedimentation rate; CRP = C-reactive protein.
- TABLE 2
Interpretation of 18F-FDG PET/CT Combining Visual Grading Score and Uptake Pattern
Parameter Details Vascular infection Grade 1 18F-FDG uptake similar to background Grade 2* Low 18F-FDG uptake comparable to uptake by inactive muscles and fat, and above background uptake but below liver uptake Grade 3* Moderate 18F-FDG uptake clearly visible and higher than uptake by inactive muscles and fat, and similar to liver uptake Grade 4* Strong 18F-FDG uptake clearly above liver uptake Interpretation No vascular infection Grades 1 and 2 Inflammation Grades 3 and 4 and homogeneous uptake pattern without perigraft soft-tissue involvement Vascular infection Grades 3 and 4 and inhomogeneous uptake pattern with or without perigraft soft-tissue involvement Endocarditis Grade 1 No relevant 18F-FDG uptake of heart Grade 2† Diffuse 18F-FDG uptake in heart (reflecting normal uptake in myocardium) Grade 3 Focal 18F-FDG uptake in heart with or without diffuse low-level uptake in myocardium Interpretation No endocarditis Grade 1 Evaluation not possible Grade 2 Endocarditis Grade 3 - TABLE 3
Risk Factors and Outcome of All Patients with Proven, Probable, and Possible Chronic Q Fever
Parameter Proven Probable Possible Number of patients 147 60 66 Diagnostics Positive PCR blood + tissue 25 (17.0) 0 0 Positive PCR blood only 58 (39.5) 0 0 Positive PCR tissue only 27 (18.4) 0 0 Antiphase I IgG at diagnosis 4,096 (256–131,071) 4,096 (512–65,536) 2,048 (1,024–32,768) Vascular prosthesis 76 (51.7) 17 (28.3) 0 Infected vascular prosthesis 63 (82.9) 0 0 Known aneurysm 44 (29.9) 8 (13.3) 0 Infected aneurysm 34 (77.3) 0 0 Cardiac valve prosthesis 26 (17.7) 10 (16.7) 0 Modified Duke criteria Definite endocarditis 9 (6.1) 0 0 Possible endocarditis 37 (25.2) 19 (31.7) 3 (4.5) Rejected endocarditis* 77 (52.4) 37 (61.7) 55 (83.3) Other preexisting valvular disease 13 (8.9) 10 (16.7) 1 (1.5) Pacemaker 5 (3.4) 1 (1.7) 0 Intracardiac defibrillator 2 (1.4) 2 (3.3) 0 Other infection Other vascular infection 3 (2.0) 0 0 Other metastatic infection† 24 (16.3) 0 0 Mortality Q fever–related 18 (12.2) 1 (1.7) 0 Overall 33 (22.4) 8 (13.3) 8 (12.1) ↵* In 36 patients with chronic Q fever, no echocardiography was performed.
↵† Other metastatic foci were pulmonary foci (n = 4), cutaneous foci (n = 2), spinal infection (n = 3), psoas abscesses (n = 11), and both psoas abscess and spondylodiskitis (n = 4).
PTA = percutaneous transluminal angiography.
Qualitative data are expressed as numbers followed by percentages in parentheses; continuous data are expressed as mean followed by range in parentheses.
Reevaluation Finding n Q fever–related mortality No infection: grades 1 and 2 142 3 (2.1%) Inflammation: grades 3a and 4a without perigraft soft-tissue involvement 16 0 Infection: grades 3b and 4b with or without perigraft soft-tissue involvement 63 15 (23.8%) - TABLE 5
Comparison of 18F-FDG PET/CT to Modified Duke Criteria for Diagnosing Endocarditis
Diagnosis Modified Duke criteria Duke criteria including 18F-FDG PET/CT as major criterion Significance* Definite endocarditis 9 (3.8) 17 (7.2) 0.008 Possible endocarditis 59 (24.9) 57 (24.1) 0.063 Rejected endocarditis 169 (71.3) 163 (68.8) 0.008 Total 237† 237†





{kind=link}
{kind=link}
{kind=link}