


Abstract
377
Objectives: PET/MR has demonstrated significant influence in the characterization of pancreatic malignancies. This preliminary study aimed to prospectively evaluate TOF (Time-of-flight) PET/MR in the application of pancreatic cystic lesions.
Methods: Twenty-four patients with pancreatic cystic lesions were recruited in the study. After at least 6 hours of fasting, each patient underwent a torso non-TOF 18F-FDG PET/CT scan (Biograph 64, Siemens Healthcare) and subsequently a dedicated pancreas TOF PET/MR scan (SIGNA PET/MR, GE Healthcare). The MR sequences included RTr Cor SSFSE T2, RTr Ax fs T2 Propeller, RTr Ax DWI (b=0, 20, 50, 100, 200, 400, 600, 800 s/mm2), BH Ax LAVA-Flex and MRCP (magnetic resonance cholangiopancreatography). One experienced nuclear medicine physician assessed the PET/CT and PET images of PET/MR. One experienced radiologist analyzed the MR images. Neither interpreter was aware of the clinical history or histopathological results. On 18F-FDG PET scans, any focal tracer accumulation exceeding normal pancreas parenchyma uptake was considered positive. SUVmax and Standard ADCmean (mean apparent diffusion coefficient) of positive lesions were measured based on PET/MR images. LPR (lesion-to-pancreas ratio) was calculated comparing SUVmax of positive lesions with that of normal pancreas parenchyma and was set to one in patients without visible focal uptake. The image parameters were compared to histopathological results. Tumors with invasive carcinoma or poorly differentiated neuroendocrine tumors (G3) were considered as malignancy.
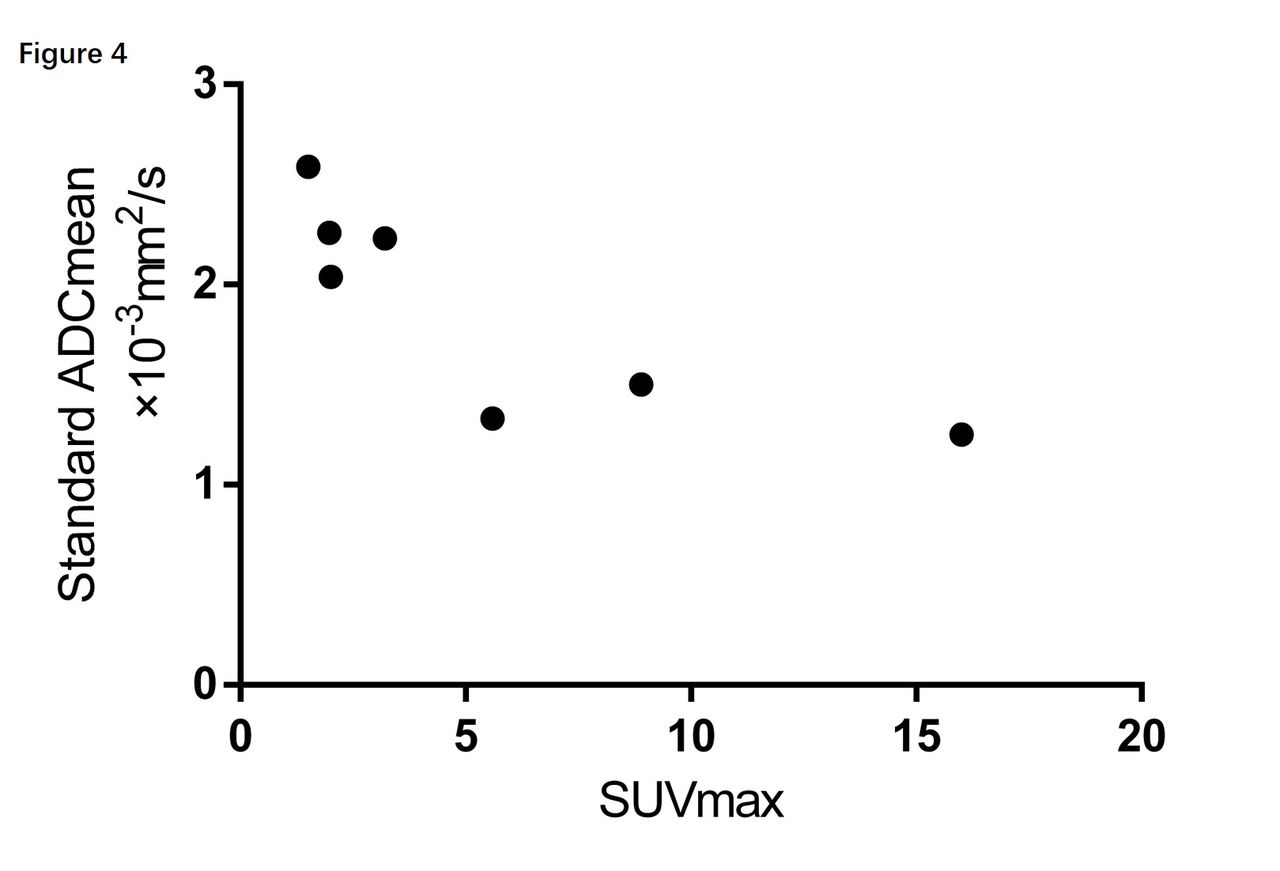
Results: Ten patients were ruled out since they were considered to have benign lesions and didn’t undergo surgery. Fourteen patients with histopathological confirmation remained in the study (Table 1). Based on 18F-FDG accumulation, six patients had positive PET scans. PET/MR revealed 3 more lesions than PET/CT on these patients (11 lesions vs. 8 lesions, respectively), which turned out to be the uptake of one mural nodule and two paraaortic lymph nodes (Figure 1,). Both PET/CT and PET/MR had good negative predictive value for benign lesions (Figure 2). In patients with intraductal papillary mucinous neoplasm, those with invasive carcinoma have a much higher LPR than those with dysplasia . A similar result was also shown in malignancies compared with benign lesions (Figure 3). Both SUVmax and LPR of positive lesions were correlated with Standard ADCmean (Figure 4). In one patient, both CT and MRI showed a large cyst with a mural nodule. But the uptake of the mural nodule was comparable to normal pancreas parenchyma. It turned out to be benign mucinous cystadenoma with intermediate dysplasia. T2-weighted images and MRCP were helpful in illustration of pancreatic duct dilation, intracystic septations, mural nodules, fluid heterogeneity, and connection to the main pancreatic duct. These anatomical features are critical in the differential diagnosis of pancreatic cystic lesions.
Conclusion: Both PET/CT and PET/MR do well in differentiating between benign and malignant pancreatic cystic lesions. However, TOF PET images could reveal more positive lesions than non-TOF images. Furthermore, PET/MR could provide more diagnostic anatomical information.





In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.