


Abstract
1211
Objectives: F-18 fluorodeoxy glucose (FDG) is mostly utilized to estimate tumor metabolism, myocardiac viability, and cerebral neuronal activity [1,2]. Then we occasionally find incidental prostatic FDG uptake (IPU) when interpreting FDG PET/CT results in various cancer work-up studies or healthcare screening. Although pure, malignant, hypermetabolic lesions related to prostate adenocarcinoma or metastases have been reported in a few studies [3,4], these situations do not occur frequently. Prostatitis is a common urologic disorder [5], and 10% of patients with chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) [6] have clinically significant bacteria in their prostate, including sexually-transmitted infectious microorganisms such as Chlamydia trachomatis [7,8]. Many men who have vague symptoms with CP/CPPS may not notice the disease and may not discuss their symptoms with clinicians. Therefore, clinically unexposed prostate infections are underestimated and are not exaggerated in clinical practice. To the best of our knowledge, although some reports have been researched to evaluate how IPU could be related to prostate cancer, it was difficult to find a paper about the relationship between IPU and prostate infection tests [9]. Therefore, a significant objective of this study is to evaluate the relationship between an IPU and factors of prostate infection.
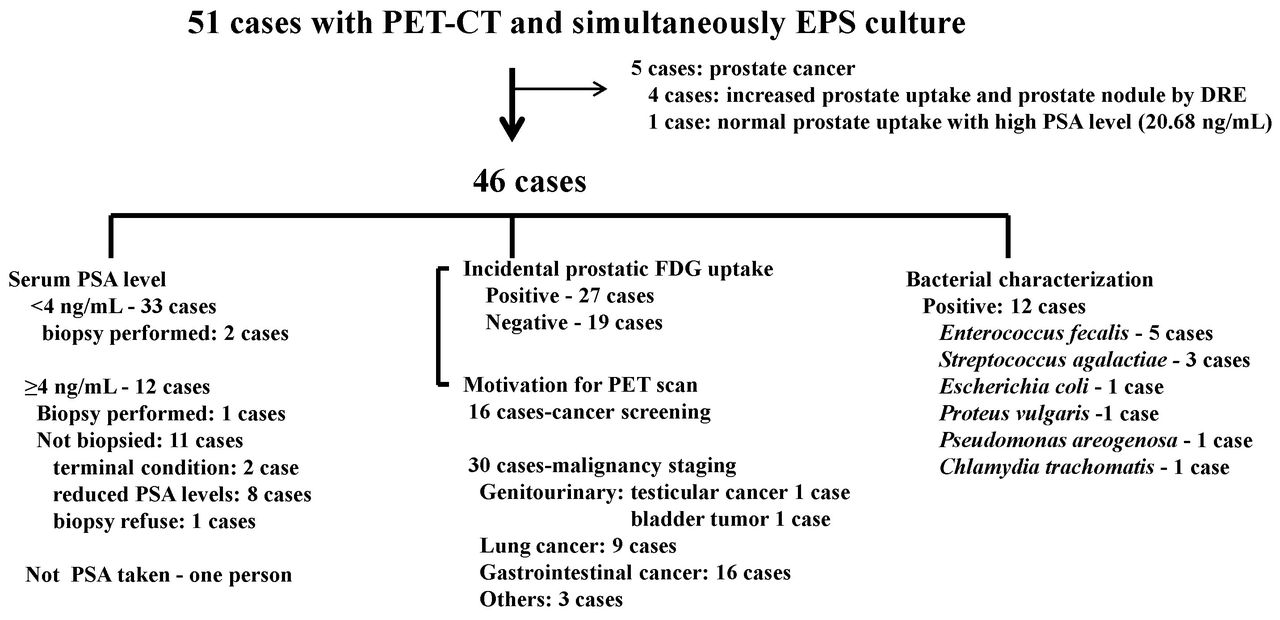
Methods: Only 51 men from 7,493 men who underwent FDG PET/CT scans over a period of six years agreed to a physical prostate examination and expressed prostatic secretion (EPS) test within two weeks after torso FDG PET/CT scans. Among them, five men were pathologically diagnosed with prostate cancer. We also reviewed the FDG PET/CT scans of the enrolled patients and evaluated the relationship between the FDG PET/CT, PSA and the prostatic laboratory findings. The FDG uptake patterns of the prostate glands were classified into diffuse and focal types according to a semiquantitive visual grade analysis. The precondition of a significantly positive focal and diffuse FDG uptake within the prostate gland was to ensure a distinct peripheral FDG uptake that was higher than the surrounding prostate gland and to reveal an even or uneven increase in the FDG uptake of the prostate tissue greater than that of the upper leg muscles.
Results: For the 46 men, 27 cases revealed an IPU in FDG PET/CT while 19 did not. Of the 46 subjects that did not reveal any prostate nodule in their prostate with DRE, 33 men showed normal PSA values (< 4 ng/mL) while 12 men exhibited high serum PSA levels (蠅 4 ng/mL) during their initial visit (Fig. left). The enrolled patient characteristics were as follows: mean age of 61.15 ± 13.79 yrs (30-83 yrs), SUVmax of 2.64 ± 1.33 (1.2 - 7.1), and PSA of 3.10 ± 3.50 (range: 0.16-13.55 ng/mL). There was a significant difference in the serum PSA level (p=0.018) between the negative and positive FDG PET/CT groups, and we could not find any significant differences in age, WBC counts in EPS, presence of pyuria, combined malignancies, and presence of FDG uptake. Ten of 27 patients (37%) with IPU in the PET/CT scan revealed bacterial infections in their prostate (Fig. right). A multivariate analysis revealed that the bacterial presence in EPS increased the risk of IPU (adjusted odds ratio [OR], 9.167; P = 0.019) (Table).
Conclusion: The results of our study demonstrate that there is a significant association between IPU and the positive results for a prostate culture. In addition, there is a significant difference in the PSA between patients with negative and positive results in the FDG PET/CT scans. Bacterial presence in the prostate tends to increase the risk of an IPU on FDG PET/CT. Therefore, men with incidental prostate FDG uptake should be considered for the possibility of a prostate infection in addition to a concomitant malignancy. Research Support:

Influence of patient characteristics on FDG PET/CT scan positivity
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.