


Article Figures & Data
Figures
- FIGURE 1.
Kaplan–Meier curve in reference to MACE stratified by MBR-IR value y-axis represents cumulative event-free rate (log-rank test, P < 0.001).
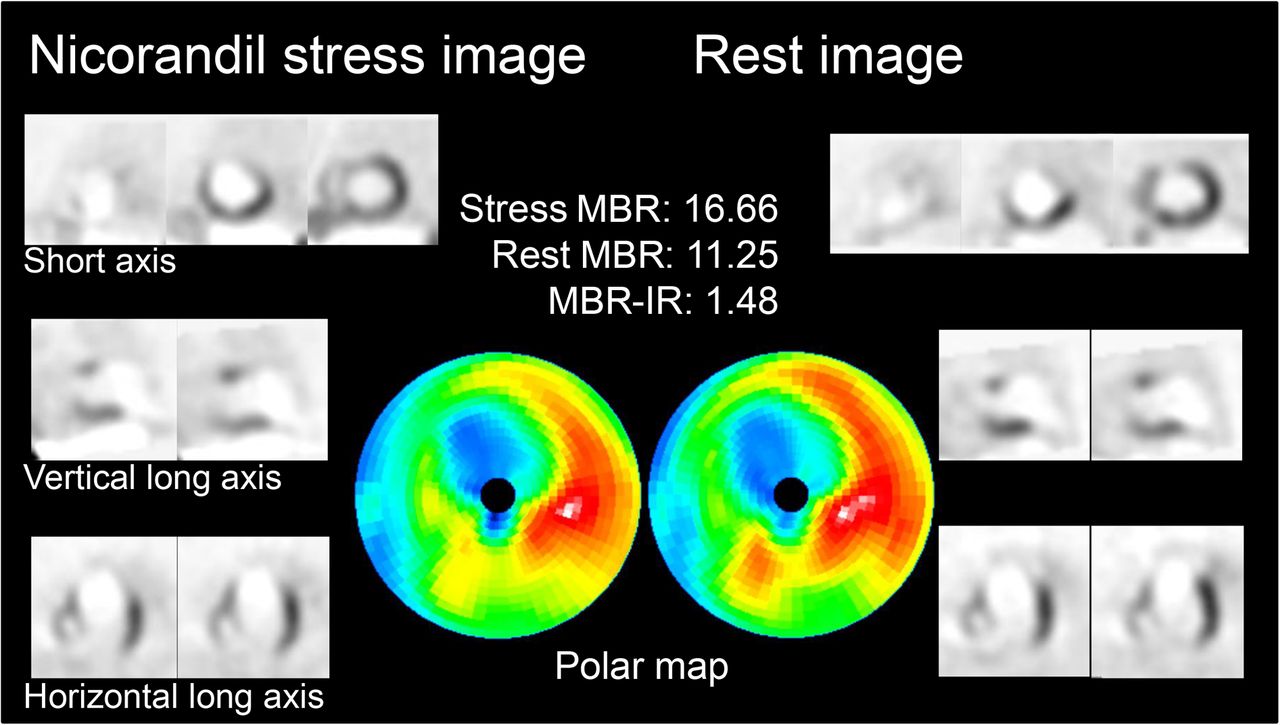
- FIGURE 2.
A 77-y-old man with acute ischemic heart failure in high–MBR-IR group. Rest myocardial perfusion SPECT images show anteroseptal–apical and distal inferior perfusion defects, and perfusion improvement is observed for anteroseptal wall in nicorandil-stress images, excluding central area of previous myocardial infarction site. MBR-IR is relatively high for an AIHF patient, with a value of 1.48. This patient remained MACE-free for entire 5-y follow-up period.
- FIGURE 3.
A 69-y-old woman with acute ischemic heart failure in low–MBR-IR group. Nicorandil stress and rest myocardial perfusion SPECT images show anteroseptal–apical perfusion defects, and perfusion improvement is observed only in marginal zone of previous myocardial infarction site in nicorandil-stress images. MBR-IR is low, with a value of 1.09. This patient was hospitalized due to deterioration of heart failure 189 d after initial onset.



Tables
Characteristic n or mean ± SD No. of patients 22 Age (y) 70 ± 12 Male 16 (73%) NYHA class (I/II/III/IV) 0/2/2/18 BNP (pg/mL) 524 (258–744) Coronary risk factors Hypertension 21 (95%) Dyslipidemia 15 (68%) Diabetes mellitus 13 (59%) Interval (d) Onset to first MPI 8 (6–12) Nicorandil-stress and rest 3 (3–5) Onset to CAG 7 (4–15) Previous MI 20 (91%) 1VD/2VD/3VD 2/7/13 NYHA = New York Heart Association; BNP = brain natriuretic peptide; MPI = myocardial perfusion imaging; MI = myocardial infarction; VD = vessel disease.
Categorical data are expressed as numbers, followed by percentages in parentheses, unless otherwise indicated; continuous data are expressed as mean ± SD or median (25th–75th).
Cardiovascular parameter Nicorandil-stress Rest P Systolic BP (mm Hg) 98 ± 16 123 ± 15 <0.001 Diastolic BP (mm Hg) 60 ± 6 70 ± 15 0.004 Heart rate (bpm) 78 ± 15 67 ± 11 <0.001 LVEF (%) 40 (31–44) 36 (30–40) 0.106 LVEDV (mL) 154 (118–191) 161 (105–196) 0.516 LVESV (mL) 96 (71–128) 108 (63–131) 0.276 BP = blood pressure.
Data are expressed as mean ± SD or median (25th–75th).
Characteristic High MBR-IR (n = 11 [50%]) Low MBR-IR (n = 11 [50%]) P Age (y) 75 ± 9 65 ± 13 0.046 Male 7 (64%) 9 (82%) 0.635 NYHA class 0/0/2/9 0/2/0/9 0.883 BNP (pg/mL) 534 (189–965) 513 (412–704) 0.844 Hypertension 10 (91%) 11 (100%) 1.000 Dyslipidemia 6 (55%) 9 (82%) 0.361 Diabetes mellitus 5 (45%) 8 (73%) 0.387 Previous myocardial infarction 10 (91%) 10 (91%) 1.000 SSS 17 (15–24) 25 (23–28) 0.139 SRS 19 (16–28) 27 (24–29) 0.144 Rest LVEF (%) 38 (32–53) 31 (30–38) 0.216 Rest LVEDV (mL) 136 (90–165) 186 (156–201) 0.111 Rest LVESV (mL) 83 (43–116) 118 (103–140) 0.102 Nicorandil-stress MBR 29.49 (26.57–37.44) 26.70 (16.96–31.93) 0.151 Rest MBR 18.62 (16.62–26.80) 25.39 (16.17–30.71) 0.507 MBR-IR 1.55 (1.34–1.61) 1.08 (1.02–1.10) <0.001 MBR-IR in infarcted region 1.06 (1.00–1.06) 0.98 (0.97–1.00) 0.149 MBR-IR in ischemic region 1.57 (1.41–1.74) 1.18 (1.16–1.22) 0.002 NYHA = New York Heart Association; BNP = brain natriuretic peptide; SSS = summed stress score; SRS = summed rest score.
Categorical data are expressed as counts (%), and continuous data are expressed as mean ± SD or median (25th–75th).
- TABLE 4
Comparison of Clinical Profiles of All Patients Who Did and Did Not Experience MACE
Characteristic MACE (n = 12 [55%]) No MACE (n = 10 [45%]) P Age (y) 70 ± 10 71 ± 14 0.950 Male 9 (75%) 7 (70%) 1.000 NYHA class 0/0/1/11 0/2/1/7 0.185 BNP (pg/mL) 664 (420–794) 408 (184–687) 0.277 Hypertension 12 (100%) 9 (90%) 0.455 Dyslipidemia 9 (75%) 6 (60%) 0.652 Diabetes mellitus 7 (58%) 6 (60%) 1.000 Previous myocardial infarction 12 (100%) 8 (80%) 0.195 SSS 25 (21–28) 20 (15–25) 0.209 SRS 27 (23–29) 22 (15–29) 0.427 Low MBR-IR 10 (83%) 1 (10%) 0.002 Rest LVEF (%) 31(30–39) 38 (31–53) 0.477 Treatments after myocardial perfusion imaging PCI 3 (25%) 1 (10%) 0.594 CABG 1 (8%) 1 (10%) 1.000 Nicorandil 7 (58%) 5 (50%) 1.000 ARB 11 (92%) 6 (60%) 0.135 β-blocker 10 (83%) 9 (90%) 1.000 Statin 10 (83%) 6 (60%) 0.348 Pacemaker implantation 2 (17%) 0 (0%) 0.481 ICD implantation 1 (8%) 0 (0%) 1.000 NYHA = New York Heart Association; BNP = brain natriuretic peptide; SSS = summed stress score; SRS = summed rest score; PCI = percutaneous coronary intervention; CABG = coronary artery bypass grafting; ARB = angiotensin receptor blocker; ICD = implantable cardioverter-defibrillator.
Categorical data are expressed as counts (%), and continuous data are expressed as mean ± SD or median (25th–75th).
Univariate Multivariate Characteristic Hazard ratio 95% confidence interval P Hazard ratio 95% confidence interval P Age 0.999 0.967–1.032 0.945 NYHA class IV 1.589 0.536–4.312 0.404 BNP 1.000 0.999–1.001 0.160 1.001 0.999–1.002 0.086 Hypertension 1.833 0.246–13.677 0.554 Dyslipidemia 1.259 0.512–3.097 0.615 Diabetes mellitus 0.947 0.404–2.220 0.901 Previous myocardial infarction 1.920 0.446–8.261 0.381 SSS 1.009 0.966–1.055 0.683 SRS 1.003 0.964–1.044 0.866 Low MBR-IR 3.640 1.456–9.103 0.006 3.913 1.552–9.868 0.004 Rest LVEF 0.992 0.964–1.020 0.576 Treatment after MPI PCI 1.601 0.538–4.761 0.398 CABG 0.771 0.179–3.309 0.726 Nicorandil 1.091 0.471–2.529 0.839 ARB 1.639 0.598–4.495 0.337 β-blocker 1.013 0.298–3.451 0.983 Statin 1.359 0.528–3.501 0.525 NYHA = New York Heart Association; BNP = brain natriuretic peptide; SSS = summed stress score; SRS = summed rest score; MPI = myocardial perfusion imaging; PCI = percutaneous coronary intervention; CABG = coronary artery bypass grafting; ARB = angiotensin receptor blocker; ICD = implantable cardioverter-defibrillator.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.