


Article Figures & Data
Figures
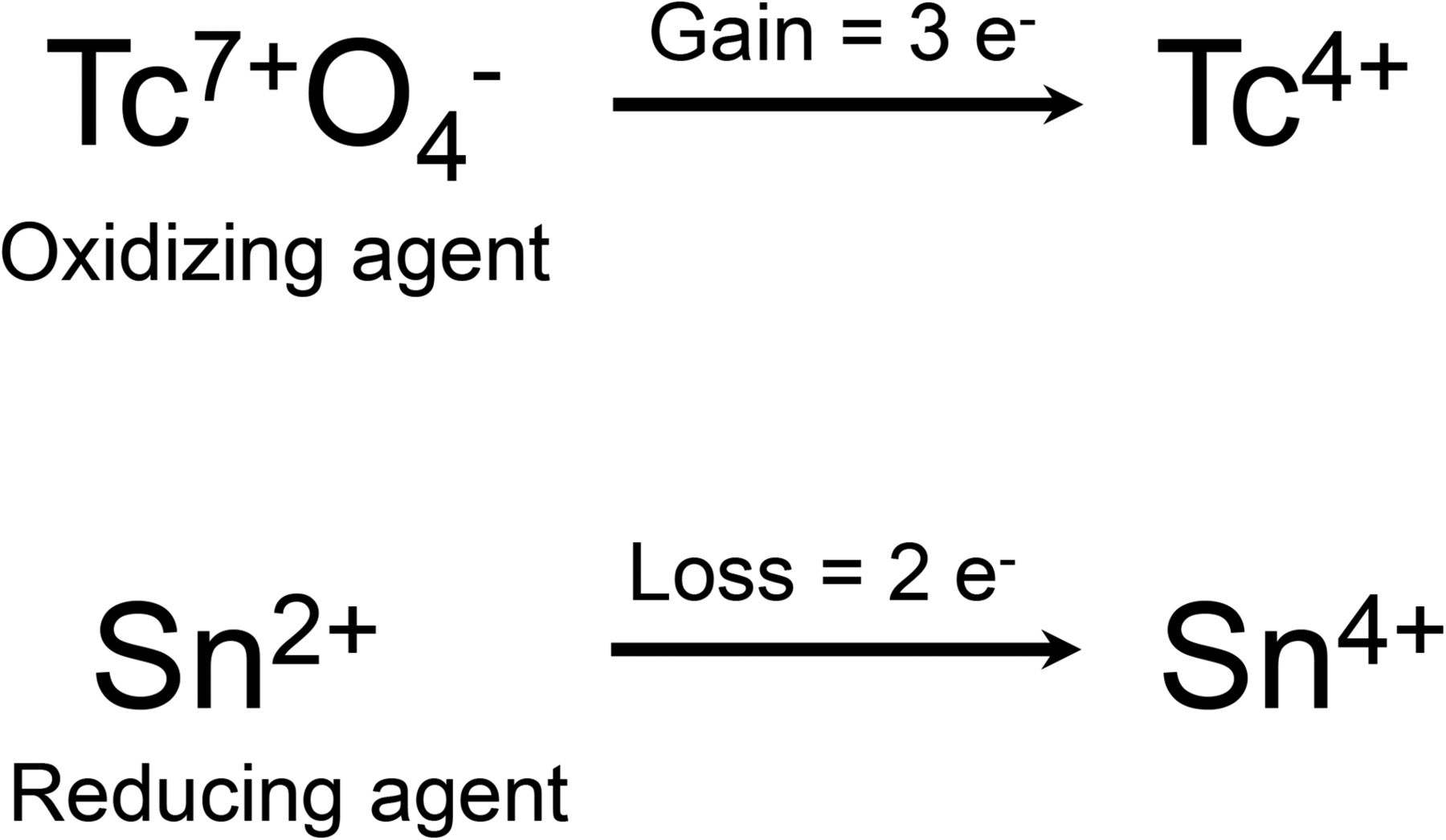
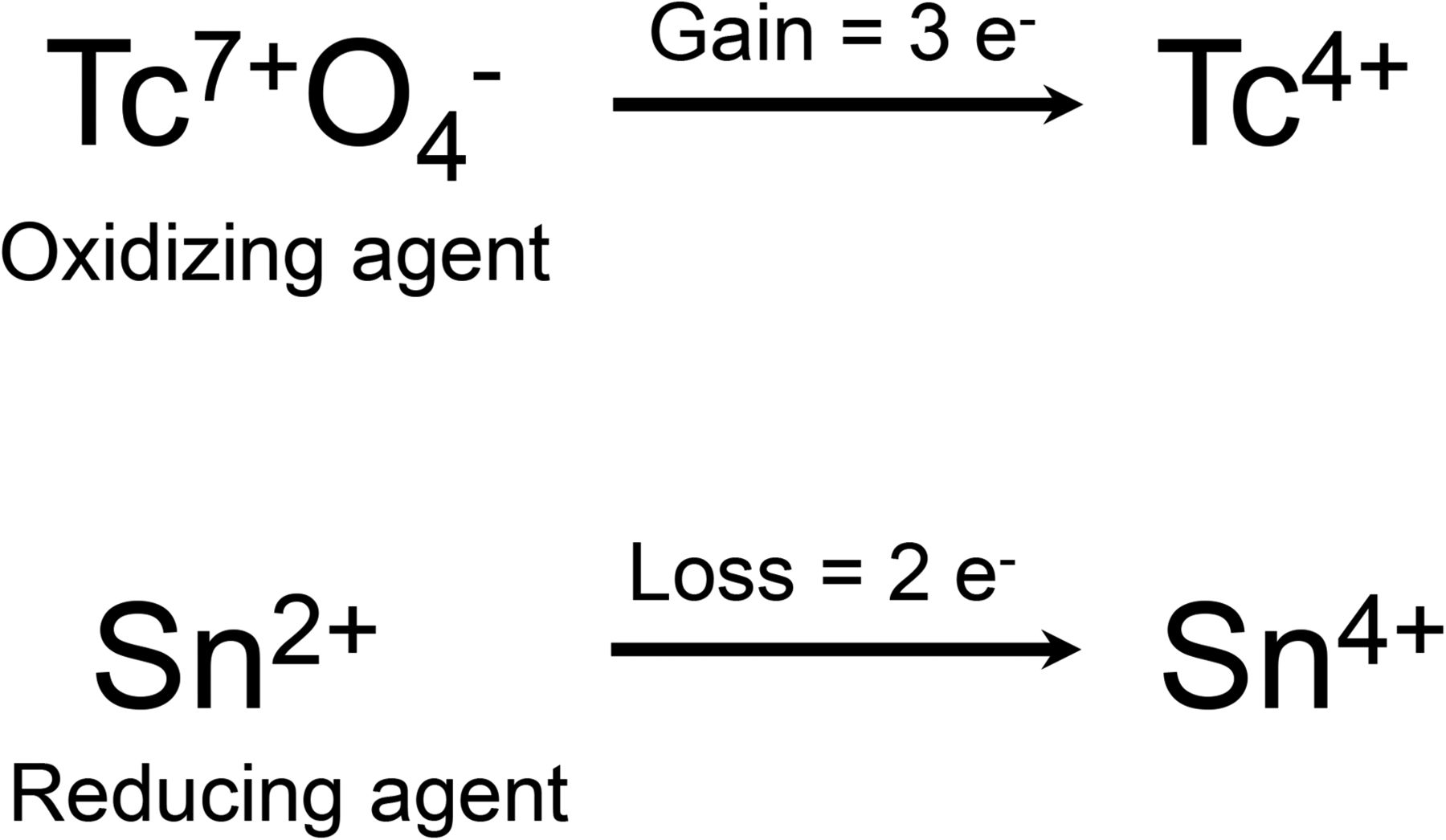
- FIGURE 1.
Stannous reduction method (3).
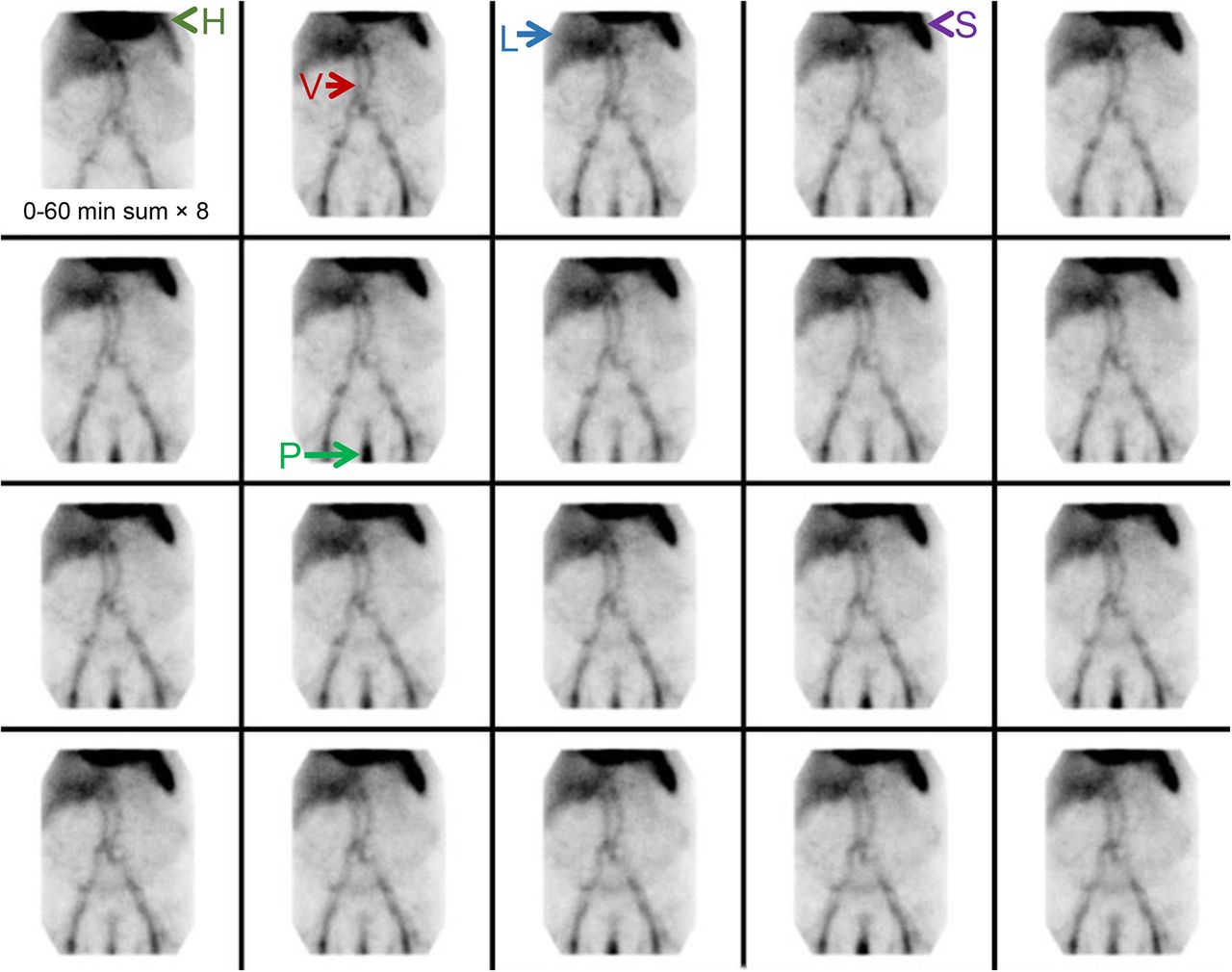
- FIGURE 2.
Normal biodistribution of 99mTc-labeled erythrocytes. Heart (H), vascular structures (V), liver (L), spleen (S), and penis (P) are labeled. We see no intraluminal activity to suggest presence of active gastrointestinal bleed.
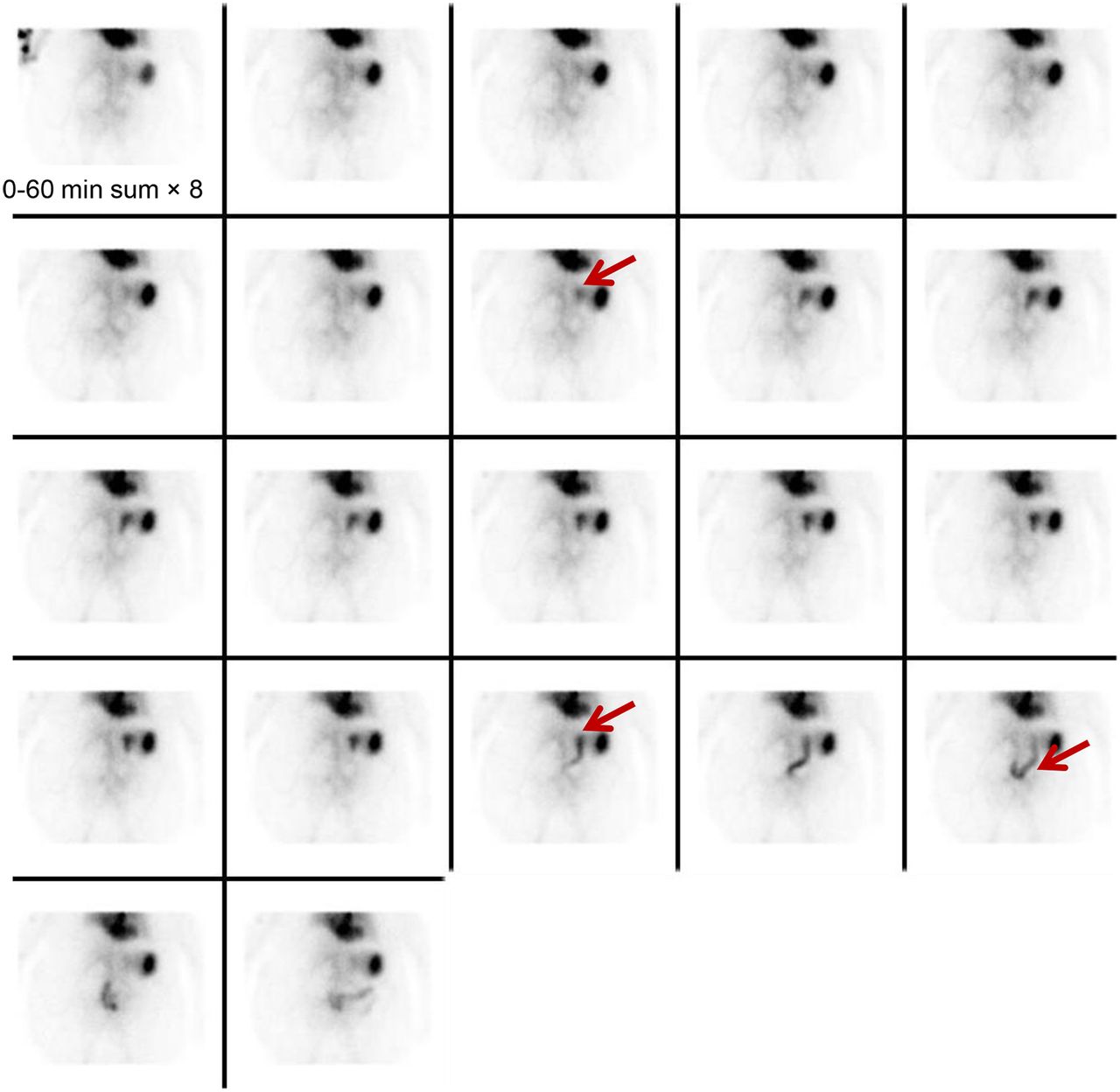
- FIGURE 3.
Example of bleeding originating from branch of celiac artery. Focus of increasing intensity is identified in upper abdomen, moves in anterograde fashion, and conforms to bowel. Distribution of focus is suggestive of gastric bleed (arrows).
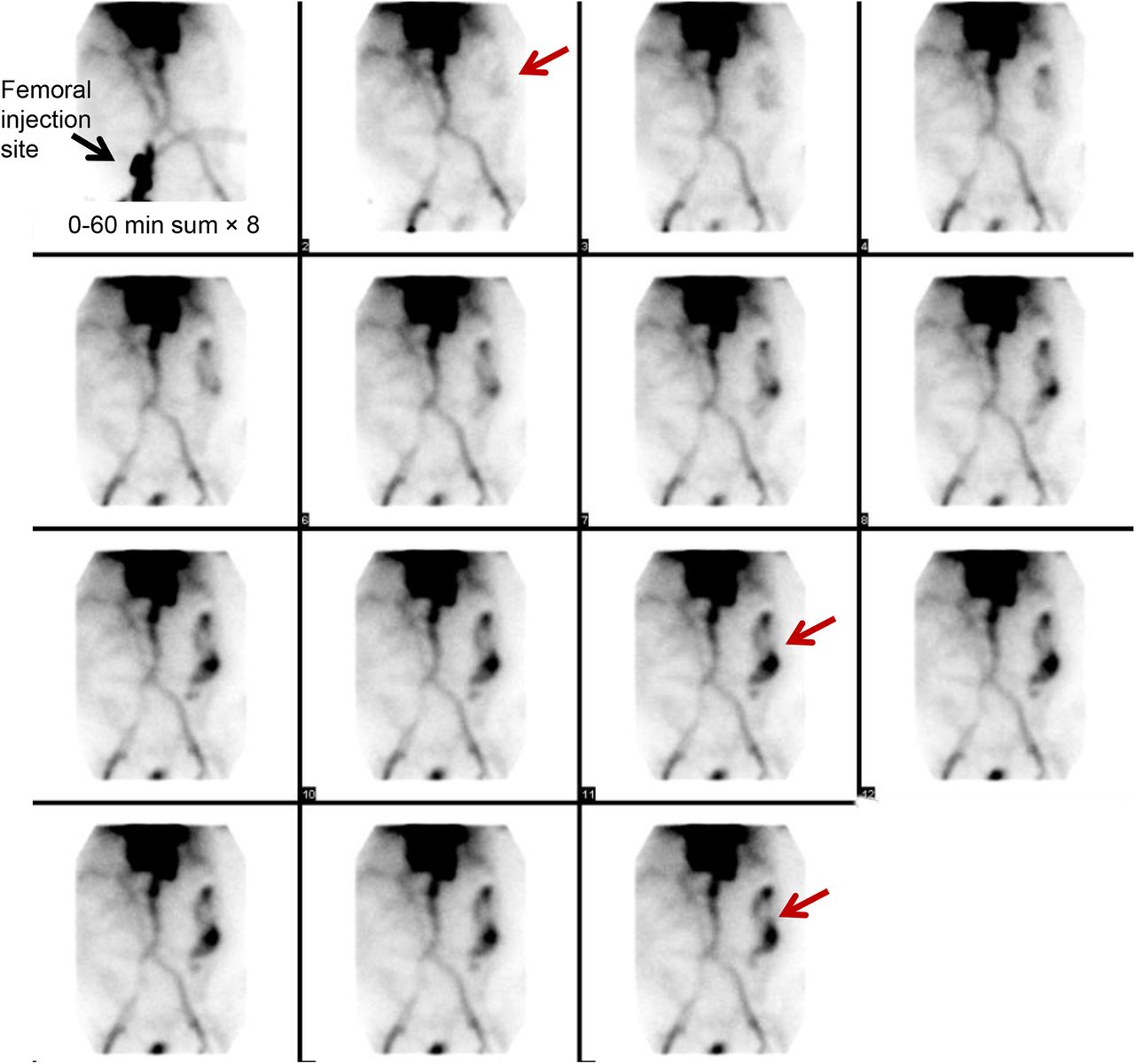
- FIGURE 4.
Example of bleeding originating from branch of superior mesenteric artery. Focus of increasing intensity is identified in lower abdomen at midline (arrows) and shows anterograde and retrograde movement conforming to bowel lumen. Focus crosses midline several times and thus is most compatible with small-bowel bleed.
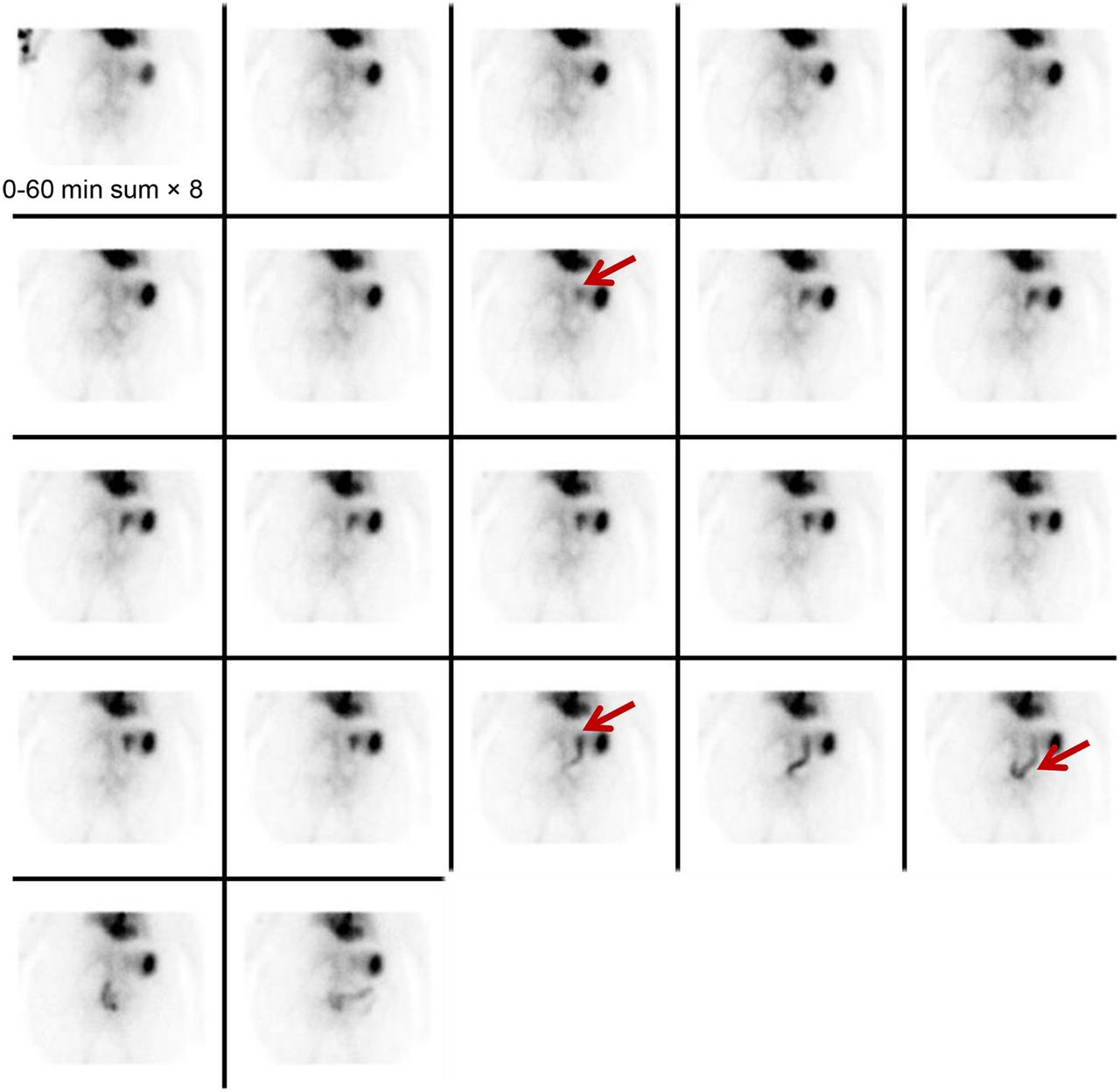
- FIGURE 5.
Example of bleeding originating from branch of inferior mesenteric artery. Focus of increasing intensity is identified in left upper quadrant and shows anterograde movement. Given its distribution in periphery of abdomen (arrows), focus is typical of large-bowel bleed originating in descending colon.


Tables
Term Definition Overt or acute gastrointestinal bleeding Visible bleeding in the form of hematemesis, melena, or hematochezia Occult or chronic gastrointestinal bleeding Bleeding not apparent to patient and presenting as anemia or on fecal occult blood testing Obscure gastrointestinal bleeding Recurrent bleeding of uncertain source after or despite upper or lower endoscopy Hematemesis Vomiting of blood Melena Dark, tarry/sticky feces containing partially digested blood Hematochezia Passage of fresh blood per anus, usually in or within stools - TABLE 2
Causes of Interference with Erythrocyte Radiolabeling, Leading to Free 99mTc-Pertechnetate (9–15)
Cause Mechanism of disrupted radiolabeling Methyldopa Oxidation of stannous ion; decrease in reduction Hydralazine Oxidation of stannous ion; decrease in reduction Quinine Possible antibody to red blood cells Doxorubicin Lowered labeling efficiency in proportion to concentration of drug Iodinated contrast medium Decrease in stannous reduction; alteration of 99mTc binding Chocolate Unknown Tobacco Oxidation of stannous ion, possible damage to red blood cell plasma membrane or possible chelating action on stannous or pertechnetate ions (mechanism relates to reactive oxygen species present) Heparin Formation of complexes with 99mTc-pertechnetate in presence of stannous ion, causing renal excretion Too much or too little stannous ion Alteration of 99mTc-pertechnetate reduction Recent blood transfusion Unknown Sickled red blood cells Impaired labeling due to abnormal hemoglobin structure Method Description and considerations Efficiency In vivo Patient is injected intravenously with 1 mg of stannous pyrophosphate, which circulates for 20 min, followed by intravenous injection of 555–1,110 MBq of 99mTc-pertechnetate. This technique is generally not recommended because of its low labeling efficiency but is reserved for patients who will not receive blood products for religious reasons. 75%–80% Modified in vivo Patient is injected intravenously with 1 mg of stannous pyrophosphate, which circulates for 20 min. Vial of blood is mixed with 555–1,110 MBq of 99mTc-pertechnetate and allowed to incubate for 10 min before intravenous injection into patient. 85%–90% In vitro Vial of blood is withdrawn from patient and added to vial containing stannous pyrophosphate. After 5 min, vial A containing sodium hypochlorite is added to destroy extracellular Sn2+. Vial B containing citrate buffer is then added. 99mTc-pertechnetate (555–1,110 MBq) is added and incubated before intravenous administration to patient. ≥97% - TABLE 4
Comparison of Whole-Body Absorbed Radiation Dose Evaluated by GIBS vs. CTA (56,72)
Technique Dose (mSv) Pediatric GIBS with 80–784 MBq of 99mTc-labeled red blood cells 0.559–5.488 Adult GIBS with 555–1,110 MBq of 99mTc-labeled red blood cells 3.885–7.77 CTA protocoled for gastrointestinal bleeding without initial unenhanced CT phase 18.2–28* CTA protocoled for gastrointestinal bleeding with initial unenhanced CT phase 26.8–42* ↵* Iterative reconstruction CT will be lower.
Pharmaceutical Dosing/timing Effect Cimetidine (other H2 blockers, such as famotidine, ranitidine, or proton pump inhibitors, can also be used but have different dosing) 20 mg/kg/d orally for 2 d in children or 10–20 mg/kg/d for 2 d in neonates Inhibits release of 99mTc-pertechnetate by intraluminal cells, thus increasing and prolonging uptake Glucagon 50 μg/kg intravenously 10 min after administration of 99mTc-pertechnetate Slightly reduces gastric activity of 99mTc-pertechnetate and suppresses peristaltic activity Pentagastrin (no longer recommended in United States secondary to side effects) 6 μg/kg subcutaneously 20–30 min before 99mTc-pertechnetate administration Increases gastric mucosal uptake of 99mTc-pertechnetate, thus increasing target-to-background ratio Related to gastrointestinal tract Not related to gastrointestinal tract Peptic ulcer Hydronephrosis Barrett esophagus Aneurysm of abdominal vessel Retained gastric antrum Calyceal diverticulum Duplication cyst of ileum Anterior sacral meningomyelocele Small-bowel obstruction Hemangioma Appendicitis Lymphoma Intussusception Ectopic kidney Inflammatory bowel diseases (e.g., Crohn disease or ulcerative colitis) Recent laparoscopic surgery (hyperemia at periumbilical port site) Carcinoid of small bowel Volvulus Small-bowel bleeding not related to Meckel diverticulum





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}