


Abstract
The critical challenge in abdominal aortic aneurysm (AAA) research is the accurate diagnosis and assessment of AAA progression. Angiogenesis is a pathologic hallmark of AAA, and CD105 is highly expressed on newly formed vessels. Our goal was to use 64Cu-labeled anti-CD105 antibody Fab fragment for noninvasive assessment of angiogenesis in the aortic wall in a murine model of AAA. Methods: Fab fragment of TRC105, a mAb that specifically binds to CD105, was generated by enzymatic papain digestion and conjugated to NOTA (1,4,7-triazacyclononane-1,4,7-triacetic acid) for 64Cu labeling. The binding affinity/specificity of NOTA-TRC105-Fab was evaluated by flow cytometry and various ex vivo studies. BALB/c mice were anesthetized and treated with calcium phosphate to induce AAA and underwent weekly PET scans using 64Cu-NOTA-TRC105-Fab. Biodistribution and autoradiography studies were also performed to confirm the accuracy of PET results. Results: NOTA-TRC105-Fab exhibited high purity and specifically bound to CD105 in vitro. Uptake of 64Cu-NOTA-TRC105-Fab increased from a control level of 3.4 ± 0.1 to 9.5 ± 0.4 percentage injected dose per gram (%ID/g) at 6 h after injection on day 5 and decreased to 7.2 ± 1.4 %ID/g on day 12, which correlated well with biodistribution and autoradiography studies (i.e., much higher tracer uptake in AAA than normal aorta). Of note, enhanced AAA contrast was achieved, due to the minimal background in the abdominal area of mice. Degradation of elastic fibers and highly expressed CD105 were observed in ex vivo studies. Conclusion: 64Cu-NOTA-TRC105-Fab cleared rapidly through the kidneys, which enabled noninvasive PET imaging of the aorta with enhanced contrast and showed increased angiogenesis (CD105 expression) during AAA. 64Cu-NOTA-TRC105-Fab PET may potentially be used for future diagnosis and prognosis of AAA.
- abdominal aortic aneurysm (AAA)
- positron emission tomography (PET)
- antibody fragment
- Fab
- CD105 (endoglin)
Abdominal aortic aneurysm (AAA) is a common and potentially lethal vascular disease more prevalent in men over the age of 65. It is characterized by progressive expansion and weakening of the abdominal aortic wall (1–3). Advanced AAA usually leads to rupture, which represents a leading cause of death in the Western world. In the United States, there are approximately 30,000 deaths every year because of AAA, and 15,000 of these are related to rupture of AAA (3,4). Although the techniques for effective diagnosis and treatment of AAA are urgently needed, noninvasive imaging of AAA at the molecular/cellular level is still underexplored, which has attracted tremendous interest from the research community. Several tracers, for example, 18F-FDG (5–10), have been reported for PET imaging of AAA in previous studies. However, the reliability of conventional tracers is still under debate (11), and there is need for new and more reliable molecular targets and tracers for PET imaging of AAA.
Angiogenesis has been proven to be a pathologic hallmark of AAA in both human and animal models, and it plays an important role in the development and progression of AAA (12–15). Higher levels of neovascularization are detected at the rupture edge in aortic aneurysm, suggesting that imaging of molecules and processes involved in angiogenesis can potentially depict high-risk aneurysms (16). One important advantage of targeting angiogenesis is that rapid, persistent, and specific targeting can be achieved with different probes, which endows an excellent efficiency and imaging contrast. The endothelial cells of newly formed vessels express high levels of CD105, also known as endoglin, on their surfaces (17). We have previously demonstrated the efficacy of a CD105-targeted antibody, TRC105, for in vivo imaging of angiogenesis (18–21). Therefore, we hypothesized that CD105 could act as a promising target for imaging and even for treatment of AAA.
Our goal was to investigate a novel probe for effective targeting and imaging of AAA with excellent targeting specificity and imaging contrast. To achieve this goal, we used a 64Cu-labeled TRC105 Fab fragment (i.e., 64Cu-NOTA-TRC105-Fab; NOTA is 1,4,7-triazacyclononane-1,4,7-triacetic acid) as a probe for PET imaging of AAA. Compared with TRC105 full antibody, TRC105-Fab could be rapidly cleared by the kidneys with shortened circulation half-life (22), possibly resulting in superior imaging contrast in the abdominal area. To the best of our knowledge, this is the first report of AAA PET imaging with an antibody fragment–based probe.
MATERIALS AND METHODS
Chemicals
TRC105 was provided by TRACON Pharmaceuticals, Inc. Rat antimouse CD31 primary antibody was purchased from BD Biosciences. AlexaFluor488- and Cy3-labeled secondary antibodies were purchased from Jackson Immunoresearch Laboratories, Inc. S-2-(4-isothiocyanatobenzyl)-1,4,7-triazacyclononane-1,4,7-triacetic acid (p-SCN-Bn-NOTA) was purchased from Macrocyclics, Inc. Fluorescein isothiocyanate (FITC) and chelex 100 resin (50–100 mesh) were acquired from Sigma-Aldrich. PD-10 desalting columns were purchased from GE Healthcare. All other reaction buffers and chemicals were from Thermo Fisher Scientific.
Generation, Characterization, and NOTA/FITC Conjugation of TRC105-Fab
TRC105-Fab was obtained by digestion of TRC105 antibody (5 mg/mL) using immobilized papain (weight ratio, papain to TRC105 = 1:40) in a reaction buffer (10 mM disodium ethylenediaminetetraacetic acid, 20 mM sodium phosphate dibasic, and 80 mM l-cysteine hydrochloride) for 4 h at 37°C under constant stirring (22,23). Subsequently, the supernatant was collected and purified by a Sephadex G-75 size-exclusion column (GE Healthcare Life Sciences) (fractionation range, 3,000–80,000 Da) using phosphate-buffered saline (PBS) as the mobile phase. The elution from the Sephadex G-75 size-exclusion column was tested by ultraviolet absorbance at 280 nm. The purity of TRC105-Fab was evaluated by sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS-PAGE; 5% stacking gel and 8% resolving gel) (24).
As-prepared TRC105-Fab was conjugated with p-SCN-Bn-NOTA or FITC at a molar ratio of 1:10 at pH 9.0 for 2 h (22). The final products (NOTA-TRC105-Fab or FITC-TRC105-Fab) were purified by PD-10 size-exclusion columns using PBS as the mobile phase to remove unbound NOTA/FITC.
Cell Lines and Flow Cytometry
Human umbilical vein endothelial cells (HUVECs) were obtained from the American Type Culture Collection and cultured as previously described (25–27). When the cells reached approximately 80% confluence, they were harvested and suspended in cold PBS with 2% bovine serum albumin at a concentration of 5 × 106 cells/mL, incubated with FITC-TRC105-Fab or FITC-TRC105-Fab-NOTA for 30 min at room temperature, and washed 3 times with cold PBS. Subsequently, the cells were analyzed using a BD FACSCalibur 4-color analysis cytometer equipped with 488- and 633-nm lasers (Becton-Dickinson) and FlowJo analysis software (Tree Star, Inc.).
AAA Animal Models
AAA was induced by topical application of calcium phosphate in 4- to 5-wk-old female BALB/c mice (Harlan) under anesthesia (2%–4% isoflurane) as described previously (28). Briefly, the abdominal cavity was opened with a midline abdominal incision. The infrarenal region of the abdominal aorta was freed from the surrounding adipofascial tissue by gentle dissection, and a small piece of 0.5 mol/L CaCl2-soaked gauze was applied for 10 min to the aorta followed by application of another piece of PBS-soaked gauze for 5 min. Mice in the sham group were treated only with PBS for 15 min. All animal studies were conducted under a protocol approved by the University of Wisconsin Institutional Animal Care and Use Committee.
Radiolabeling, PET Imaging, and Biodistribution Studies of NOTA-TRC105-Fab
64Cu was produced by a PETrace cyclotron (GE Healthcare) using the 64Ni(p,n)64Cu reaction. 64Cu was diluted in 300 μL of 0.1 M sodium acetate buffer (pH 5.0) and mixed with 200 μL of NOTA-TRC105-Fab (0.4 mg/mL). The reaction was performed at 37°C for 45 min with constant shaking. The resulting 64Cu-NOTA-TRC105-Fab was purified by PD-10 size-exclusion column chromatography, using PBS as the mobile phase. The radioactive fraction containing 64Cu-NOTA-TRC105-Fab was collected for further in vitro and in vivo studies.
PET imaging was performed on days 5 and 12 after the induction of AAA using a micro-PET/micro-CT Inveon rodent model scanner (Siemens Medical Solutions USA, Inc.). The animals were injected with 5–10 MBq of 64Cu-NOTA-TRC105-Fab via the tail vein, and serial images were obtained at 0.5, 3, 6, 14, and 24 h after injection. Data acquisition, image reconstruction, and region-of-interest (ROI) analysis of the PET images were performed as previously described (22,29). After the last scan at 24 h after injection on day 12, biodistribution studies were performed to corroborate PET data. Aorta, blood, and major organs/tissues were collected and wet-weighed. The radioactivity in the tissue was measured using a γ counter (PerkinElmer) and presented as percentage injected dose per gram (%ID/g) (mean ± SD).
Ex Vivo Imaging and Histology
The infrarenal portion of the abdominal aorta was collected from the animals after euthanasia. Autoradiographic images of the collected aortas were obtained using a γ camera. The aortas were frozen and cryosectioned for histologic analysis. Hematoxylin and eosin staining was performed to observe the microscopic changes in the abdominal aortic wall, acquired by a Nikon Eclipse Ti microscope (18). Frozen tissue slices of 7-μm thickness were double-stained for endothelial marker CD31 and CD105 as previously reported (20). The slides were coverslipped with Vectashield mounting medium for fluorescence with 4′,6-diamidino-2-phenylindole (Vector Laboratories, Inc.). Fluorescent images were acquired by Nikon Digital Eclipse C1 plus confocal microscope (20).
RESULTS
Generation and Characterization of TRC105-Fab
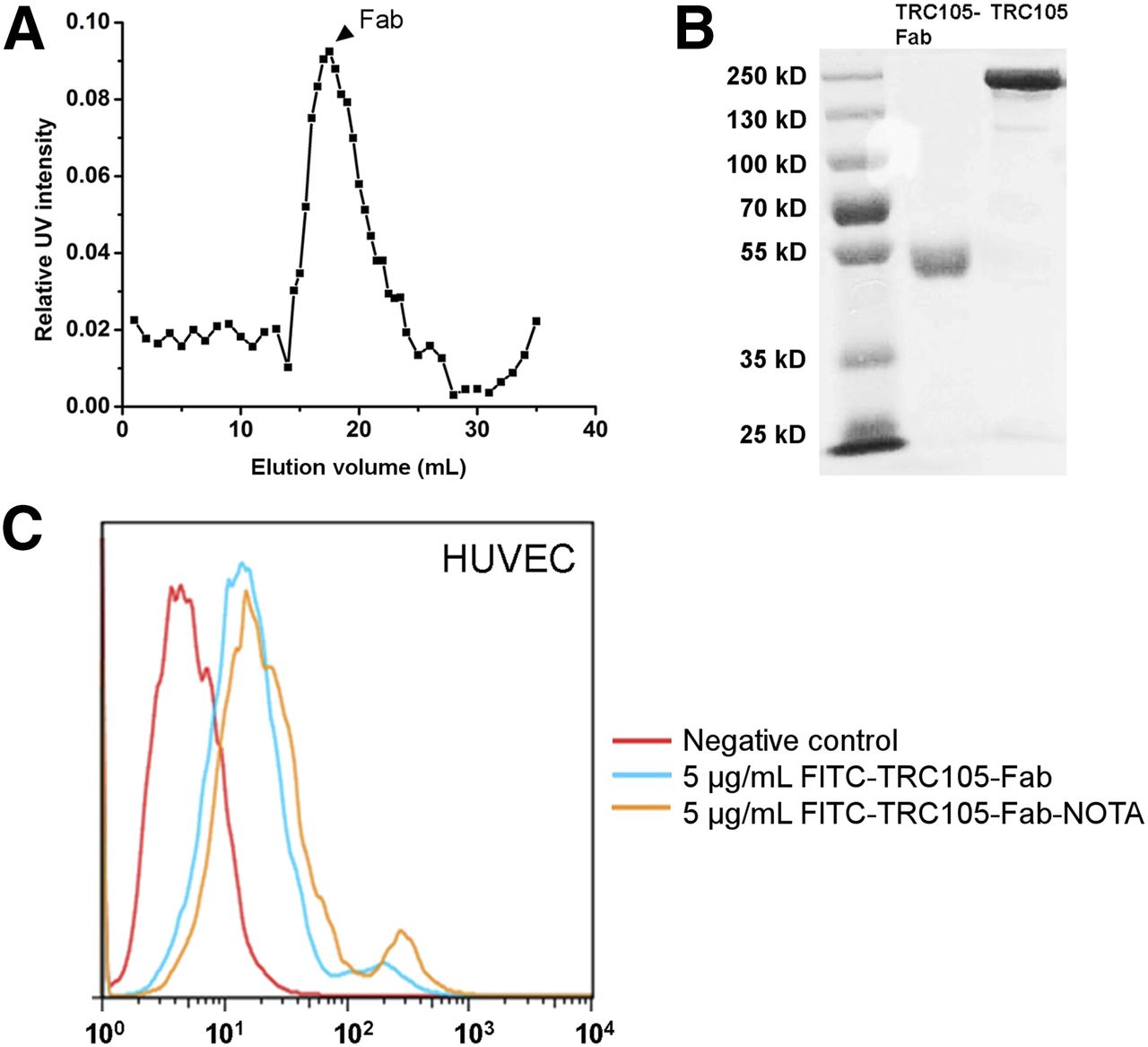
The elution profile of the TRC105-Fab showed a narrow peak in ultraviolet intensity between 16 and 18 mL, indicating a high purity (Fig. 1A). This fraction was used for further studies. A narrow band corresponding to a molecular weight of 50–55 kDa was observed in SDS-PAGE (Fig. 1B), further confirming the purity of TRC105-Fab.

Purification and characterization of TRC105-Fab. (A) Elution profile of TRC105-Fab from Sephadex G-75 column. Arrowhead = single fraction used for further in vitro and in vivo studies. (B) SDS-PAGE of TRC0105 (left) and TRC105-Fab (right). (C) Flow cytometry analysis of FITC-TRC105-Fab and FITC-TRC105-Fab-NOTA (5 ug/mL) in HUVECs. UV = ultraviolet.
Flow Cytometry
CD105 is highly expressed on HUVECs (27). Our previous studies have documented that TRC105 possesses superior binding affinity and specificity to CD105 (20,27,30). Flow cytometry was used to examine the targeting efficiency of TRC105-Fab in vitro. After the treatment with 5 ug of FITC-TRC105-Fab per milliliter, the fluorescence signal from the HUVECs exhibited an approximately 4-fold increase over the negative control (PBS-treated HUVECs) (Fig. 1C), indicating that TRC105-Fab could efficiently bind to CD105, although with a lower binding affinity than the intact antibody. In addition, a similar increase was observed after incubating the cells with 5 ug of FITC-TRC105-Fab-NOTA per milliliter, suggesting that NOTA conjugation does not compromise the binding affinity of FITC-TRC105-Fab.
PET Imaging and Biodistribution Studies
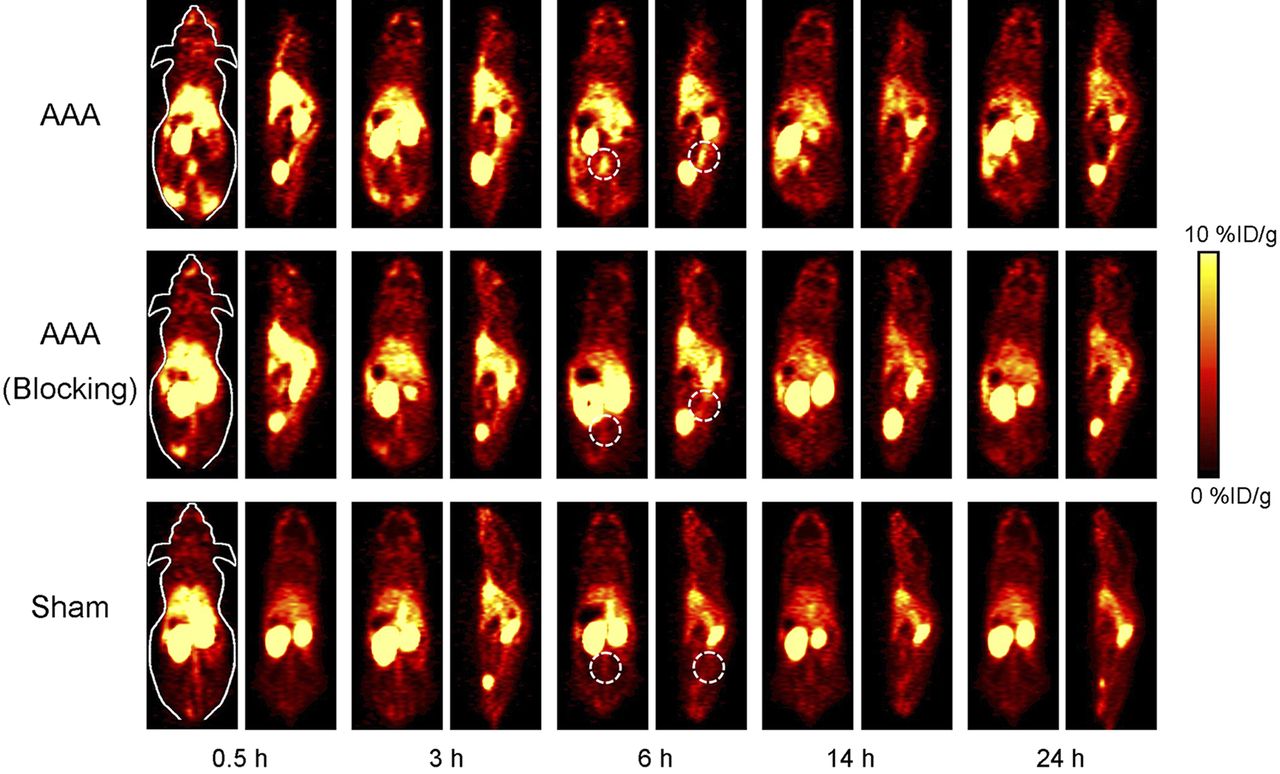
On day 5 after AAA induction, a significantly higher tracer uptake was observed in the aortic region of the animals from the AAA group as early as 0.5 h after injection, remaining relatively stable up to 24 h after injection (9.4 ± 0.1, 9.3 ± 0.7, 9.5 ± 0.4, 7.9 ± 0.5, and 7.9 ± 0.4 %ID/g at 0.5, 3, 6, 16, and 24 h after injection, respectively; n = 3; Figs. 2 and 3A). On day 12, the uptake in the aortas of the animals from the AAA group was still high (8.0 ± 1.5, 7.9 ± 1.2, 7.2 ± 1.4, 5.8 ± 1.0, and 5.4 ± 1.5 %ID/g at 0.5, 3, 6, 16, and 24 h after injection, respectively; n = 3; Figs. 3B and 4), although a little lower in comparison to the first week. This result suggests that 64Cu-NOTA-TRC105-Fab could efficiently target AAA, and the extent of angiogenesis in AAA is stronger on day 5 than day 12, as shown by higher tracer uptake on day 5.

In vivo PET imaging on day 5. Serial coronal and sagittal PET images were acquired at different time points after injection of 64Cu-NOTA-TRC105-Fab in AAA-induced mice, AAA-induced mice preinjected with 2 mg of TRC105 (blocking), and sham group without AAA induction on day 5 after induction.

ROI analysis of PET images. (A) 64Cu-NOTA-TRC105-Fab uptake (%ID/g) in AAA, blocking, and sham groups, on day 5 after induction. (B) 64Cu-NOTA-TRC105-Fab uptake (%ID/g) in AAA, blocking, and sham groups, on day 12 after induction. (C) Comparison of aorta-to-muscle ratios in AAA, blocking, and sham groups on day 5 after induction. (D) Comparison of aorta-to-muscle ratios in AAA, blocking, and sham groups on day 12 after induction. Differences of aorta uptake and aorta-to-muscle ratio in 3 groups were statistically significant (P < 0.05) at all time points (n = 3) tested by 1-way ANOVA.

In vivo PET imaging on day 12. Serial coronal and sagittal PET images were acquired at different time points after injection of 64Cu-NOTA-TRC105-Fab in AAA-induced mice, AAA-induced mice preinjected with 2 mg of TRC105 (blocking), and sham group without AAA induction on day 12 after induction.
The in vivo targeting specificity of 64Cu-NOTA-TRC105-Fab was confirmed with blocking studies on both day 5 and day 12. The signal from aorta in the blocking group was much lower than that in the AAA group and decreased significantly from 0.5 h to 24 h after injection (day 5: 7.1 ± 0.9, 6.3 ± 0.8, 5.5 ± 1.0, 4.2 ± 0.4, and 3.4 ± 0.2 %ID/g; day 12: 5.7 ± 0.8, 4.5 ± 0.2, 4.5 ± 0.5, 3.1 ± 0.3, and 3.0 ± 0.1 %ID/g at 0.5, 3, 6, 16, and 24 h after injection, respectively; n = 3; Figs. 2, 3A, 3B, and 4). The signal from normal aorta was also lower throughout the scans on both day 5 and day 12 in the sham group (day 5: 4.8 ± 0.6, 4.2 ± 1.1, 3.4 ± 0.1, 3.0 ± 0.5, and 2.5 ± 0.3 %ID/g; day 12: 4.8 ± 0.4, 4.3 ± 0.2, 3.7 ± 0.2, 3.2 ± 0.1, and 3.0 ± 0.5 %ID/g at 0.5, 3, 6, 16, and 24 h after injection, respectively; n = 3; Figs. 2, 3A, 3B, and 4). Taken together, a great enhancement in aortic uptake was achieved in an AAA animal model using 64Cu-NOTA-TRC105-Fab, suggesting its superior efficiency and specificity in CD105 targeting. The signals from normal tissues were similar in AAA, blocking, and sham groups at all time points (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org), indicating consistent pharmacokinetics of 64Cu-NOTA-TRC105-Fab and accuracy of ROI analysis.
64Cu-NOTA-TRC105-Fab yielded low levels of background signal in the abdominal area, probably because it was mainly cleared though the kidneys (Figs. 2 and 4). The aorta-to-muscle ratio was measured as a standard of imaging contrast. On day 5 and day 12, the aorta-to-muscle ratio was much higher in the AAA group (day 5: 7.3 ± 0.7, 6.6 ± 0.8, 7.3 ± 0.9, 6.0 ± 0.4, and 5.4 ± 1.0; day 12: 8.0 ± 1.8, 6.5 ± 1.0, 5.6 ± 1.1, 5.1 ± 0.9, and 4.1 ± 0.5 at 0.5, 3, 6, 16, and 24 h after injection, respectively; n = 3; Figs. 3C and 3D), compared with the blocking (day 5: 5.4 ± 0.9, 4.9 ± 0.7, 4.3 ± 0.8, 3.8 ± 0.5, and 2.7 ± 0.2; day 12: 4.5 ± 0.8, 3.5 ± 0.3, 3.2 ± 0.3, 2.4 ± 0.2, and 2.2 ± 0.1 at 0.5, 3, 6, 16, and 24 h after injection, respectively; n = 3; Figs. 3C and 3D) and sham groups (day 5: 3.9 ± 1.0, 3.3 ± 0.9, 2.7 ± 0.3, 2.6 ± 0.4, and 2.1 ± 0.3; day 12: 3.4 ± 0.3, 3.1 ± 0.3, 2.7 ± 0.2, 2.5 ± 0.2, and 2.4 ± 0.4 at 0.5, 3, 6, 16, and 24 h after injection, respectively; n = 3; Figs. 3C and 3D). The data clearly demonstrate that excellent imaging contrast can be achieved in AAA with 64Cu-NOTA-TRC105-Fab probe.
To confirm the accuracy of PET images and ROI analysis, mice in all 3 groups were sacrificed at 24 h after injection on day 12. Aorta and other major organs were collected, and the radioactivity signals were measured with a γ counter. The quantitative data from biodistribution and ROI analysis matched well (Fig. 5). Of note, kidney uptake was significantly higher than the liver uptake in the biodistribution study, further validating the renal clearance of 64Cu-NOTA-TRC105-Fab. More important, low uptake observed in the intestine and muscles explains the low background signal and hence superior imaging contrast of 64Cu-NOTA-TRC105-Fab in AAA.

Biodistribution of 64Cu-NOTA-TRC105-Fab in AAA, blocking, and sham groups 24 h after injection on day 12 after induction (n = 3). p.i. = after administration.
Ex Vivo Imaging and Histology
A macroscopically visible aneurysmal dilation was observed in the abdominal aortas of mice from the AAA group 5 d after induction (Supplemental Fig. 2). Ex vivo autoradiography revealed a higher signal in the aortas from the AAA group than the aortas from blocking and sham groups (Fig. 6A), further confirming the accuracy of the results from PET imaging, ROI analysis, and biodistribution studies. Flattening and degradation of the elastic lamina due to increased diameter was obvious in hematoxylin and eosin staining of the dilated aorta (Fig. 6B). The external diameter of the aorta was 0.9 ± 0.1 mm in the AAA group on day 5, whereas it was only 0.4 ± 0.01 mm in the normal aorta.

Ex vivo analysis. (A) Autoradiography of abdominal aorta from AAA, blocking, and sham groups with 64Cu-NOTA-TRC105-Fab. (B) Hematoxylin and eosin staining of AAA and normal aorta. (C) Immunofluorescence histology of AAA samples collected from AAA group on day 5 and day 12 after induction and normal aorta collected from normal mouse. Red fluorescence indicates CD31 expression, and green fluorescence indicates CD105 expression. Nuclei were counterstained with 4′,6-diamidino-2-phenylindole (DAPI). Max = maximum; min = minimum.
The intensity of CD105 immunofluorescence was highest on day 5, suggesting active angiogenesis after AAA induction (Fig. 6C). The fluorescence intensity was similar to the normal aorta on day 12. These results correlated well with PET imaging results. Taken together, CD105 was highly expressed in AAA at day 5 after induction, accompanied with structural change of aortic wall, matching well with in vivo and ex vivo studies.
DISCUSSION
In management of AAA, clinicians are often faced with the important decision of whether to perform invasive repair or to manage the condition conservatively. This obstacle arises from the lack of methods that enable the noninvasive acquisition of molecular–cellular information in the developing AAA. Current guidelines recommend endovascular repair or surgery if the aortic diameter exceeds 5.5 cm and follow-up with anatomic imaging every 3–6 mo for aneurysms above 4 cm. However, the size of AAA is neither the sole nor the most accurate determinant for the risk of rupture (31). Individual risk is also influenced by sex, age, smoking, and comorbidities, but its assessment is rarely easy because reliable methods for the optimal evaluation of these variables are not readily available. This situation often leads to difficulties in decision making, and many patients are unnecessarily exposed to the risks of reparative surgery when their aneurysm might never have ruptured if left untreated (32). Serial monitoring of the biologic activity of AAA would be ideal to identify high-risk patients and prompt earlier therapy to prevent rupture while also sparing low-risk patients from expensive and morbid procedures (33).
To date, PET imaging of AAA has been mostly performed with 18F-FDG (5–10,34–37). One disadvantage of 18F-FDG is nonspecific uptake by inflammatory tissues (38), which may lead to false-positive results if there is an inflammatory disease in the artery wall other than AAA. Additionally, the correlation between 18F-FDG uptake in AAA and the chronic inflammation observed in the wall of asymptomatic AAAs is controversial, so metabolic activity of inflammatory cells in asymptomatic AAAs was not sufficient to result in an increased glucose metabolism detectable by 18F-FDG PET (10,39), possibly leading to false-negative results. We also tested the imaging capacity of 18F-FDG in AAA in this study, but we could not detect a significant difference between aortic signals in normal mice and mice with AAA (Supplemental Figs. 3 and 4). On the contrary, the increased expression of CD 105 in AAA could be detected with high sensitivity and specificity using TRC105-Fab. CD105 is expressed on inflamed and some normal tissues to a certain extent, but the expression on endothelial cells is significantly higher (40). Therefore, CD105 has been accepted as an important angiogenesis marker (20). 64Cu-NOTA-TRC105-Fab possesses excellent binding efficiency and high targeting specificity toward CD105 as validated by in vitro flow cytometry and in vivo PET imaging in our study. The selective binding ability of the probe may facilitate the differential diagnosis of inflammatory arterial diseases and AAA, therefore preventing false results in PET imaging of AAA.
Antibody-based PET tracers are generally not suitable for AAA imaging because of the hepatic clearance and relatively high intestine uptake, yielding a high background in the abdominal area. However, because of its small size (50–55 kDa), TRC105-Fab was cleared mainly through the renal pathway and taken up minimally by the intestines, as we documented with ex vivo biodistribution studies, providing a superior imaging contrast. TRC105-Fab also had a shorter blood half-life (2.1 h; Supplemental Fig. 5), in comparison with TRC105 (half-life, 3.5 h) (30). However, the blood half-life is still longer than that of small molecules, possibly leading to inaccuracy of AAA uptake. Therefore, more comparative imaging experiments with different targeting probes and imaging modalities are needed in future studies to confirm the potential of TRC105-Fab for PET imaging of AAA.
The limitation to the current preliminary study is the experimental AAA model. Although the murine model has biologic features found in human AAA (28), it does involve aortic dissection as part of the AAA expansion process and may not be ideal to study AAA rupture. Moreover, murine AAA develops over weeks, rather than decades, so the model might not fully represent human AAA in terms of biology and progression (33). Prospective outcome studies are needed first with more clinically relevant animal models of AAA and eventually in patients. These trials will determine whether an increased PET signal, despite the limited spatial resolution of PET, can indeed predict aneurysm rupture.
CONCLUSION
In this study, we demonstrated an increased expression of CD105 in AAA and defined a high-specify, high-sensitivity probe for the in vivo PET imaging of AAA with TRC105-Fab. More important, we achieved an exquisite imaging contrast because of the low background in the abdominal area. The as-designed imaging probe might open new avenues into AAA research, which will eventually benefit the health care of the whole AAA patient population.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work is supported, in part, by the University of Wisconsin–Madison, the Department of Defense (W81XWH-11-1-0644 and W81XWH-11-1-0648), the National Science Foundation (DGE-1256259), the National Institutes of Health (NIBIB/NCI 1R01CA169365, P30CA014520, 5T32GM08349, and T32CA009206), and the American Cancer Society (125246-RSG-13-099-01-CCE). Charles P. Theuer is an employee of TRACON Pharmaceuticals, Inc. The other authors declare that they have no conflict of interest. No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Apr. 16, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 15, 2014.
- Accepted for publication March 31, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Gallium-67/68-Labeled Antibody Fragment for Immuno-SPECT/PET Shows Low Renal Radioactivity Without Loss of Tumor Uptake
- Molecular Characterization of High-Risk Aortic Aneurysms: Imaging Beyond Anatomy
- Molecular Fingerprint for Terminal Abdominal Aortic Aneurysm Disease
- A Novel Fusion of ALT-803 (Interleukin (IL)-15 Superagonist) with an Antibody Demonstrates Antigen-specific Antitumor Responses
- Dual Targeting of Tissue Factor and CD105 for Preclinical PET Imaging of Pancreatic Cancer
- Novel Molecular Imaging Approaches to Abdominal Aortic Aneurysm Risk Stratification