


Article Figures & Data
Figures
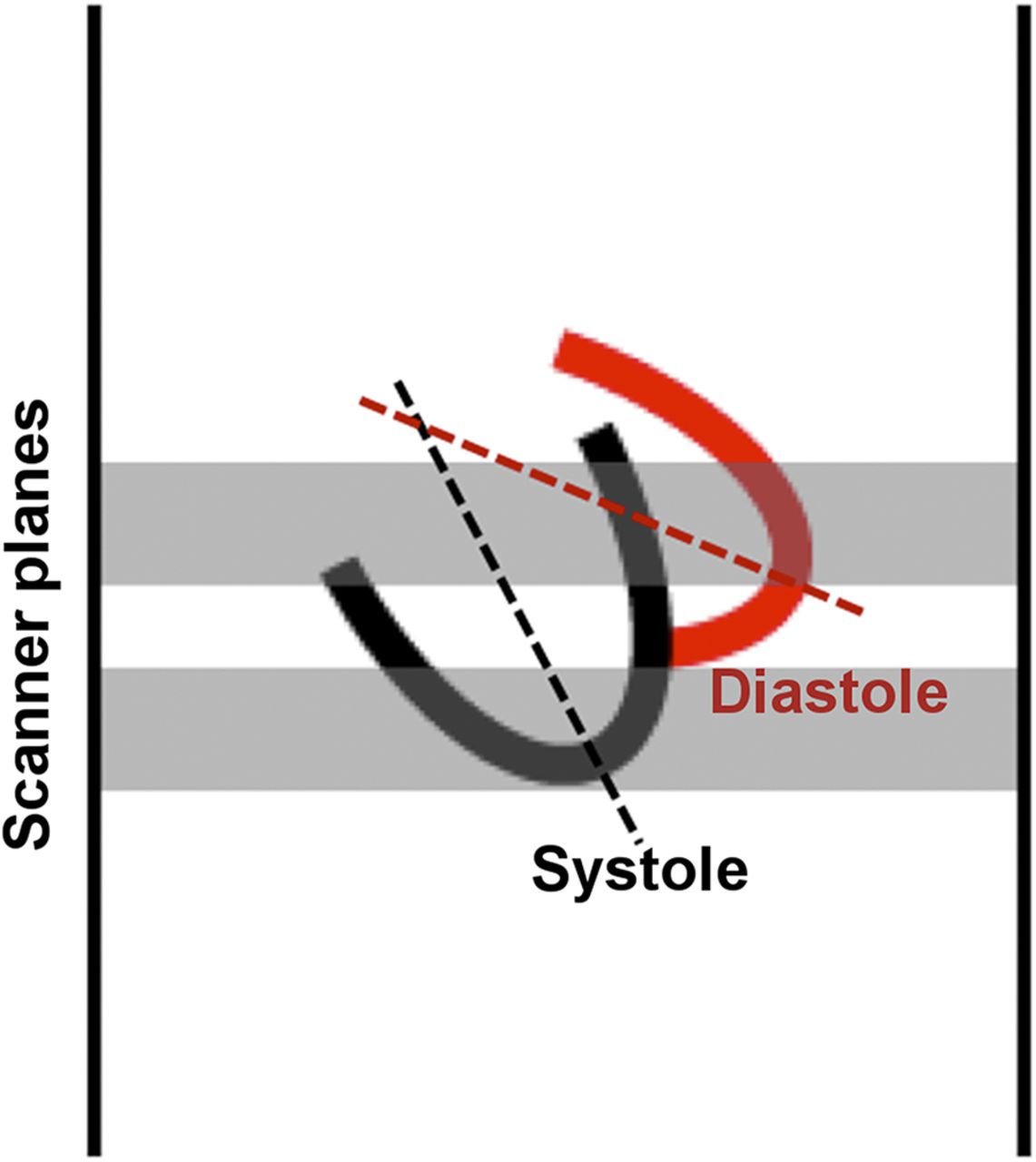
- FIGURE 1.
Medial and downward recoil of left ventricle during systole may move inferior myocardium into and out of the most inferior imaging plane, thereby reducing inferior activity, especially for inferior apex, with resulting artifact in conventional whole-cycle images not present on systolic images.
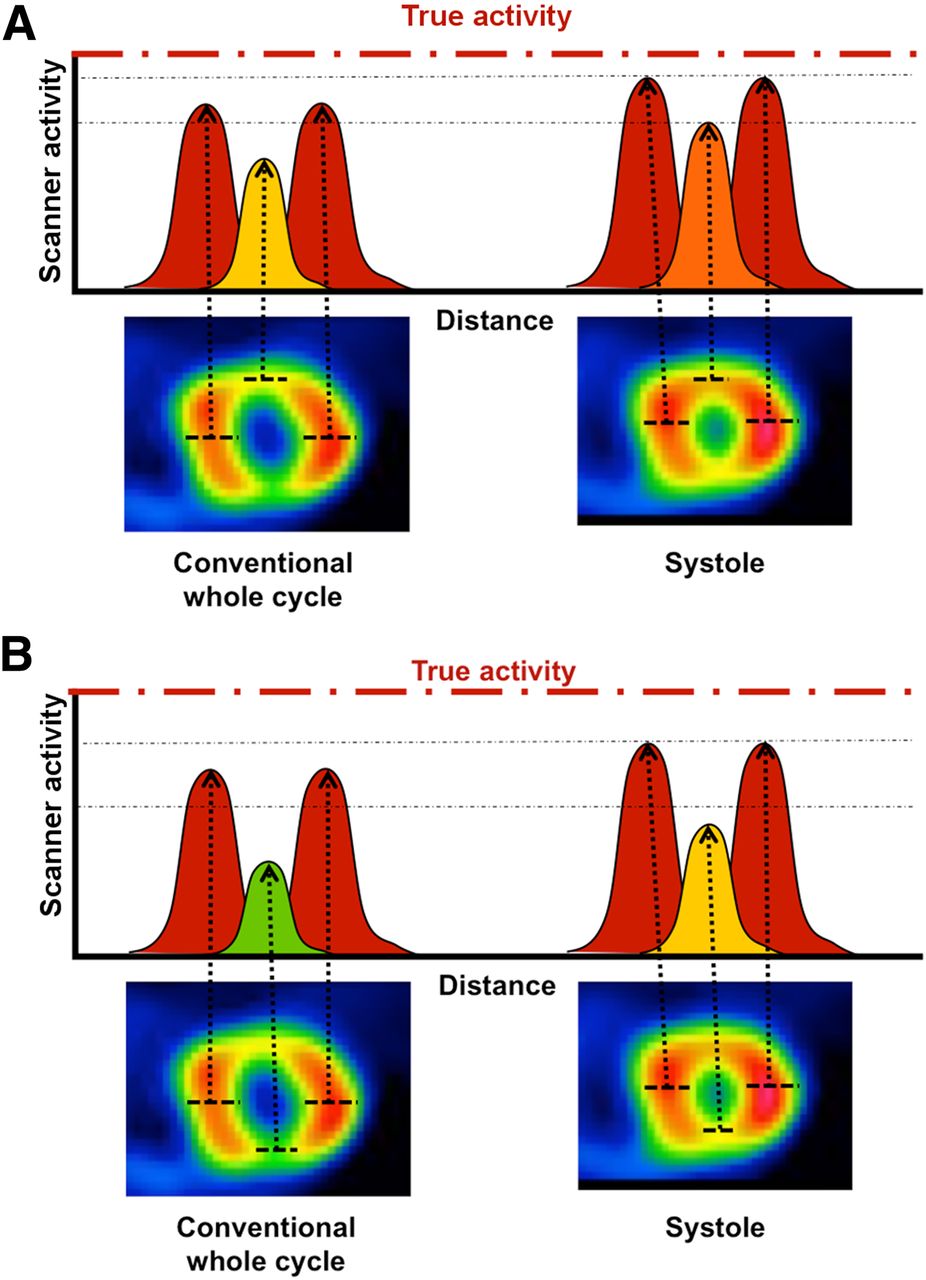
- FIGURE 2.
In this example with normal angiogram, red dashed line indicates schematically true activity that scanners typically do not recover because of limited resolution and efficiency. Scanner activity recovery in anterior and inferior walls is less on conventional whole-cycle images than systolic images because of limited scanner resolution and partial-volume loss for diastolic images or cardiac motion. This difference between systolic and conventional whole-cycle relative images is less prominent for lateral walls because of their greater thickness due to papillary muscles and associated better activity recovery. (A) In systole, LV walls are thickened with better activity recovery by scanner such that anterior defect normalizes on systolic images, suggesting that defect on conventional image is artifact due to partial-volume loss. (B) Activity recovery profiles for inferior wall during systole compared with anterior defect. This inferior defect also substantially improves to nearly normal on systolic images, suggesting that defect in whole-cycle image is artifact. Some residual attenuation is likely due to diaphragm and liver.
- FIGURE 3.
(A) Anterior stress perfusion defect on whole-cycle image not present on systolic images suggesting that defect on whole-cycle image is artifact as confirmed by normal coronary angiogram. (B) Inferior stress perfusion defect on both whole-cycle and systolic images indicating true perfusion defect as confirmed by coronary angiogram.
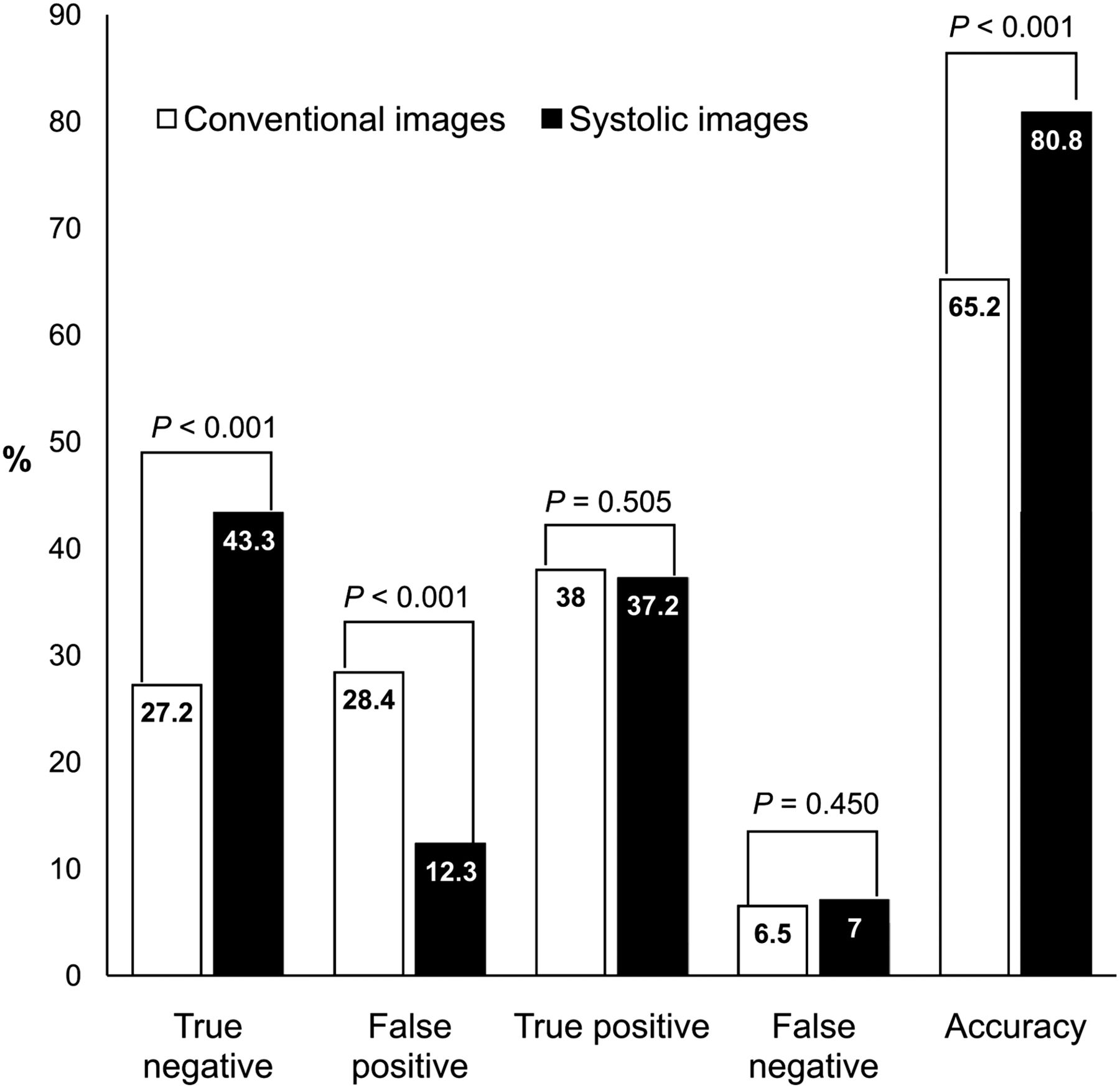
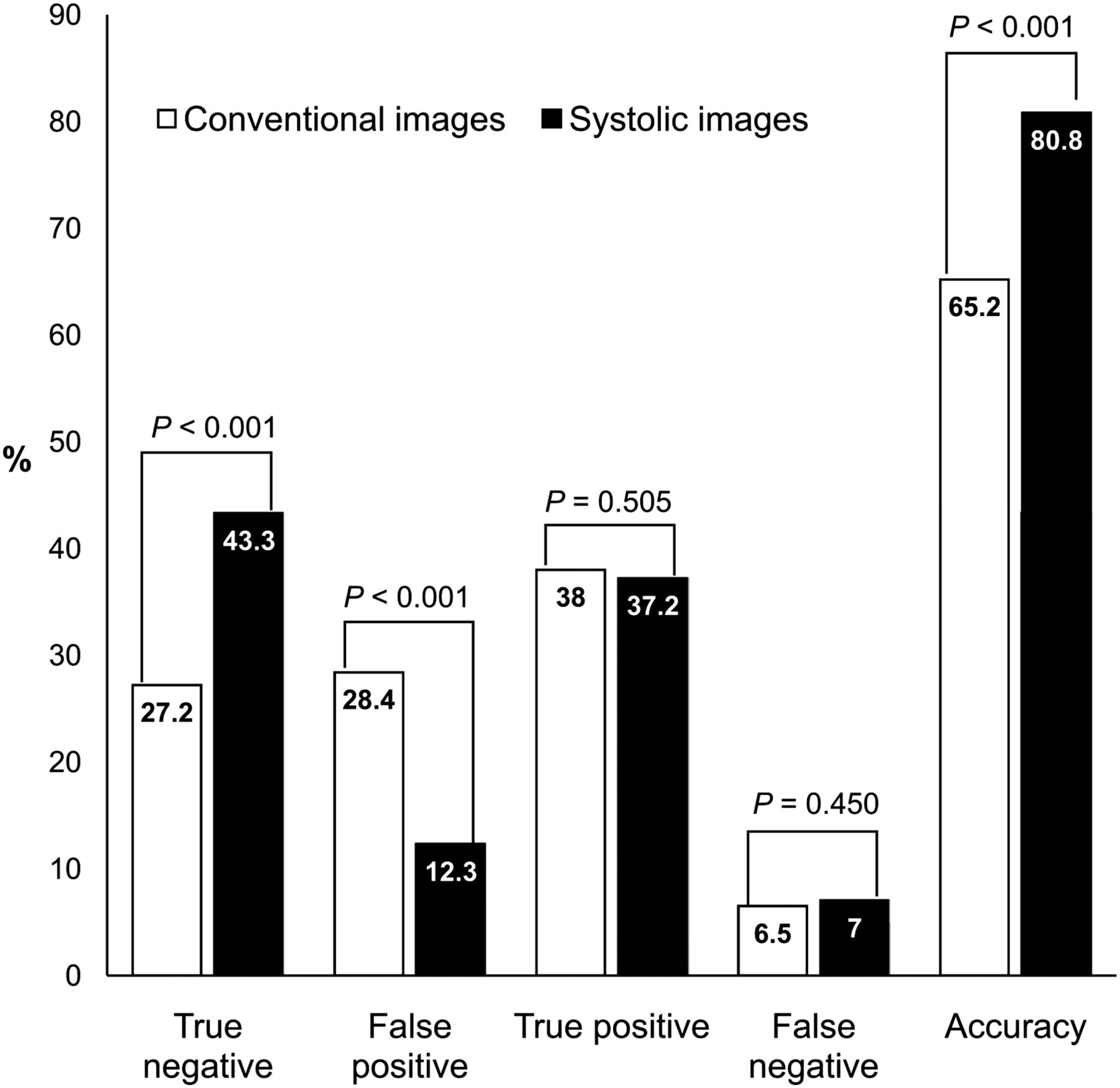
- FIGURE 4.
Bar graph demonstrates result of considering systolic images in interpretation of whole-cycle conventional images compared with coronary angiogram.



Tables
Characteristic No CAD (n = 335) CAD (n = 268) P Age (y) 54.8 ± 11.3 60.9 ± 11.5 <0.001 Male 187 (55.8) 179 (66.8) 0.007 Tobacco use 46 (13.7) 58 (21.6) 0.013 Hypertension 297 (88.7) 249 (92.9) 0.092 Diabetes 128 (38.2) 144 (53.7) <0.001 Dyslipidemia 183 (54.6) 188 (70.1) <0.001 Family history of premature CAD 19 (5.7) 28 (10.5) 0.033 Type of stress test Adenosine 289 (86.3) 240 (89.6) 0.261 Exercise 34 (10.2) 18 (6.7) 0.147 Regadenoson 9 (2.7) 7 (2.6) 0.999 Dobutamine 3 (0.9) 3 (1.1) 0.999 Values are n, with percentage in parentheses, or mean ± SD. P < 0.05 = statistically significant.
Coronary angiogram Patient (n = 268) CAD 3-vessel disease 50 (18.7) 2-vessel disease 68 (25.4) 1-vessel disease 147 (54.9) Coronary artery involvement Left main 15 (5.6) Left anterior descending 165 (61.6) Left circumflex artery 117 (43.7) Right coronary artery 146 (54.5) Values are n, with percentage in parentheses.
- TABLE 3
Interpretation Result by Conventional and Systolic Images in Patients With and Without CAD
SPECT score No CAD (n = 335) CAD (n = 268) P Conventional images SRS 2.2 ± 2.3 7.6 ± 7.3 <0.001 SSS 3.0 ± 2.6 9.2 ± 7.4 <0.001 SDS 0.8 ± 1.7 1.6 ± 2.6 <0.001 Systolic images Systolic SSS 2 ± 2.3 9.1 ± 7.6 <0.001 Systolic SDS −0.3 ± 1.8 1.6 ± 2.8 <0.001 Left ventricular ejection fraction (%) 61.6 ± 9.8 50.6 ± 15.8 <0.001 Values are mean ± SD. Normal study = SSS < 4 and SDS < 2, P < 0.05 = statistically significant.
Patient group Whole cycle SSS ± SD Systolic SSS ± SD P ΔSSS No CAD (n = 335) 3.0 ± 2.6 2.0 ± 2.3 <0.001 −1 ± 1.2* CAD (n = 268) 9.2 ± 7.4 9.1 ± 7.6 0.559 −0.1 ± 1.3* Values are mean ± SD. ΔSSS = difference between SSS and systolic SSS, normal study = SSS < 4 and SDS < 2, *P < 0.001, P < 0.05 = statistically significant.
Accuracy Patient group Unchanged* Conventional images Systolic images P All patients (n = 603) 499 (82.8%) 393 (65.2%) 487 (80.8%) <0.001 SSS ≤ 8 (n = 481) 377 (78.4%) 282 (58.6%) 376 (78.2%) <0.001 SSS > 8 (n = 122) 122 (100%) 111 (91%) 111 (91%) — *Result of interpretation was not altered by systolic images from normal to abnormal or abnormal to normal, normal study = SSS < 4 and SDS < 2, P value < 0.05 = statistically significant.
Values are n, with percentages in parentheses.





{kind=link}
{kind=link}
{kind=link}
{kind=link}