


Abstract
The nicotine metabolite ratio (NMR), a stable measure of hepatic nicotine metabolism via the CYP2A6 pathway and total nicotine clearance, is a predictive biomarker of response to nicotine replacement therapy, with increased quit rates in slower metabolizers. Nicotine binds directly to nicotinic acetylcholine receptors (nAChRs) to exert its psychoactive effects. This study examined the relationship between NMR and nAChR (α4β2* subtype) availability using PET imaging of the radiotracer 2-18F-fluoro-3-(2(S)-azetidinylmethoxy)pyridine (2-18F-FA-85380, or 2-18F-FA). Methods: Twenty-four smokers—12 slow metabolizers (NMR < 0.26) and 12 normal metabolizers (NMR ≥ 0.26)—underwent 2-18F-FA-PET brain imaging after overnight nicotine abstinence (18 h before scanning), using a validated bolus-plus-infusion protocol. Availability of nAChRs was compared between NMR groups in a priori volumes of interest, with total distribution volume (VT/fP) being the measure of nAChR availability. Cravings to smoke were assessed before and after the scans. Results: Thalamic nAChR α4β2* availability was significantly reduced in slow nicotine metabolizers (P = 0.04). Slow metabolizers exhibited greater reductions in cravings after scanning than normal metabolizers; however, craving was unrelated to nAChR availability. Conclusion: The rate of nicotine metabolism is associated with thalamic nAChR availability. Additional studies could examine whether altered nAChR availability underlies the differences in treatment response between slow and normal metabolizers of nicotine.
An estimated 43.8 million Americans and 1.1 billion people worldwide smoke cigarettes (1,2). Tobacco use is the leading cause of preventable death, representing a significant medical and public health problem (3). Despite the burden of nicotine dependence on public health, available pharmacotherapies have long-term failure rates of 70%–80% (4).
Individual differences in rate of nicotine metabolism via CYP2A6 have been linked to variation in smoking rates (i.e., cigarettes per day) (5,6). The ratio of 3′-hydroxycotinine to cotinine, referred to as the nicotine metabolite ratio (NMR), has been validated as a measure of inherited differences in hepatic metabolism of nicotine and as a predictor of both total nicotine clearance and response to smoking cessation therapies (7,8). Smokers who are normal metabolizers of nicotine are less likely to quit smoking with transdermal nicotine than slow metabolizers (7,9). A recent multicenter, randomized, placebo-controlled trial of 1,246 smokers showed that varenicline was more efficacious than the nicotine patch in normal metabolizers as measured by NMR; however, in slow metabolizers, these treatments had equivalent efficacy (10). Among pregnant women, who clear nicotine at higher rates than nonpregnant women, those with a higher NMR were also less likely to achieve cessation (11). Despite the validated clinical significance of the NMR for targeting smoking cessation therapy, the mechanisms underlying its association with treatment response are unknown. This study examined whether slow and normal metabolizers differ in nAChR availability after approximately 18 h of abstinence from nicotine. We focused on short-term abstinence because ability to refrain from nicotine during the first day of an attempt to quit is highly predictive of long-term abstinence (12,13).
Chronic nicotine exposure in both animal models and humans has been shown to increase nAChR density, based on immunohistochemistry and other in vitro molecular probes specific for the nAChR α4β2* subtype (14–18). PET imaging and SPECT using 2-18F-fluoro-3-(2(S)-azetidinylmethoxy)pyridine (2-18F-FA-85380, or 2-18F-FA) and 123I-5-IA, respectively, have confirmed these results in vivo in humans (19–21). Specifically, chronic nicotine exposure leads to nAChR upregulation (22), whereas quitting smoking leads to decreased receptor levels (i.e., normalization) (23). SPECT molecular imaging studies of the nAChR α4β2* subtype have also shown that nAChR availability in smokers peaks after 1 wk of abstinence (22,24), suggesting the persistent occupation of nAChRs by nicotine. These studies have consistently shown the highest density of nAChRs (α4β2* subtype) to be in the thalamus (21). Studies have also shown that smoking, exposure to secondhand smoke, and administration of the smoking cessation medication varenicline displaces 2-18F-FA and 123I-5-IA binding to the α4β2* receptor subtype (25–28). On the basis of these data, we hypothesized that slow nicotine metabolizers would have lower nAChR availability after overnight nicotine abstinence than normal metabolizers. Changes in nAChR availability have been observed in the thalamus and cortex (25,26,29), and for that reason our a priori analysis targeted the thalamus, frontal cortex, temporal cortex, and whole brain.
MATERIALS AND METHODS
Participants
This study was conducted in accordance with the Declaration of Helsinki, and the University of Pennsylvania Institutional Review Board approved all procedures. Individuals who expressed interest in participating in smoking cessation research at the University of Pennsylvania completed an in-person intake session during which they provided written informed consent and were screened for eligibility. Eligible participants were between the ages of 18–65 y and reported smoking at least 10 cigarettes per day for the past 6 mo (confirmed by an exhaled carbon monoxide [CO] reading greater than 10 parts per million [ppm]) and were fluent English speakers. Persons with a history of DSM Axis I psychiatric or substance disorders (except nicotine dependence), assessed using the Mini International Neuropsychiatric Interview (30), and those taking psychotropic medications were excluded. Other exclusion criteria included current use of chewing tobacco, snuff, or smoking cessation products; pregnancy, planned pregnancy, or breastfeeding; history of brain injury; or MR imaging–contraindicated material in the body.
The NMR was determined from a plasma sample provided at intake (6). Participants were classified as slow metabolizers (NMR < 0.26) or normal metabolizers (NMR ≥ 0.26), based on prior clinical data showing differences in smoking cessation outcomes using this cutoff (7,9). Because slow metabolizers typically compose one fourth of the general population of smokers, we oversampled this group to obtain equal numbers of slow and normal metabolizers. Participants and research staff involved with the PET scans were unaware of NMR. Of 35 eligible participants who scheduled a PET scan, 5 voluntarily withdrew before the PET scan, and 6 were withdrawn from the study because of noncompliance with study requirements (breath alcohol concentration reading > 0.01 or exhaled CO > 15 ppm at the PET scan) or a newly acquired MR imaging contraindication, leaving a final sample of 24 participants (12 slow metabolizers and 12 normal metabolizers). The 15-ppm cutoff for CO was used because overnight abstinence may not be sufficient to clear CO in smokers who have compromised pulmonary function. The average CO reading at session initiation was 8.2 ppm (range: 4–15 ppm). A second CO reading, taken before scanning, averaged 3.5 ppm (range: 2–7 ppm).
Scanning Procedures
Participants were instructed to cease smoking at 9:00 pm on the night before the scan visit. The visit started at 7:30 am the next day, and the scan data acquisition was initiated at 3:00 pm. Thus, there was approximately 18 h of abstinence before scanning. After overnight nicotine abstinence, participants underwent PET brain imaging of 2-18F-FA delivered by bolus plus infusion to shorten the duration of the PET imaging session, which is lengthened by the relatively slow receptor uptake of 2-18F-FA (31). The time period of overnight abstinence was chosen because most smokers relapse in the first 24 h of an attempt to quit (12) and because our primary hypothesis concerned differences in receptor availability in early abstinence due to differences in rates of nicotine metabolism. At the start of the session, participants provided a urine sample for a drug screen, a breath alcohol sample (>0.01 exclusionary), and a breath CO sample for biochemical confirmation of abstinence (CO < 15 ppm, or at least a 50% reduction from the intake session). During the PET scan, 2-18F-FA (113.96–217.56 MBq [3.08–5.88 mCi]) was administered as a 50% bolus initially with additional 2-18F-FA (115.07–222 MBq [3.11–6.0 mCi]) (50%) administered as a continuous infusion over 8 h. Participants completed 2 h of brain scanning beginning 6 h (±30 min) after injection to allow the radiotracer to achieve a steady state (31). PET scanning was performed on a Gemini TruFlight (TF) Big Bore PET/CT scanner (Philips Healthcare). A low-dose (120 kVp, 50 mAs) unenhanced CT scan of the head was performed before the emission acquisition for attenuation correction. PET images were reconstructed via an iterative line-of-response row-action maximum-likelihood algorithm using 2 iterations and 4 subsets and the sharp filter setting. Just before and immediately after the 2-h PET scan, participants completed the Brief Questionnaire on Smoking Urges (32), a validated measure of cravings to smoke.
To facilitate automatic generation of brain volumes of interest (VOIs), all participants received a T1-weighted anatomic scan on a Siemens MR scanner, with 3 participants on a 3-T Magnetom Sonata Syngo and 21 participants on a 1.5-T Magnetom Trio A Tim, acquired using magnetization-prepared 180° radiofrequency pulses and rapid gradient-echo sampling. Subjects underwent MR scanning at a session different from the PET scan.
Measurement of Unbound, Unmetabolized 2-18F-FA in Plasma
Baseline venous blood samples were obtained before injection for assessment of 2-18F-FA binding to plasma proteins, measurement of serum nicotine levels, and preparation of standards for the solid phase extraction process. The average nonmetabolized concentration of free 2-18F-FA in plasma during the scan period was determined from an average of 5.8 blood samples (range, 3–6 samples; SD, ±0.7) for each participant from 5 h to 7.5 h after bolus injection. 2-18F-FA binding to plasma proteins was evaluated by ultrafiltration using YM-10 filtration devices (Millipore Corp.). Additional venous blood samples (∼3 mL) were drawn at predetermined intervals during the infusion period for measurement of unbound, nonmetabolized 2-18F-FA. Samples were centrifuged at 4,000 × g for 15 min, and plasma radioactivity was measured using an automated γ counter. Radioactivity attributable to nonmetabolized 2-18F-FA was determined using solid phase extraction with Clean Screen extraction columns (200 mg/10 mL; United Chemical Technologies, Inc.) (33).
Data Analysis
PET Analysis Including Automatic Generation of Brain VOIs and Partial Volume Correction
To standardize the PET imaging acquisition times after radiotracer administration across all subjects, we used only the 90 min of PET scanning that was contemporaneous for all participants—6.25–7.75 h after bolus injection—using six 15-min time bins (mean midpoint of scans was 7.0 ± 0.1 h after bolus injection). Each participant’s PET image and T1-weighted MR scan were coregistered, and brain VOIs were automatically defined using the T1-weighted MR imaging parcellation PNEURO tool in PMOD software (PMOD Technologies Ltd., version 3.5). Mean regional time–activity curves were output by PMOD software with partial volume correction based on a variant of the Rousset correction method, whereby 15% of the pixels in the inner VOI were used for calculating the VOI average. Average activity concentrations for the 90-min period were decay-corrected to the time of bolus injection for use in subsequent calculations.
Calculation of Total Distribution Volume (VT/fP)
VT/fP was calculated as the ratio of average, partial volume–corrected 2-18F-FA concentration in brain to unbound, nonmetabolized 2-18F-FA concentration in plasma (31).
Generation of Mean PET Images for Participant Cohorts
Using each participant’s calculated distribution volume (VT/fP), mean images of participant VT/fPs were created, with both PET image and plasma activity concentrations decay-corrected to the time of 2-18F-FA bolus injection. All participants’ VT/fP images were spatially normalized to the same template, and the resulting VT/fP images were averaged for participants with normal hepatic nicotine metabolism (n = 12) and for participants with slower rates of hepatic nicotine metabolism (n = 12).
Descriptive statistics were generated for demographic and smoking variables, with differences between NMR groups being tested using t tests and χ2 tests. Group differences in VT/fP in the a priori VOIs were estimated by ANOVA, including age, sex, and average cigarettes per day as covariates; nonsignificant covariates were allowed to drop from the models at a P value of less than 0.1. Associations between VT/fP and craving were tested using regression models including mean QSU total score as the outcome and VT/fP in the a priori regions as the primary predictor. α was adjusted on the basis of 4 VOIs with an average correlation of 0.95, resulting in an adjusted P value of 0.047. Twenty-four smokers provided 80% power to detect an NMR group-effect size of 1.2 (34).
RESULTS
Demographic statistics for the study sample are summarized in Table 1. There were no significant differences in age, sex, race, cigarettes per day, or Fagerström Test for Nicotine Dependence score between the NMR groups (P > 0.05).
Demographic and Smoking-Related Variables at Baseline
Receptor availability was significantly greater (as measured by 2-18F-FA VT/fP) in normal metabolizers than it was in slow metabolizers in the thalamus bilaterally, where the concentration of nAChRs is highest (F = 4.921, P = 0.037). Significant associations were not observed in other tested regions: whole brain, temporal lobes, and frontal lobes; however, trends in all regions were observed (Figs. 1 and 2).

2-18F-FA partial volume–corrected VT/fP by region and NMR group: Smokers with slower nicotine metabolism (NMR < 0.26) demonstrated less VT/fP in brain than those with normal metabolism, including in thalamus (P = 0.037), region of greatest nAChR density within CNS. This relationship persisted and approached significance when VT/fP of slow (bottom quartile) and normal NMR groups were compared for entire brain (P = 0.07). P values were calculated using 1-way ANOVA. Error bars show SEM. For whole brain, frontal lobe, thalamus, and temporal lobe, P = 0.07, 0.1, 0.04, and 0.1, respectively. *P < 0.05.
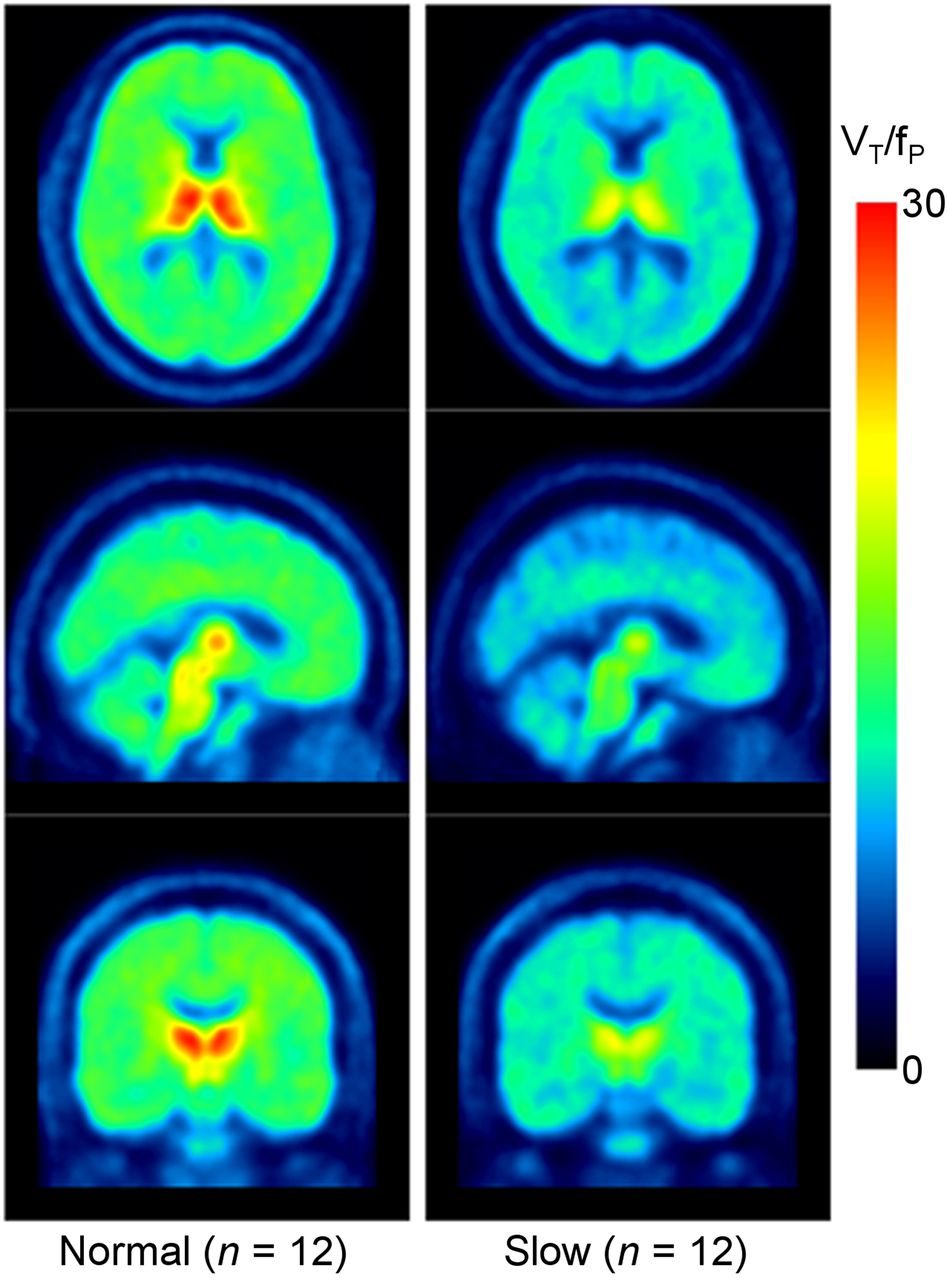
Mean 2-18F-FA VT/fP PET images demonstrating lower 2-18F-FA binding in subgroup with slower hepatic metabolism of nicotine. Mean PET images for normal metabolizers (left) and those with slower rates of hepatic nicotine metabolism (right) were spatially normalized to same template.
There were no significant associations between VT/fP in the 4 VOIs and self-reported urges to smoke. Urges to smoke did not differ between slow and normal metabolizers before scanning; however, the groups differed with respect to changes in urges before and after scanning, with slow metabolizers exhibiting a decrease (mean change in slow metabolizers, −8.1; SE = 2.9) and normal metabolizers showing a slight increase (mean change of +1.8; SE = 2.2).
DISCUSSION
These data suggest that slow metabolizers of nicotine exhibit reduced nAChR availability in the thalamus after 18 h of abstinence from smoking, compared with normal nicotine metabolizers. Individual variation in hepatic metabolism increases the nicotine half-life in plasma from approximately 2 to 4 h (35–37). In addition, nicotine levels in the brain can persist beyond nicotine plasma half-life (22,24). Therefore, differences in thalamic nAChR availability observed between slow and normal metabolizers may reflect differences in nicotine binding to nAChRs that result from differences in elimination kinetics. Nonetheless, other possibilities, such as differences in nAChR expression or binding, should be considered. For example, in nonhuman primates at baseline before nicotine exposure, 2-18F-FA VT/fP binding is believed to be reflective of nAChR expression because the radiotracer does not compete with nicotine as it does in smokers (38). However, definitive measurement of nAChR protein expression requires use of histopathologic techniques (14,39). Binding of the radiotracer with plasma proteins before crossing the blood–brain barrier and interacting with nAChRs could occur, but the established bolus-plus-infusion technique used should account for such an interaction (31). Four of the 24 smokers had persistent nicotine in their blood after overnight abstinence: 3 slow metabolizers and 1 normal metabolizer. These values measured less than 5 ng/mL. Although such levels could interfere with radiotracer binding, we intentionally timed the study so that nicotine might persist in the blood (and brain) of slow metabolizers. Not surprisingly, because of its participation in numerous neuronal circuits, the thalamus has been implicated in nicotine dependence by both functional MR imaging and PET studies (40,41). Although in the present study significance was detected only in the thalamus, the region of greatest nAChR availability, the trend suggests a whole-brain phenomenon. It is possible, however, that overnight abstinence was not sufficient to reveal other involved neuroanatomical locations.
Although validation of these preliminary findings is necessary, the results suggest that normal metabolizers of nicotine, who have faster rates of nicotine elimination, also exhibit greater nAChR availability during the first day after an attempt to quit. Other data show that smokers with a higher specific-binding volume of distribution (a measure of nAChR availability) are more likely to relapse after an attempt to quit (42). Thus, future research could examine whether increased nAChR availability in normal metabolizers mediates the increased likelihood of relapse on nicotine patch or the greater efficacy of varenicline in this group (10).
In addition, although nAChR expression and availability are dynamic and influenced by age, sex, and hormones, including estrogen and progesterone (43), age and sex were not associated with nAChR availability in our sample. The relatively small sample size is another limitation; however, the relationship between NMR and nAChR availability was consistent with the a priori hypothesis. Prior 2-18F-FA-PET imaging studies have used abstinence periods of at least 36–48 h to ensure complete depletion of nicotine. Future studies in slow and normal metabolizers that include a second scan at least 1 wk later would be valuable to explore whether differences in availability can be attributed to long-term occupancy or upregulation.
It is also important to note that the nAChR, a nonselective cation channel, may exist in multiple conformational states (44). Binding of an agonist such as nicotine may stabilize the receptor in either the open or desensitized state. 2-18F-FA-PET brain imaging cannot determine the current conformational state of unavailable receptors. The timing of nAChR densensitization (decreased response to nicotine exposure) has been studied in cell culture (45), but in vivo molecular imaging methods lack the temporal resolution to distinguish between an nAChR that is densensitized to nicotine and one that is not. Despite this shortcoming, 2-18F-FA-PET brain imaging has established validity for detecting differences in tobacco exposure and for predicting smoking cessation (19,23,26,46). Finally, it should be noted that although increases in cravings to smoke among normal (vs. slow) metabolizers were noted, consistent with faster clearance of nicotine, levels of craving or changes in craving did not correlate with nAChR availability.
CONCLUSION
These results suggest that individual differences in the rates of metabolism of nicotine, based on the NMR, are associated with nAChR availability in smokers shortly after an attempt to quit. Manipulation of nicotine hepatic metabolism could be valuable in improving smoking cessation rates (47,48). This study further reinforces prior evidence that PET imaging of the α4β2* nAChR subtype represents a promising biomarker of nicotine exposure and possibly smoking cessation success. In addition, it raises the underappreciated issue of how psychoactive drug metabolism influences neuronal receptor expression and availability.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported by a grant from the Pharmacogenetics Research Network (PNAT, U01-DA20830), the Abramson Cancer Center at the University of Pennsylvania, the Institute for Translational Medicine and Therapeutics of the Perelman School of Medicine at the University of Pennsylvania (NIH), a McCabe Pilot Award (University of Pennsylvania), and the Commonwealth of Pennsylvania (the Pennsylvania Department of Health disclaims responsibility for analyses, interpretations, or conclusions). Additional support was provided by Pfizer, the National Center for Research Resources, and the National Center for Advancing Translational Sciences, National Institutes of Health (UL1TR000003). Arthur Brody is supported by grants from the National Institute on Drug Abuse (R01 DA20872), the Department of Veterans Affairs Office of Research and Development (CSR&D Merit Review Award I01 CX000412), and the Tobacco-Related Disease Research Program (23XT-0002). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 13, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication February 3, 2015.
- Accepted for publication July 14, 2015.





{kind=link}
{kind=link}