


Abstract
The accurate depiction of both biologic and anatomic profiles of tumors has long been a challenge in PET imaging. An inflammation, which is innate in the carcinogenesis of oral squamous cell carcinoma (OSCC), frequently complicates the image analysis because of the limitations of 18F-FDG and maximum standardized uptake values (SUVmax). New PET parameters, metabolic tumor volume (MTV) and total lesion glycolysis (TLG), as well as 18F-fluoro-α-methyltyrosine (18F-FAMT), a malignancy-specific amino acid–based PET radiotracer, are considered more comprehensive in tumor image analysis. Here, we showed the substantial effects of the intratumoral inflammatory process on 18F-FDG uptake and further study the possibility of MTV and TLG to predict both tumor biology (proliferation activity) and anatomy (pathologic tumor volume). Methods: 18F-FDG and 18F-FAMT PET images from 25 OSCC patients were analyzed. SUVmax on the tumor site was obtained. PET volume computerized-assisted reporting was used to generate a volume of interest to obtain MTV and TLG for 18F-FDG and total lesion retention (TLR) for 18F-FAMT. The whole tumor dissected from surgery was measured and sectioned for pathologic analysis of tumor inflammation grade and Ki-67 labeling index. Results: The high SUVmax of 18F-FDG was related to the high inflammation grade. The SUVmax ratio of 18F-FDG to 18F-FAMT was higher in inflammatory tumors (P < 0.05) whereas the corresponding value in tumors with a low inflammation grade was kept low. All 18F-FAMT parameters were correlated with Ki-67 labeling index (P < 0.01). Pathologic tumor volume predicted from MTV of 18F-FAMT was more accurate (R = 0.90, bias = 3.4 ± 6.42 cm3, 95% confidence interval = 0.77–6.09 cm3) than that of 18F-FDG (R = 0.77, bias = 8.1 ± 11.17 cm3, 95% confidence interval = 3.45–12.67 cm3). Conclusion: 18F-FDG uptake was overestimated by additional uptake related to the intratumoral inflammatory process, whereas 18F-FAMT simply accumulated in tumors according to tumor activity as evaluated by Ki-67 labeling index in OSCC.
A worldwide estimation of newly diagnosed oral cavity cancer in 2008 was more than 250,000, with an estimated mortality number reaching 128,000 (1). Ninety percent of oral cavity cancer is oral squamous cell carcinoma (OSCC) derived from mucosal lining (2), which is directly exposed to the external environment. Despite the advancement of diagnostic imaging and detection of biologic markers, no significant improvement in survival rate was obtained over the past 40 y (3).
OSCC PET imaging using 18F-FDG and maximum standardized uptake value (SUVmax) assessment is helpful for pretreatment staging and improved TNM classification (4,5). Even though it has been considered as an independent prognostic factor (6), the shortcoming of semiquantitative SUVmax is its dependency on a mere single pixel (7), which may not represent the whole tumor entity (8). Moreover, several major limitations of the standardized uptake value (SUV) concept affect its reliability as a surrogate of the targeted quantity, the metabolic rate of 18F-FDG (9).
Because 18F-FDG accumulation in tumor cells depends on glucose metabolism, PET is a sensitive modality for malignancy but lacks the specificity and ability to depict the true tumor biology. To address this, the amino acid–based PET radiotracer 18F-fluoro-α-methyltyrosine (18F-FAMT), which accumulates exclusively in malignant tumor cells through the L-type amino acid transporter 1, was developed (10–12). In previous OSCC studies, 18F-FAMT was better than 18F-FDG in its correlation with tumor proliferation activity, represented by Ki-67 labeling index (Ki-67 LI) (13,14). Moreover, significant false-positive accumulation of 18F-FDG in inflammatory lesions, other nonmalignant lesions, and some normal organs due to physiologic activity contributes to the lower specificity of 18F-FDG for malignancy.
Recently, metabolic tumor volume (MTV) and total lesion glycolysis (TLG), which quantify both anatomic and pathophysiologic aspects of the entire tumor, have been introduced as new evaluation parameters in 18F-FDG PET and used as independent prognostic biomarkers in various solid malignancies (15–17). The addition of these new biomarkers into American Joint Committee on Cancer stage may provide more reliable outcome prediction in oral cancer patients (18).
18F-FAMT discriminates malignant tumors from benign lesions in oral malignancies (14,19). Moreover, in OSCC, 18F-FAMT provides more accurate assessment of bone marrow invasion than 18F-FDG (10). In this study, we investigated how 18F-FDG and 18F-FAMT PET parameters (SUVmax, MTV, and TLG or total lesion retention [TLR]) might be affected by intratumoral inflammatory process through a study with tumor inflammation grade obtained from postsurgical specimen pathologic examination.
MATERIALS AND METHODS
Patients
The study involved 25 OSCC patients (11 men and 14 women; age, 31–88 y; mean age, 61.9 y) who were referred for surgery from April 2008 to March 2013. All patients underwent surgery after 18F-FDG and 18F-FAMT PET/CT imaging. The study protocol was approved by the institutional review board of Gunma University, and all patients who agreed to participate in the study signed a written informed consent form.
Radiopharmaceuticals and PET Image Analysis
18F-FAMT and 18F-FDG were produced in our hospital cyclotron facility. 18F-FAMT was synthesized by the method developed by Tomiyoshi et al. (20). 18F-FDG or 18F-FAMT was administered intravenously at a dose of 5.0 MBq/kg after the patient had fasted for at least 6 h. PET was performed 64.0 ± 12.2 and 66.0 ± 14.0 min after administration for 18F-FDG and 18F-FAMT, respectively, using a PET/CT scanner (Discovery STE; GE Healthcare) with a 700-mm field of view and slice thickness of 3.27 mm. Three-dimensional data acquisition was done for 3 min per bed position, followed by the image reconstruction with the 3-dimensional ordered-subset expectation maximization method. The segmented attenuation correction was performed by CT (140 kV, 120–240 mAs) to produce 128 × 128 matrix images.
All patients underwent 18F-FDG PET imaging first and then continued with 18F-FAMT PET before surgery. One of 3 experienced nuclear medicine physicians (minimum 5 y experience in general nuclear medicine and 4 y in PET/CT) interpreted each PET image of 18F-FAMT and 18F-FDG. The PET images were first examined visually for abnormal 18F-FDG or 18F-FAMT accumulation, and regions of interest covering the whole tumor were placed manually over every axial image plane, to obtain SUVmax for a semiquantitative analysis of tumor uptake.
PET tumor volumes were calculated using PET volume computerized-assisted reporting, an automated segmentation software (Advantage Workstation; GE Healthcare). With a predetermined pathologically confirmed cutoff SUV of 3.0 for 18F-FDG and 1.4 for 18F-FAMT from previous PET study of maxillofacial tumors (19), PET volume computerized-assisted reporting performs autosegmentation to the threshold-defined volumes and automatically calculates MTV and average SUV (10). TLG of 18F-FDG was calculated by multiplying MTV with the average SUV within that volume. A similar formula was used to determine TLR of 18F-FAMT. TLR is defined as a parameter similar to TLG and describes the quantitative amount of 18F-FAMT trapped in tumor cells. For semiquantitative comparison, 18F-FDG–to–18F-FAMT ratios of SUVmax, MTV, and TLG/TLR were calculated.
Tumor Histopathologic Analysis
The surgical specimens were fixed in 10% formalin solution, paraffin-embedded, decalcified when needed overnight, and sectioned (3 μm) for pathologic and immunohistochemical analysis. Pathologic tumor volume (PTV) is measured 3-dimensionally using the length (l), width (w), and thickness (t) by the classic formula (π/6) × l × w × t.
Hematoxylin and eosin (H-E) staining was performed for inflammation analysis. A 4-grade classification of inflammation was used on the basis of the distribution of inflammatory cells within the tumor tissue and its surroundings (Table 1) (21). Tumor with an inflammation grade of 2 and 3 was considered to have a severe inflammation, whereas grade 0 and 1 were similar to normal organs. Immunohistochemical staining was performed using the labeled streptavidin biotinylated antibody method (14). Molecular immunology borstel-1 or MIB-1 (Dako), a murine monoclonal antibody specific for human nuclear antigen Ki-67, was used in a 1:100 dilution.
Tumor Inflammation Grade
Statistical Analysis
Nonparametric tests (Spearman rank test and Mann–Whitney U test) were used to determine the statistical difference of variables. Relationships within variables were measured using Pearson correlation analysis. For both radiotracers’ MTV, further analysis with the Bland–Altman method was used to determine the degree of agreement of the MTVs with PTVs. Probability values of less than 0.05 indicated a statistically significant difference. Results were shown as mean ± SD.
RESULTS
Patients
The average time interval from the last 18F-FDG PET to 18F-FAMT PET was 9.8 ± 10.8 d (range, 2–56 d), and the average time interval from 18F-FAMT PET studies to surgery was 16.7 ± 10.1 d. All patients’ characteristics, their tumor PET quantitative values, tumor volumes, and Ki-67 LIs are summarized in Table 2. Inflammations were found in all patients’ tumors.
Characteristic of Patients and Tumors
Inflammation Involvement in PET Images and Histologic Sections
The high 18F-FDG SUVmax without correspondingly high 18F-FAMT SUVmax is shown on the right lower quadrant of the Pearson correlation graph in Figure 1 (R = 0.53, P = 0.003). This tendency is further described in Figure 2A, in which the 18F-FDG–to–18F-FAMT SUVmax ratio is significantly higher in the grade 2 and 3 group (P = 0.030), showing that high SUVmax of 18F-FDG was significantly correlated with advanced tumor inflammation.

Correlation analysis of SUVmax of 18F-FDG and 18F-FAMT.

18F-FDG–to–18F-FAMT ratio of PET parameters. (A) 18F-FDG–to–18F-FAMT SUVmax ratio is significantly higher on tumor with high inflammation grade. (B and C) PET metabolic parameters (MTV [B] and TLG/TLR [C]) showed that 18F-FDG and 18F-FAMT are similar when uptake is calculated from whole tumor. NS = not significant.
In contrast, the 18F-FDG–to–18F-FAMT ratio of MTV and TLG/TLR showed no difference between inflammation groups (Fig. 2B, P = 0.76; Fig. 2C, P = 0.10, respectively). However, some outliers were observed and suggest more cautious interpretation.
Spearman rank correlation coefficients showed that Ki-67 LI correlated with all PET parameters (Table 3). Even though SUVmax of both radiotracers correlates with Ki-67, in 18F-FAMT, correlation coefficients of MTV and TLR were ρ = 0.718 and 0.748, whereas, in 18F-FDG, correlation coefficients of MTV and TLG were lower, ρ = 0.546 and 0.619, respectively. The SUVmax of 18F-FDG and 18F-FAMT were only moderately correlated with each other (ρ = 0.578), whereas their MTV and TLG/TLR were strongly correlated (ρ = 0.814 and 0.873, respectively).
Spearman Rank Correlation Coefficients for All PET Parameters, Ki-67, and PTV
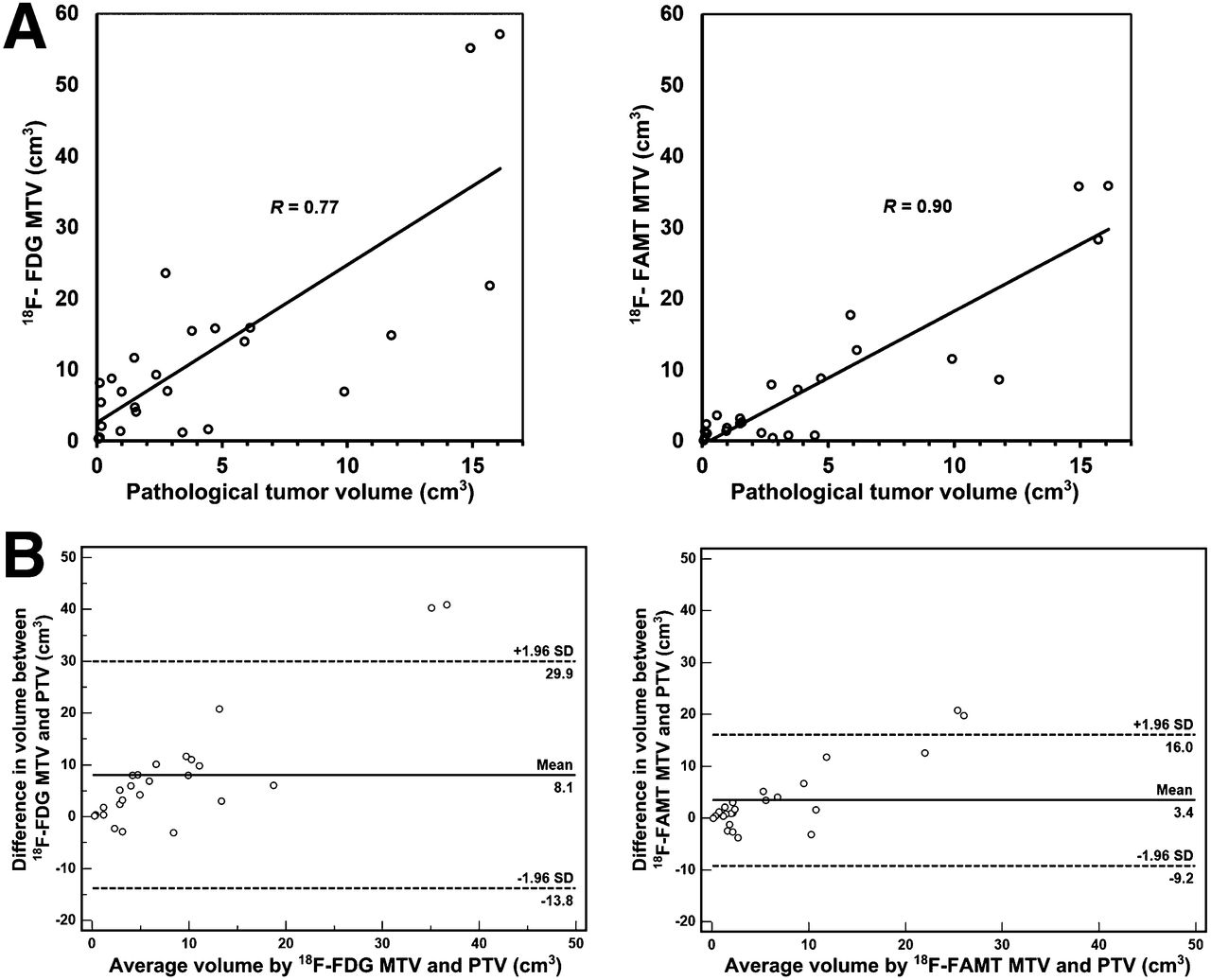
The potentials of MTV to predict the actual tumor volume using of both radiotracers were evaluated by direct comparisons with PTV. MTV values of 18F-FAMT and 18F-FDG provided a good estimation of the actual tumor volume (Fig. 3A, R = 0.77 and 0.90, respectively). Bland–Altman analysis (Fig. 3B) further demonstrated that tumor volumes measured by the MTV of 18F-FAMT showed better agreement with actual tumor volume (bias = 3.4 ± 6.42 cm3, 95% confidence interval = 0.77–6.09 cm3) than that of 18F-FDG MTV (bias = 8.1 ± 11.7 cm3, 95% confidence interval = 3.45–12.67 cm3).
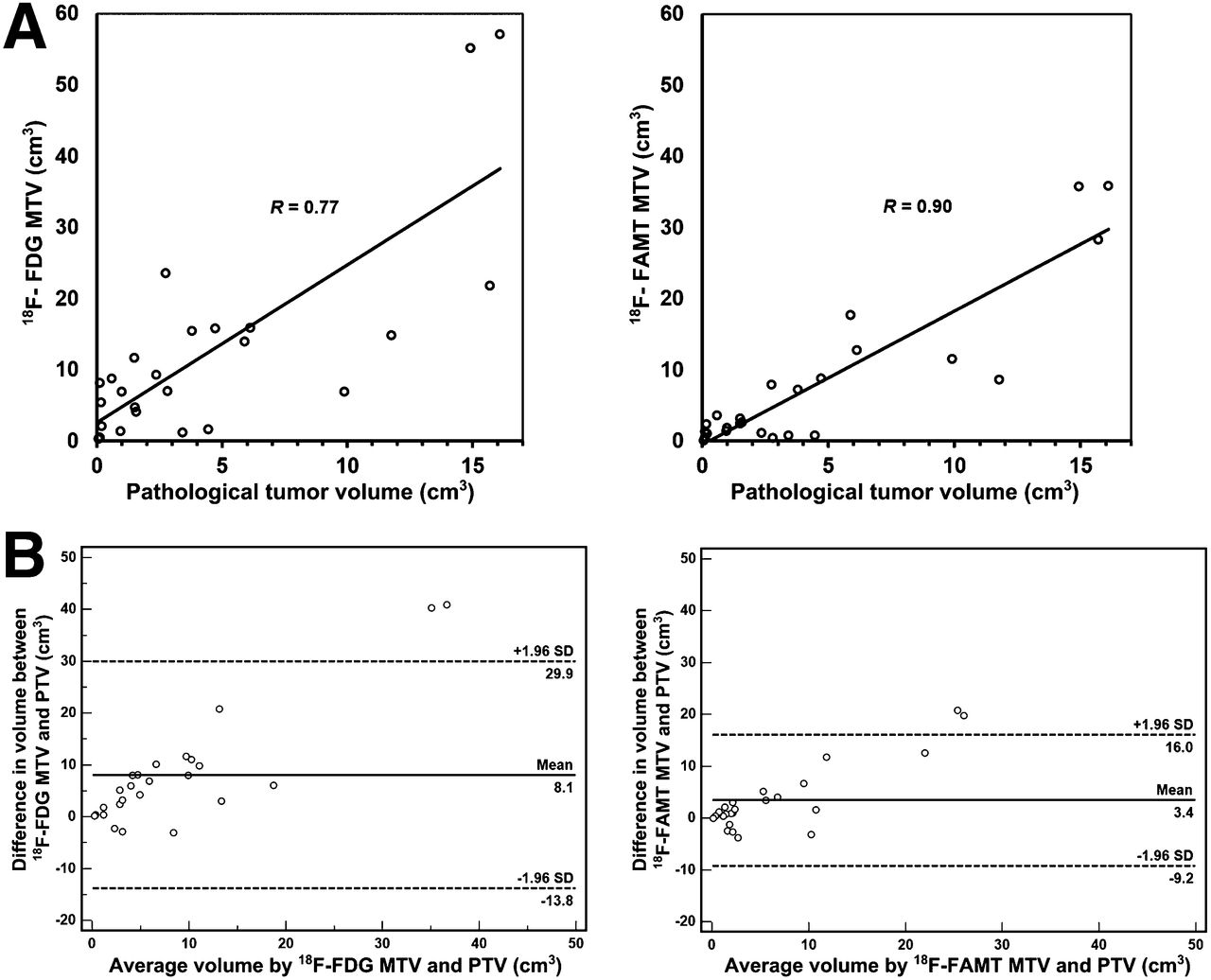
(A) Prediction of actual tumor volume using MTV of 18F-FDG and 18F-FAMT. (B) Bland–Altman analysis. 18F-FAMT MTV predicts tumor size more accurately.
Case Figures
A representative case presented in Figure 4 (patient 20) shows that both 18F-FDG and 18F-FAMT SUVmax parameters demonstrate high uptake. Ki-67 LI from the pathologic specimen was also high (87.6%). However, H-E staining showed that inflammation in this tumor was minimal.

A 40-y-old man with OSCC in right buccal region. (A) Mean-intensity-projection and coronal images of 18F-FDG and 18F-FAMT PET of primary lesion. High 18F-FDG and 18F-FAMT tumor uptake was noted. Concordant high uptake of 18F-FDG (SUVmax = 16.2) and 18F-FAMT (SUVmax = 5.8) was also noted. A high Ki-67 LI value (87.6%) is shown in immunohistochemistry sections (B), and H-E staining showed grade 1 tumor inflammation (C).
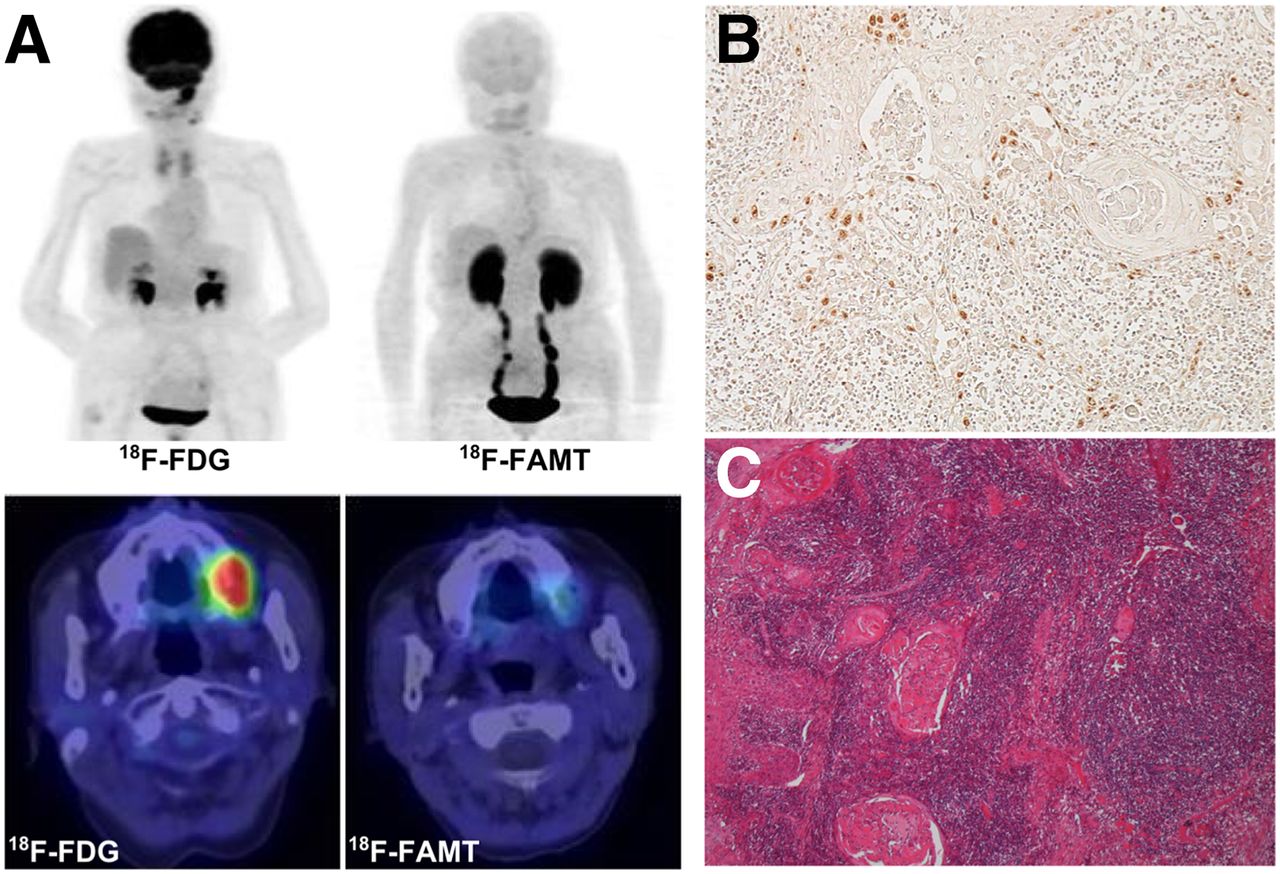
A discordant SUVmax finding between 18F-FDG and 18F-FAMT (patient 2) is presented in Figure 5. In this case, low uptake of 18F-FAMT was suggestive for low tumor activity, as confirmed by a low Ki-67 LI. However, the tumor stage of this patient was advanced due to the presence of neck lymph node metastasis (also confirmed by 18F-FAMT uptake). H-E staining revealed that this tumor had high-grade inflammatory cell infiltration in the invasion area and consisted of mainly neutrophil granulocyte.
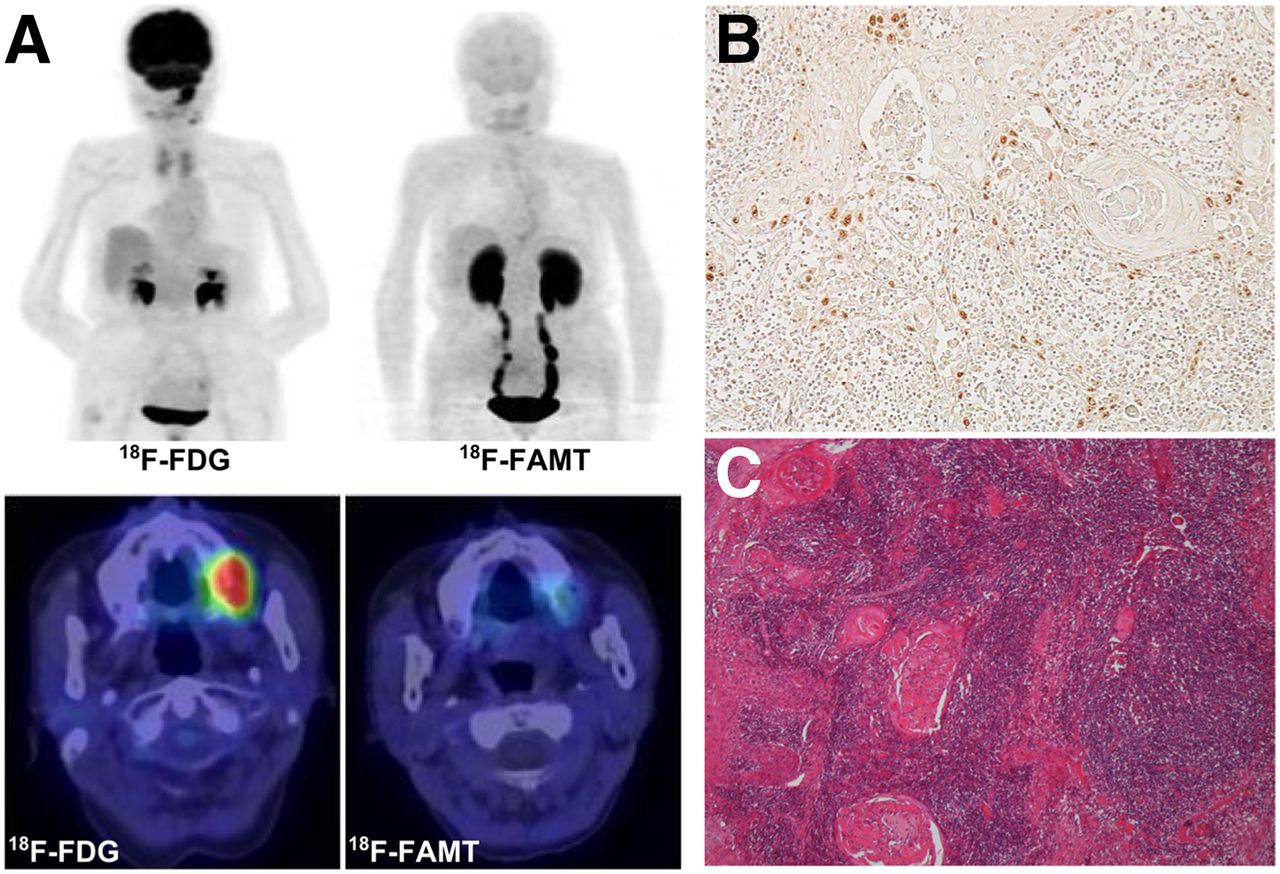
An 88-y-old woman with OSCC in left maxilla region. (A) Mean-intensity-projection and axial images of 18F-FDG and 18F-FAMT PET of primary lesion. High 18F-FDG uptake (SUVmax = 12.2) is noted while on same plane, 18F-FAMT uptake (SUVmax = 1.8) is low. Low tumor proliferation activity is shown by low Ki-67 LI value (39.3%) (B), whereas H-E staining showed grade 3 tumor inflammation (C).
In these 2 patients, all 18F-FAMT parameters corresponded well with Ki-67 staining and PTV. Besides patient 2, 2 other patients (patients 7 and 15) had extremely high 18F-FDG SUVmax without evidence of appropriate PTV, and interestingly their 18F-FAMT parameters matched with their tumor size and proliferation.
DISCUSSION
18F-FDG is the most widely used PET radiotracer for malignancies (22). As a glucose analog, 18F-FDG accumulates in the cells through glucose transporter-1 receptors; these receptors are highly expressed in most malignant cells because of their high metabolic activity. However, active nonmalignant pathologic processes, such as inflammation and infection, may also enhance glycolytic metabolism. Although it has been reported that inflammatory tumors might complicate 18F-FDG PET analysis, this concept has not been validated (23).
We demonstrated that the SUVmax of 18F-FDG and 18F-FAMT were only moderately correlated. Given that 18F-FAMT is more tumor-specific, this finding prompted us to analyze further the inflammation involvement. A significantly higher 18F-FDG–to–18F-FAMT SUVmax ratio in inflammatory tumor strongly suggested that 18F-FDG SUVmax was largely influenced by the intratumoral inflammatory process.
Inflammation is an integral part of the natural course of OSCC carcinogenesis. The highly diverse surfaces in the oral cavity provide a milieu for more than 750 distinct taxa of bacteria. Thus, the oral epithelium is constantly exposed to external challenges at both the cellular and the molecular levels. The evidence suggests that there is a link between microbial infection and OSCC (24).
Tumor cell proliferation rate is reported as a prognostic factor in head and neck carcinomas (25). In oral cavity epidermoid carcinomas, Ki-67 expression serves as an independent prognostic factor for survival (26). However, it is impossible to obtain comprehensive Ki-67 status because of the invasive nature of the biopsy. Thus, developing methods to evaluate cell proliferation activity from PET images would certainly be beneficial (27,28). Regarding the nature of 18F-FDG, such an objective could only be optimally accomplished using a more malignant-specific radiotracer.
The SUVmax of 18F-FDG PET provides prognostic information additional to that provided by the American Joint Committee on Cancer stage (18) and data useful for tumor-aggressiveness evaluation, early detection of recurrence, and outcome prediction in head and neck cancers (16,18). Despite its popularity and practical application, however, SUVmax is derived only from a single pixel, thus it may not represent the whole tumor entity and does not provide any information regarding tumor biology (29,30). Furthermore, SUVmax is highly sensitive to noise and affected by the partial-volume effect (30,31). These phenomena appear particularly in inflammatory lesions; therefore, the evaluation of biologic and anatomic tumor data based only on SUVmax is highly susceptible to bias (30).
Nowadays, advanced image analysis tools and 3-dimensional display techniques allow quick and consistent volume-based assessment. Recently, new 18F-FDG PET parameters (MTV and TLG) have been introduced and showed their potential as an alternative to SUVmax by offering more relevant tumor information while combining both metabolic activity and 3-dimensional tumor volume (15,16). In lung cancer, recently these parameters served as significant prognostic factors for survival and provided better prognostic imaging biomarkers than SUVmax (31). In OSCC, TLG was suspected to be also reliable as an independent prognostic factor for recurrence and metastasis. In head and neck cancer, adding primary tumor TLG into a prognostic scoring system might be useful for risk stratification (15). Together, 18F-FDG MTV and TLG provide such potential in OSCC treated with chemoradiotherapy (32). Moreover, in a recent systematic review, both parameters are accurate prognostic indicators of outcome in head and neck cancer (33).
In this study, we evaluated the potential of 18F-FAMT and these new PET parameters for accurate depiction of both biologic and anatomic profiles of oral tumors. The potential of L-type amino acid transporter 1 as a therapeutic target in oral cancer has been described long before (34,35). We designed 18F-FAMT as a specific PET radiotracer for L-type amino acid transporter 1 that is overexpressed exclusively in malignant tumors (12) and performed several clinical trials in comparison with 18F-FDG in oral malignancies (10,14,19). Therefore, analysis of 18F-FAMT and its corresponding tumor pathologic characteristics is fundamental for the development of a PET imaging–based comprehensive diagnosis of tumor growth.
Previously, we reported that SUVmax of 18F-FAMT PET images showed better correlation with Ki-67 expression and clinicopathologic variables than 18F-FDG in the primary tumor of OSCC (14). Our current study elaborated this finding by introducing new parameters in the evaluation of both PET radiotracers. Consistent with the previous report, all 18F-FAMT parameters surpassed those of 18F-FDG in providing better correlation with cell proliferation activity. In particular, the MTV and TLR of 18F-FAMT showed their potential as an SUVmax replacement, because they have a stronger correlation with cell proliferation activity, compared with SUVmax. Such findings were not observed in 18F-FDG, for which both new parameters correlated less well with Ki-67, showing that 18F-FAMT is superior to 18F-FDG in its accuracy to predict tumor cell growth in OSCC.
The correlation between 18F-FAMT’s new parameters and Ki-67 in this study revealed the potential of 18F-FAMT for use as a predictor of tumor cell growth in OSCC. The specificity of 18F-FAMT for malignant and highly proliferating tumors is shown in Figure 4 (patient 20); the SUVmax for both 18F-FDG and 18F-FAMT corresponded well to the radiotracer’s high expression of tumor Ki-67. As shown in Figure 5 (patient 2), the expression of Ki-67 correlated well with 18F-FAMT uptake, whereas 18F-FDG showed a high uptake suggestive of a false-positive result caused by inflammation or nonspecific uptake, which is prone to overestimation.
If we may further hypothesize by taking into account the well-established correlation between Ki-67 and patients’ survival, our findings suggest that 18F-FAMT and its new parameters might provide immediate predictions of patients’ survival, through the estimation of tumor cell proliferation. This relationship is currently under evaluation.
This study is limited by the use of pathologically confirmed fixed SUV cutoff values for the segmentation threshold, which is exclusive for OSCC. Gradient-based segmentation might be a better method for other tumors than the fixed-threshold method; however, similar results were not observed in head and neck cancers (18,36). Finally, this was a retrospective single-center study, thus the results might be subject to selection bias. In general, further investigations are needed to elucidate the effects of the intratumoral inflammatory process on 18F-FDG uptake in other types of tumors.
CONCLUSION
18F-FDG uptake was overestimated by additional uptake related to the intratumoral inflammatory process, whereas 18F-FAMT simply accumulated in tumors according to tumor activity as evaluated by Ki-67 LI.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 4, 2014.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication November 3, 2014.
- Accepted for publication November 4, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}