


Abstract
Historically, it has been difficult to monitor the acute impact of anticancer therapies on hematopoietic organs on a whole-body scale. Deeper understanding of the effect of treatments on bone marrow would be of great potential value in the rational design of intensive treatment regimens. 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) is a functional radiotracer used to study cellular proliferation. It is trapped in cells in proportion to thymidine-kinase 1 enzyme expression, which is upregulated during DNA synthesis. This study investigates the potential of 18F-FLT to monitor acute effects of chemotherapy on cellular proliferation and its recovery in bone marrow, spleen, and liver during treatment with 2 different chemotherapy regimens. Methods: Sixty patients with non–small cell lung cancer underwent concurrent radical chemoradiotherapy to 60 Gy in 6 wk with either cisplatin/etoposide (C/E, n = 28) weeks 1 and 5 or weekly carboplatin/paclitaxel (C/P, n = 32) regimens. 18F-FLT and 18F-FDG PET with CT were performed at baseline, week 2 (day 9 for 18F-FLT and day 10 for 18F-FDG PET), and week 4 (day 23 for 18F-FLT and day 24 for 18F-FDG PET). Visual and semiquantitative standardized uptake value (SUV) measurements were performed in bone marrow outside the radiotherapy field, liver, spleen, and small bowel. These were correlated to blood counts and smears in a subset of patients. Results: The C/E group exhibited a drop in bone marrow 18F-FLT uptake at week 2 (median SUVmax [maximum SUV] decrease to 31%, 8.7–6.0, P < 0.001), with recovery at week 4, reflecting the absence of chemotherapy between these times. By contrast, the weekly C/P group showed gradually declining bone marrow uptake (P > 0.05). Spleen uptake in both cohorts decreased at week 2, with intense rebound activity at week 4 (SUVmax week 4 at 58% above baseline: 2.4–3.8, for C/E, respectively, 30% for C/P: 2.7–3.5, P < 0.001). Liver uptake changed little. 18F-FLT changes preceded neutrophil count reductions. 18F-FDG uptake in marrow liver and spleen changed much less than 18F-FLT. Conclusion: 18F-FLT imaging may be used to quantify impairment and recovery of bone marrow by specific chemotherapy regimens and may also enable imaging of organ-specific processes such as spleen activation. 18F-FLT is superior to 18F-FDG for this purpose. This technology may support novel treatment planning and monitoring approaches in oncology patients.
Functional tracers with whole-body imaging capability constitute the centerpiece of oncologic molecular imaging. A wide field of view facilitates a holistic assessment of disease processes and organ function in the human body because it shows organs and systems beyond the primary lesion. Molecular imaging therefore offers a clinical counterpart to systems-based approaches in fundamental research (1).
Use of combined PET and CT, with the radiotracer 18F-FDG, has significantly enhanced the management of patients with non–small cell lung cancer (NSCLC), including the areas of diagnosis, staging, target delineation for radiation therapy (RT), and therapeutic response monitoring (2).
18F-FDG is a well-known PET/CT tracer for the imaging of glucose metabolism pathways within tumors, but it also demonstrates variable uptake in the bone marrow. For example, 18F-FDG uptake is increased in Hodgkin disease in relation to tumor-secreted cytokines (3,4), and rebound uptake in the bone marrow has also been well described after cytotoxic chemotherapy (5). However, it is unclear to what extent these changes reflect marrow proliferation because 18F-FDG uptake is multifactorial. In contrast to this, 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) is a recent functional tracer more directly linked to proliferation. The trapping of 18F-FLT in cells is related to the activity and regulation of the cytosol-based thymidine-kinase-1 enzyme (TK1) (6). TK1 is upregulated during DNA synthesis. The relationship between this tracer and the cellular cycle and hence, indirectly, the proliferative activity is well-documented (7).
Monitoring the impact of chemotherapy on the hematopoietic system is critical in medical oncology, given the significance of adverse effects induced by immunosuppression and thrombocytopenia (8). The overall toxicity of well-established regimens is thoroughly documented, although dosage schemes and adaptation to parameters such as body surface or renal function remain largely empiric. There are few tools that can offer insights into the toxicity of new therapy regimens or new drugs. Molecular imaging has a role to play and could provide some of the technologies needed to answer these questions and develop personalized chemotherapy schemes. In particular, the time taken for recovery in marrow proliferative function may have important implications for scheduling of chemotherapy.
There have been several recent papers reporting the utility of 18F-FLT PET/CT in monitoring hematopoietic organs, such as bone marrow and the spleen, in chronic myeloproliferative disorders or within radiotherapy fields (9–12), but we are unaware of any reports of time-dependent distribution patterns of 18F-FLT uptake in organs affected by cytotoxic chemotherapy regimens during treatment. A prospective trial of serial 18F-FLT and 18F-FDG PET/CT for monitoring disease response to radical chemoradiotherapy (chemo-RT) in patients with NSCLC is currently ongoing at our center (Registry no. ACTRN12611001283965). In this trial, patients are treated with 1 of 2 chemotherapy regimens (cisplatin/etoposide [C/E] or carboplatin/paclitaxel [C/P]), which have different and well-documented toxicities (8). Data from our study therefore presented a unique opportunity to explore these topics further.
Specifically, we hypothesized that distinct radiotracer patterns would be identifiable in response to different chemotherapy regimens. We paid particular attention to the behavior of the bone marrow and spleen, given the renewed interest in the latter in oncology (13,14). We interrogated the stability of hepatic uptake, critical for qualitative imaging, because the liver has a potential hematopoietic role that may translate as variation of uptake during chemotherapy (15). We further investigated the interrelation between 18F-FLT and 18F-FDG in these organs and the potential for 18F-FLT uptake to anticipate the classic toxicity endpoint of peripheral blood counts and blood smears.
MATERIALS AND METHODS
Patients
Patients with stage I–IIIB NSCLC considered by our multidisciplinary tumor board to be suitable candidates for radical chemo-RT were recruited. Patients with previous thoracic RT or complete macroscopic tumor excision were excluded. Our Institutional Ethics Committee approved the trial, and patients provided written, informed consent.
Chemo-RT
Treatment planning included conformal RT (60 Gy/30 fractions, 6 wk) with concomitant C/E: cisplatin (50 mg/m2) on days 1 and 8 (cycle 1) and 29 and 36 (cycle 2) and etoposide (50 mg/m2 daily during cycles 1 and 2—that is, respectively, weeks 1 and 5), or weekly C/P: carboplatin (area under the curve, 2) and paclitaxel (45 mg/m2). Dexamethasone was administered intravenously: 20 mg (C/P) and 12 mg (C/E). Chemotherapy doses were adapted to baseline renal function (electronic glomerular filtration rate). Full blood counts were recorded at baseline and at least before each chemotherapy cycle. Prospective blood sampling with full blood counts and blood smears on the day of each 18F-FLT PET/CT study was performed in the last 21 patients. Blood smears were scanned on a ScanScope XT slide scanner (20×) (Aperio). Counting of neutrophils, lymphocytes, and monocytes was performed on eight 10× fields with the ImageScope software (Leica Biosystems).
PET/CT Imaging
Imaging was performed at baseline, week 2 (day 9 for 18F-FLT and day 10 for 18F-FDG, after 14 Gy ± 2 Gy), and week 4 (day 23 for 18F-FLT and day 24 for FDG, after 38 Gy ± 4 Gy) of chemo-RT. Scans were acquired on an integrated PET/CT (STE [GE Healthcare] or Biograph [Siemens Medical Solutions]). Patients were weighed and intravenously injected with either 3.7 MBq of 18F-FLT per kilogram or 4.2 MBq of 18F-FDG per kilogram. Patients fasted for at least 6 h before 18F-FDG and rested for at least 1 h before scanning. Patient positioning followed our previously reported method (16). Baseline emission scans were initiated 60 min after injection, and all subsequent scans were scheduled according to the baseline uptake time. Baseline 18F-FLT scans were obtained from vertex to thighs, and baseline 18F-FDG scans were obtained from the base of the brain to thighs. Subsequent scans were limited from the thoracic inlet to the mid abdomen to reduce radiation exposure from the CT component by Institutional Ethics Committee request. Approval for 18F-FLT was granted by the Australian Therapeutic Goods Administration (Cyclotek, Bundoora, Victoria, Australia).
Image Analysis
Visual assessment of the effective radiotherapy field was evaluated on 18F-FLT scans. The uptake of the spinal bone marrow, spleen, and liver outside the radiation field was compared with the previous scan as increased, stable, or decreased by a reviewer masked to clinical data and chemotherapy regimen. For this purpose, the window width was set from a standardized uptake value (SUV) of 0–9 in all scans.
For all scans, measurements with 3-dimensional volumes of interest (VOIs) were then performed. For the bone marrow, the center of a vertebral body 2 or more vertebral levels below the visible effect of the RT field was selected (9), and mean SUV (SUVmean) was measured with a 3-mL cube VOI with an isocontour 30% maximum SUV (SUVmax). Vertebral bodies with discordant uptake in comparison with the adjacent vertebrae or with significant morphologic abnormality such as marked degenerative changes or compression fracture were excluded. For a patient, the same vertebral body was measured in all scans. Spleen and liver uptake was measured with a single VOI centered on the organ, allowing for misregistration and avoiding the superior aspect of the organ potentially prone to direct radiation impact. SUVmax, SUVmean, and VOIs and percentage injected dose for the spleen were recorded. For small bowel (jejunum), only 18F-FLT SUVmax was recorded because of peristaltic movement between PET and CT acquisitions. VOIs were placed at least 6 slices (>2 cm) from the limit of the field of view.
Measurements were performed on an Advantage Windows4.0 workstation (GE Healthcare) except for the small bowel, which was measured with Osirix3.9.4 (Osirix Medical Software).
Statistics
Statistical analyses were performed with Prism4.0 (GraphPad Software). Interpatient variations were considered nonnormal, and variations between time points were compared using Wilcoxon matched-pairs with 95% confidence interval statistical tests. Two-tailed tests were to evaluate increase or decrease in uptake and reduce type I statistical errors. Consistency of imaging charters was verified by Bland–Altman analyses (17).
RESULTS
Patients and PET/CT Scans
Sixty-seven patients were recruited between March 2009 and June 2013 (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org). Seven patients were excluded after multidisciplinary review of disease burden or withdrew consent before baseline. Sixty patients were retained, 37% (22/60) women, 63% (38/60) men; median age was 67 y in both groups (age range, 31–78 and 54–86 y, respectively). Tumor histology was adenocarcinoma in 45% (27/60), squamous cell carcinoma in 37% (22/60), large cell carcinoma in 8% (5/60), nonspecified in 7% (4/60), and neuroendocrine component in 3% (2/60). Most patients had stage III disease, and radiotherapy included the primary tumor and involved mediastinal and hilar lymph nodes. Bone marrow in the thoracic spine, ribs, and scapulae received direct or scattered radiation from radiotherapy.
Twenty-eight patients (47%) received the cisplatin/etoposide regimen and 32 (53%) a carboplatin-based regimen. Six patients did not complete the study because of disease progression and switched to palliative treatment. One hundred sixty-two and 169 PET/CT studies with 18F-FLT and 18F-FDG, respectively, were performed; 2 patients missed 18F-FLT baseline, and five 18F-FLT scans were cancelled for tracer unavailability. On average, 18F-FLT uptake time was 72 min (range, 55–118 min, 9 scans > 90 min). Mean interval between baseline uptake time and other time points was 2.2 min (range, −17 to +32 min, >15 min of difference from baseline in 7 scans). Similar values were observed for 18F-FDG scans (data not shown). Compliance of the 18F-FLT and 18F-FDG imaging charters was verified (17).
Comparison of 18F-FLT Patterns in Bone Marrow with Each Chemotherapy Regimen
Visual assessment of images between baseline and week 2 noted decreased uptake in 72% (18/25), stable uptake in 20% (5/25), and increased uptake in 8% (2/25) of the patients of the C/E cohort (Fig. 1A). For the C/P cohort, 43% (13/30) were decreased, 23% (7/30) stable, and 33% (10/30) increased (Fig. 1C). These results were also reflected by VOI analysis. 18F-FLT uptake outside the radiotherapy field significantly reduced in the C/E cohort, compared with baseline, with a median fall at week 2 of 31% (8.7/6.0, P < 0.001) but recovery by week 4 (42% increase from week 2, 6.0/8.6, P < 0.001) (Fig. 1B). This result probably reflects the C/E patients not receiving chemotherapy between weeks 2 and 4. However, the temporal pattern of changes in the C/P cohort differed with a nonsignificant fall from baseline to week 2 of 10% (9.1/8.2) and a continuing decreasing trend at week 4 (both P > 0.05) (Fig. 1D). SUVmean measurements showed similar results (data not shown).

(A) Bone marrow 18F-FLT uptake decreases at week 2 (black arrow) and returns to baseline (white arrow) after week 2 to week 4 chemotherapy break in the C/E group; representative maximum-intensity-projection images from closest-to-median bone marrow SUVmax C/E patient. (B) SUVmax for C/E group. (C) Bone marrow uptake is nonsignificantly decreasing in C/P group; representative images from closest-to-median bone marrow SUVmax C/P patient. (D) SUVmax for each C/P patient. Black lines = median SUVmax; NS = nonsignificant. **P < 0.01. ***P < 0.001.
Recovery of 18F-FLT Uptake in Spleen
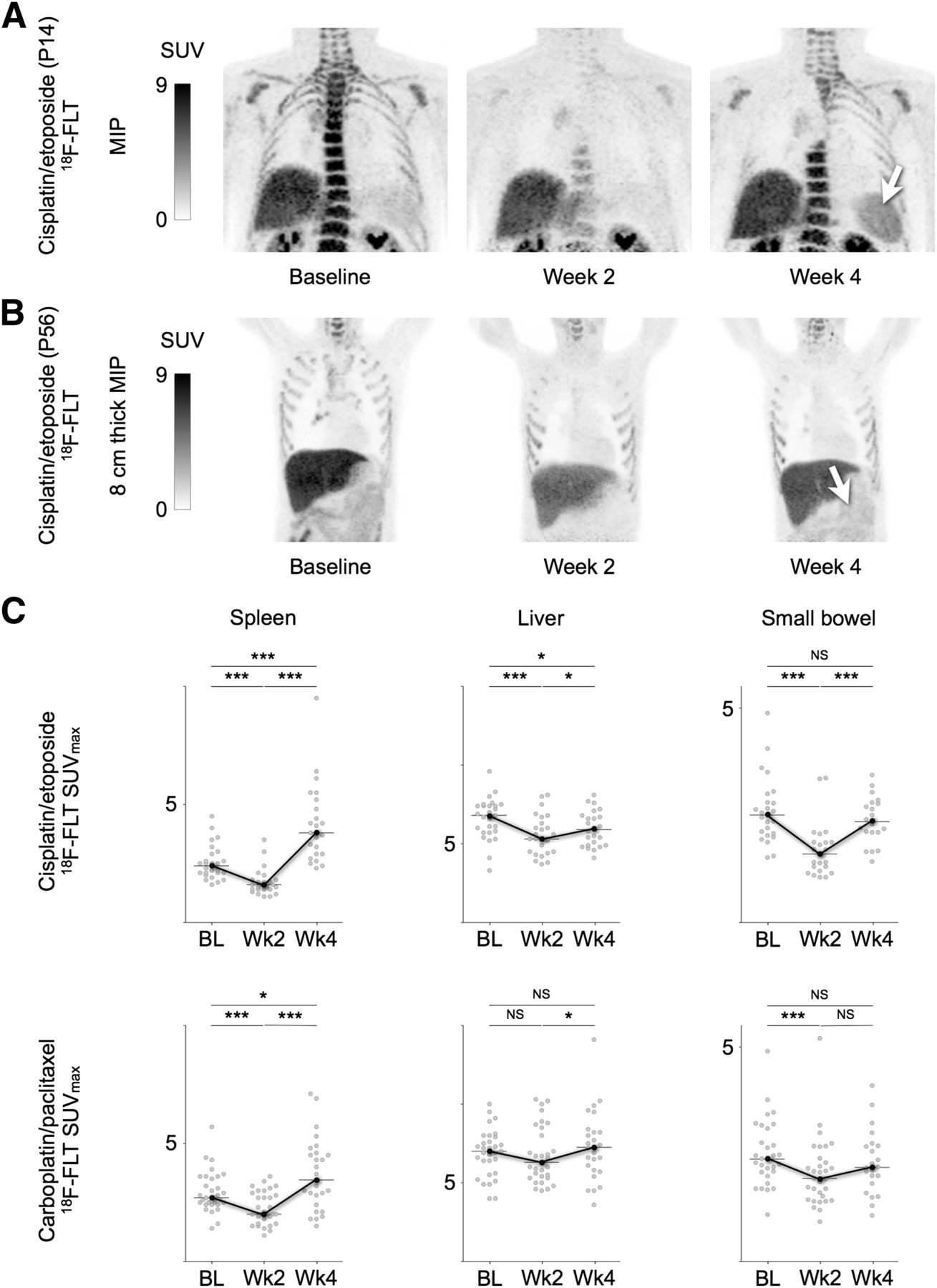
Qualitative changes in splenic uptake were also apparent during treatment. In particular, splenic uptake tended to fall at week 2 and then increase at week 4 in the C/E cohort; these changes were less apparent in the C/P cohort (Figs. 2A and 2B). Semiquantitative analysis supported this. In the C/E group, 18F-FLT uptake in the spleen decreased from baseline to week 2 by 33% (2.4/1.6, P < 0.001) but by week 4 had increased, compared with baseline by 58% (2.4/3.8, P < 0.001) and compared with week 2 by 138% (1.6/3.8, P < 0.001) (Fig. 2C). Similarly, in the C/P patients, splenic uptake had also fallen by week 2, with a reduction in SUVmax of 26% (2.7/2.0, P < 0.001), followed by an increase at week 4 by 30%, compared with baseline (2.7/3.5, P < 0.001), and 75% (2.0/3.5, P < 0.001), compared with week 2. We verified that there was no significant difference between the patients who had radiation to the left lower lung field and the others (data not shown).
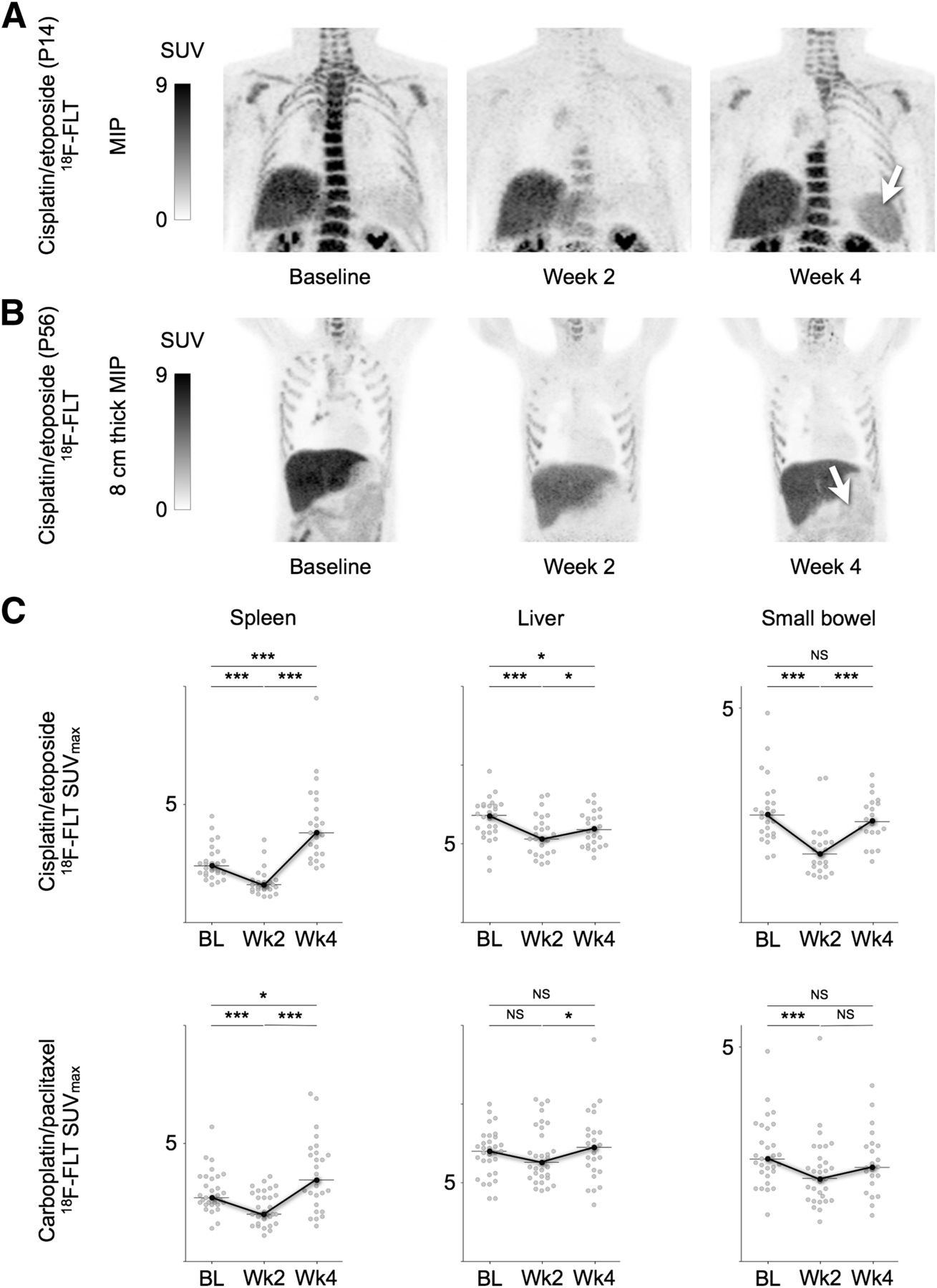
(A) 18F-FLT uptake in spleen demonstrates significant decrease at week 2 and recovery at week 4, particularly intense for C/E cohort; representative maximum-intensity-projection images from closest-to-median spleen SUVmax C/E patient show intense splenic activation at week 4 (white arrow). (B) Representative 8-cm-thickness maximum-intensity-projection image of another C/E patient demonstrates small bowel recovery at week 4 (white arrow). (C) SUVmax for each C/E patient; liver and small bowel changes are less prominent but consistent with bone marrow and spleen findings. Black lines = median SUVmax; NS = nonsignificant. *P < 0.05. ***P < 0.001.
Liver as Reference Organ for 18F-FLT Imaging
Qualitatively, liver uptake did seem to decrease during both forms of chemotherapy. This fall was significant in the C/E cohort, with a median 18F-FLT SUVmax decrease of 22% from baseline (6.8/5.3, P < 0.01), but the fall of 10% (7.0/6.3) in the C/P group was not statistically significant (Figs. 2A–2C). The recovery in hepatic uptake between week 2 and week 4 was significant in both patient groups (P < 0.05), although the uptake at week 4 remained significantly below baseline in the C/E patients (P < 0.05).
Small Bowel 18F-FLT Uptake
The mucosa of the small bowel is known to be sensitive to chemotherapy (18). For both chemotherapy cohorts, a significant decrease at week 2 (C/E: −32%, 2.5/1.7, P < 0.001; and C/P: −21%, 2.4/1.9, P < 0.001) and a significant increase from week 2 to week 4 in the C/E cohort only (C/E: +35%, 1.7/2.3, P < 0.001; and C/P: +16%, 1.9/2.2, P > 0.05) was demonstrated in the small bowel (Figs. 2A and 2C).
18F-FLT Changes as Predictor of Decline of Peripheral Neutrophil Count
We prospectively sampled the blood of the last 21 patients recruited (n = 10 C/E and 11 C/P) at the time of 18F-FLT PET/CT. Daily chemotherapy for 8 d in the C/E cohort induced a more rapid decrease in peripheral blood counts than the 2 d of chemotherapy during the same interval in the C/P cohort (Supplemental Fig. 1). We verified that neutrophil counts did not decrease at week 2 but did at week 4, whereas lymphocyte and monocyte counts dropped markedly at week 2 (P < 0.05 in C/E and C/P groups) (Fig. 3). No recovery of lymphocyte counts was observed by week 4, which was confirmed by evaluating blood smears (Supplemental Fig. 2). Significant recovery of monocyte counts was observed in the C/E group (P < 0.05) whereas only a nonsignificant increase was noted in the C/P group (Fig. 3). We demonstrated no significant correlation between the intensity of 18F-FLT uptake in the organs and peripheral white blood cell counts (data not shown). Of note, patient P01 had the highest baseline bone marrow uptake and highest neutrophil counts (18F-FLT SUVmax, 16.8; neutrophils, 33.5 × 109/L).
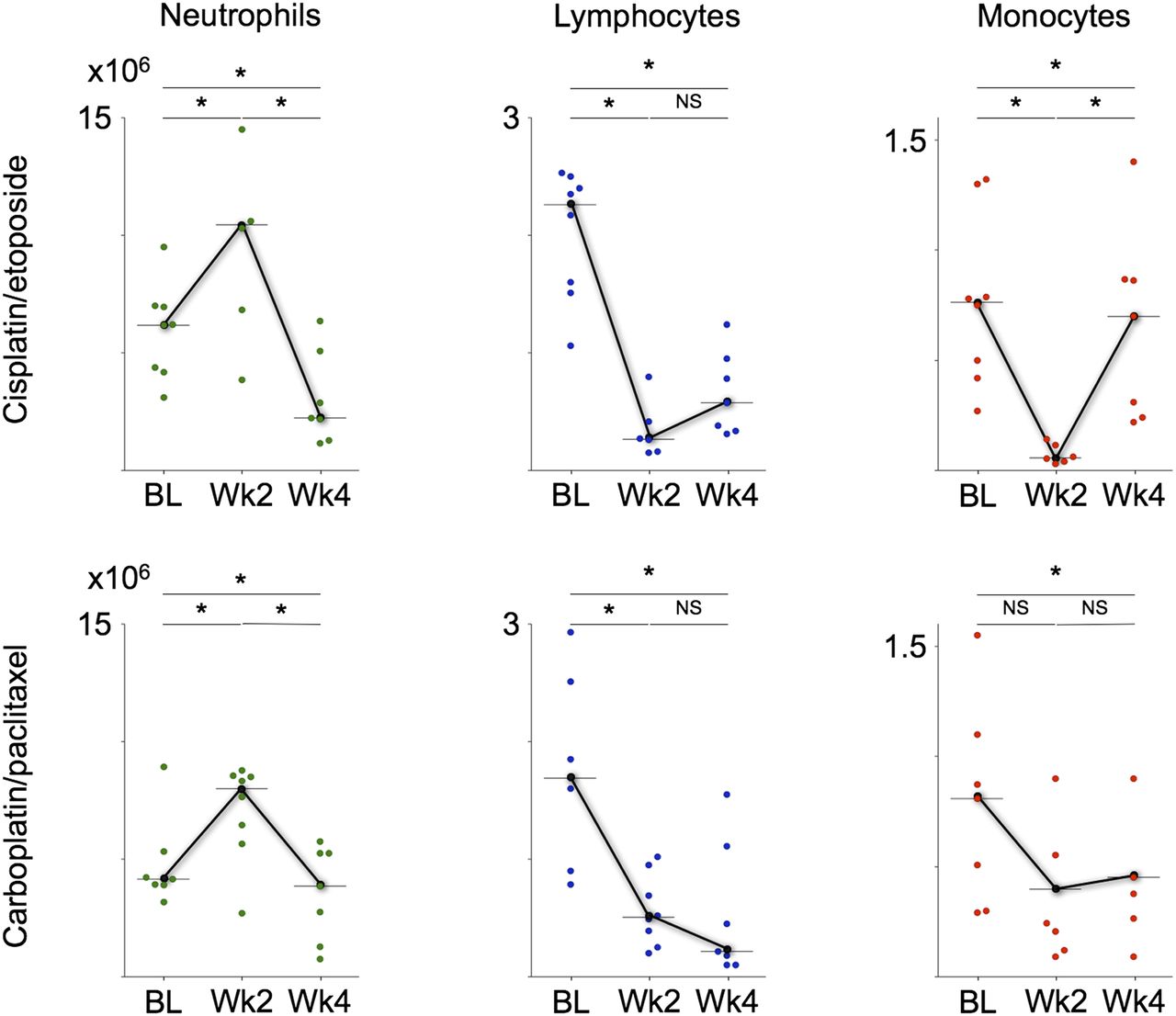
Prospective blood collection at time of each 18F-FLT PET/CT study demonstrates in both chemotherapy regimens that neutrophils did slightly increase at week 2, at which time C/E patients’ bone marrow uptake had decreased. Lymphocytes and monocytes followed change of 18F-FLT between baseline and week 2, but only monocytes in C/E group showed significant recovery. BL = baseline; NS = nonsignificant. *P < 0.05.
18F-FLT Changes and Glucose Metabolism
Significant variations of 18F-FDG SUVmax uptake were recorded in the bone marrow and spleen of both patient groups between baseline and week 2 and between week 2 and week 4 in the C/E group only. The variation of median SUVmax was less marked than for 18F-FLT, with a reduction of 15% (2.6/2.2) for bone marrow and 9% (2.4/2.2) for spleen between baseline and week 2 (Supplemental Figs. 3A and 3B). Uptake at week 4 was not significantly different from baseline in either cohort. Finally, median SUVmax was approximately 3-fold higher in the bone marrow and 2-fold higher in the liver on 18F-FLT scans 18F-FDG scans.
DISCUSSION
Of the approximately 400 studies involving 18F-FLT PET/CT indexed in PubMed, fewer than 5% focus on bone marrow or hematopoiesis. Most studies describe a dramatic drop in 18F-FLT uptake in irradiated bone marrow (9,10,19). Others have described the relation between 18F-FLT uptake in bone marrow and chronic myeloproliferative disorders (11) or describe the distribution of proliferative bone marrow in cancer patients (20–22). A relevant study in rats demonstrated bone marrow recovery monitored by 18F-FLT after bone marrow transplantation (23). In our study, we demonstrated the capability of 18F-FLT imaging to monitor chemotherapy injury to hematopoietic organs and to the small bowel mucosa. The findings demonstrate that rapid changes in 18F-FLT uptake occur in relation to the expression of TK1. The lack of direct correlation with blood counts, however, suggests that the uptake of 18F-FLT in marrow may be more complex than simply reflecting global proliferation.
A limitation in studying the relationship between 18F-FLT uptake in hematopoietic organs and chemotherapy in patients is that serial biopsies are neither practical nor likely to be acceptable to patients. Furthermore, peripheral blood counts do not allow the separation of the contribution of different organs to hematopoiesis or their relative contribution to the composition of whole blood with respect to the different cellular lineages. To circumvent this limitation, we based our analysis on 2 subgroups of chemotherapy regimens. The difference in administration schedule, with cisplatin/etoposide delivered in a dose-intense daily infusion for a week with more than 2 wk of recovery, compared with the fractionated infusion of carboplatin/paclitaxel once a week, seems to have been the main determinant of differences in early 18F-FLT biodistribution changes. We further cross-correlated 18F-FLT uptake variation with variation of uptake in the small bowel, because sensitivity to platin-based chemotherapy and in particular decrease in tyrosine kinase activity in the small bowel crypts has been known for more than 2 decades in animals (18). The combination of these 2 approaches allowed us to provide evidence of the relevance of using 18F-FLT as a likely surrogate of cell-cycle arrest and reactivation during chemotherapy.
All patients were treated according to standard radiotherapy dose and fractionation, indicating that differences between the 2 groups were not dependent on radiotherapy effects. The increase of 18F-FLT uptake measurements between week 2 and week 4 of the C/E regimen, despite ongoing radiotherapy, is consistent with this hypothesis. The significant impact of radiation on thoracic bone marrow is documented. This impact may have induced complex effects, potentially decoupling peripheral blood counts from 18F-FLT uptake patterns.
Although we investigated acute changes in blood counts, toxicity effects at or beyond the completion of the treatment are not addressed by our study. In NSCLC during radical chemo-RT, however, oesophagitis and pneumonitis are usually the most significant acute side effects after completion of therapy (24–26).
Bone marrow 18F-FLT uptake recovery was accompanied by an even more striking recovery in the spleen. The spleen is known to progressively expand in chronic myeloproliferative disorders, with concomitant intense 18F-FLT uptake (11,27,28). This organ has been rediscovered in recent years for its role in acute nontraumatic insults. These studies in small-animal models of lung carcinoma and in myocardial infarction have demonstrated the role of the spleen as a reservoir for the expansion of bone marrow–derived cells and as a supply source for monocytes relocating to the tumor or the infarction site (29,30). A small-animal study has also demonstrated the impact of splenectomy in blood counts recovery early after chemotherapy (31). Interestingly in our study, marked recovery occurs in splenic 18F-FLT uptake of C/E patients who also show synchronous recovery of circulating monocytes. This work confirmed a specific behavior of the spleen in the setting of acute hematologic toxicity. We further demonstrated that changes in 18F-FLT uptake, with its marked drop in the bone marrow of C/E patients at week 2, occurred before the fall in peripheral neutrophil counts. This drop indicates a potential for 18F-FLT as an imaging surrogate marker of clinically relevant toxicity, similarly to work that indicated peripheral lymphocyte and monocyte counts as predictors of neutropenic events (32,33).
We further demonstrated that the liver showed minimal but significant variation of uptake in the C/E regimen both with 18F-FLT and with 18F-FDG tracers. This variation should be accounted for when using this organ as a reference in the visual comparison of iterative studies. However, it is reassuring to note that this would not lead to false-positive response to therapy assessments. Liver uptake did not increase during chemotherapy even with 18F-FLT, when decreased uptake in other organs led theoretically to increased availability of 18F-FLT for hepatic glucuronidation. The reliability of the liver as a reference organ in iterative imaging is of prime clinical importance: for example, in lymphomas, in which the value of interim 18F-FDG scans to assess early response to therapy is the subject of several clinical trials (34).
CONCLUSION
This study suggests that 18F-FLT PET/CT may provide novel insights into acute changes in susceptible organs involved in hematopoiesis. This systems-based approach represents a step toward the study of the individual role of the bone marrow, spleen, and possibly liver in hematologic toxicity. 18F-FLT appears to be a useful tool to monitor these phenomena and could potentially support the development of new and, ideally, personalized chemotherapy regimens in the future.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This study is supported by the SICPA Foundation, The CASS Foundation, and NHMRC grant APP1003895. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We kindly thank Prof. Tomas Kron and Marnie Collins for their expertise and Lisa Macfarlane, Mira Liu, and Jenny Trinh for their efficient coordination.
Footnotes
Published online May 27, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 26, 2013.
- Accepted for publication March 7, 2014.





{kind=link}
{kind=link}
{kind=link}