


Abstract
Neurodegenerative diseases are characterized by progressive dysfunction and neuronal death, showing specific protein inclusions at autopsy. In vivo detection of these key proteins, namely amyloid-β, tau, α-synuclein, and trans-active response DNA-binding protein 43 kDa, is possible by means of molecular neuroimaging techniques, such as PET. The development of selective PET radiotracers targeting these proteins is critical for early and accurate diagnosis and for the successful development of disease-modifying therapies. Selective PET radiotracers for amyloid-β are already available, and potential tau tracers are emerging as new-generation biomarkers. An overview of the tau-PET radiotracer development scenario, focusing on tracers that are presently being examined in humans, is presented.
Tubulin-associated unit, or tau, is an intracellular protein playing a vital role by binding to and stabilizing axonal microtubules in neurons, thereby regulating intracellular transport. The microtubule-binding region of tau consists of 3 or 4 tandem repeats via which tau mediates additional functions (1). Disease-associated posttranslational modifications, such as hyperphosphorylation, cause tau to dissociate from microtubules and assemble into large fibrils, referred to as paired helical filaments. The normal functions of tau are thus altered. The paired helical filaments and similar tau filaments, in turn, associate to form neurofibrillary tangles, which are the pathologic hallmark of various neurodegenerative diseases. tau aggregates or inclusions depict different diseases depending on the structural basis of the aberration. For instance, accumulations of the 3 tandem repeats are typical of Pick disease and the 4 tandem repeats are characteristic of corticobasal degeneration, progressive supranuclear palsy, and argyrophilic dementias, whereas Alzheimer disease (AD) often presents a mixture of 3 and 4 tandem repeats. Thus, in ways presently not understood, structural differences within the tau protein lead to distinct histopathology and disease phenotypes (1).
CLINICAL RELEVANCE OF TAU PET IMAGING
Diseases characterized by the presence of pathologic tau, such as dementias and movement disorders as well as traumatic brain injury and chronic traumatic encephalopathy, could potentially benefit from tau PET imaging. The severity of tau pathology is closely related to neuronal loss and cognitive impairment in AD (2), supporting the use of tau as a biomarker of neurodegeneration. Tau, amyloid-β (Aβ), α-synuclein, and trans-active response DNA-binding protein 43 kDa (TDP-43) may coexist in different relative concentrations depending on the disease (e.g., Aβ predominance in AD; α-synuclein in dementia with Lewy bodies), its stage (higher concentrations in advanced disease), and its cerebral region (mesial temporal cortex tau predominance in AD). However, pure tau pathology in the absence of Aβ plaques is characteristic of a heterogeneous group of neurodegenerative disorders included under the term frontotemporal lobar degeneration. About half the frontotemporal lobar degenerations are ubiquitinopathies with TDP-43 (e.g., amyotrophic lateral sclerosis), and the other half are tauopathies, including Pick disease, progressive supranuclear palsy, corticobasal degeneration, and frontotemporal dementia and parkinsonism linked to chromosome 17. The familial tauopathies linked to tau gene mutations have provided compelling evidence that tau abnormalities alone could cause pathologic protein aggregates and massive neuronal loss leading to symptomatic onset (3,4). The last proposed clinical diagnosis criteria for frontotemporal lobar degeneration are based on recent advances in molecular genetics, biochemistry, and neuropathology (4). Specific therapies targeting the hallmark proteins of these pathologies are being investigated. However, it may be challenging to accurately classify these diseases in the clinic, particularly in the early stages, and to select appropriate patients for specific therapies in the absence of biomarkers. Accurate detection of pathologic hallmarks other than Aβ in vivo is therefore a current unmet need. In clinical practice, tau PET imaging could be potentially useful in the early detection and differential diagnosis of AD and non-AD tauopathies as well as in identifying subjects with traumatic brain injury–chronic traumatic encephalopathy who are at risk of developing dementia. As a marker of neurodegeneration, tau PET imaging could help in monitoring disease progression and severity. Clinical trials of disease-modifying therapies could also benefit from tau PET imaging. Enriched populations of patients showing cerebral tau accumulations early in the disease process, and the measurement of changes in tau over time, may decrease risks inherent in the drug development process and contribute to the discovery of effective treatments. As opposed to nonimaging biomarkers for tau (e.g., cerebrospinal fluid), PET imaging offers the advantage of providing a topographic mapping of the amount and distribution of the tau protein in the human brain in vivo. Hence, intensive research is currently ongoing to develop PET radioligands that are capable of detecting deposits of tau in vivo in an accurate and diagnostically relevant manner.
IDEAL CHARACTERISTICS OF A TAU PET TRACER AND CHALLENGES IN ITS DEVELOPMENT
The ideal radioligand for tau must share the general characteristics required of any PET radiotracer for brain imaging, such as the ability to cross the blood–brain barrier, not being a P-glycoprotein substrate, having high affinity and selectivity for the target, having suitable pharmacokinetics for PET imaging, lacking radioactive metabolites that cross the blood–brain barrier, and having favorable dosimetry. However, because of the peculiarities of the tau protein, fulfilling all these requirements may be challenging (Fig. 1) (5,6). First, given the intracellular location of tau, the radiotracer must be able to cross not only the blood-brain-barrier but also the cell membrane and enter the neuron. Second, the ideal tau radiotracer should be able to recognize and bind to deposits of all 6 tau isoforms, allowing imaging of both AD and non-AD tauopathies. Third, tau aggregates may also be present in white matter; hence, an optimal tau tracer should not show nonspecific tracer retention in this region. Also, the frequent colocalization of various protein deposits in the brain at different relative concentrations requires stringent selectivity and affinity criteria. For this reason, results from human brain homogenates containing mixtures of proteins should be interpreted with caution. Lastly, a truly comprehensive tau tracer should be able to recognize and bind to tau deposits irrespective of the number or identity of posttranslational modifications seen in vivo. For this reason, experiments should ideally be performed on human brain slices rather than on recombinant tau fibrils, which lack various posttranslational modifications and other morphologic aspects of in vivo tau deposits. In conclusion, the hunt for a tau tracer that overcomes all these challenges is considerably more daunting than appears at first sight. Nevertheless, considerable progress has been made and several ligands have entered human imaging studies.
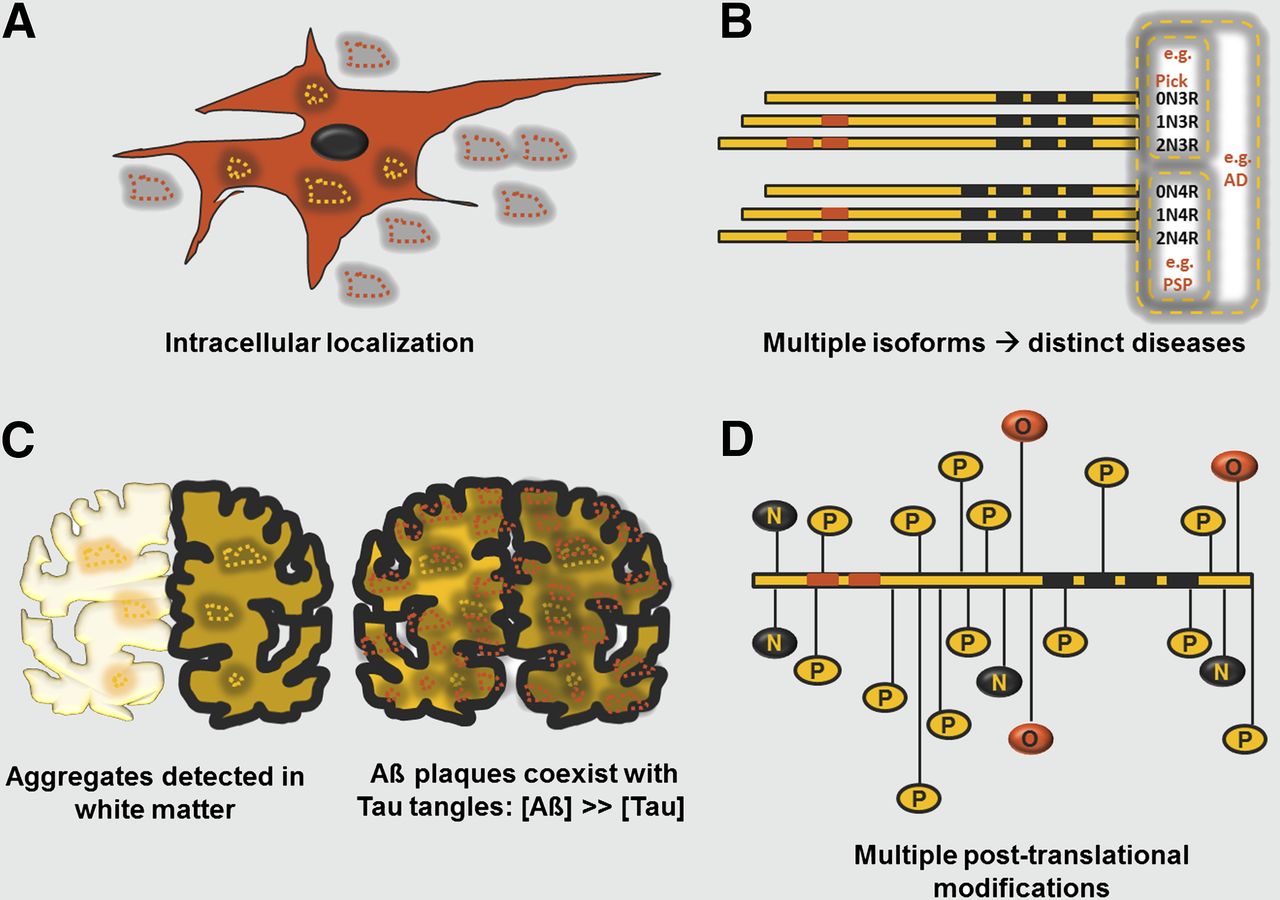
Challenges during development of tau radioligand. (A) tau aggregates (yellow punctata) are intracellularly localized as opposed to extracellular Aβ deposits (red punctata). (B) The 6 isoforms of tau are differentially represented in distinct diseases. (C) tau aggregates are present in white matter. Also, tau aggregates [Tau] colocalize with and are present in much lower concentrations than Aβ plaques [Aβ]. (D) Diverse posttranslational modifications of tau, for example, hyperphosphorylation (P), nitration (N), and O-GlcNAcylation (O) of multiple residues, give rise to various forms of protein.
OVERVIEW OF TAU PET TRACERS UNDER DEVELOPMENT
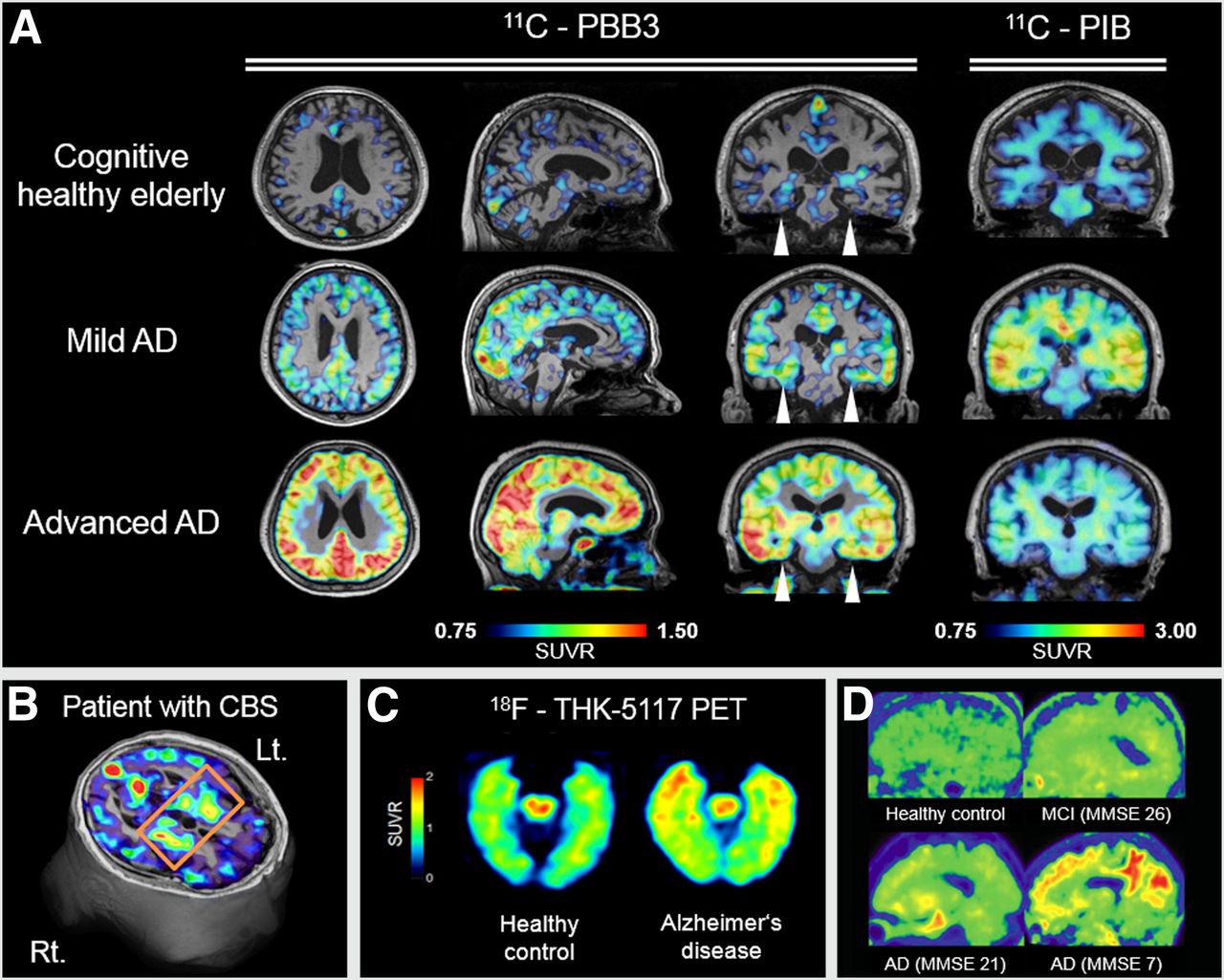
18F-FDDNP was the first 18F-labeled tracer aimed at tau PET imaging. However, binding to Aβ and α-synuclein besides tau has been demonstrated (7), complicating image interpretation. Several molecules are being validated for use as alternative tau tracers. These include, but are not restricted to, 11C-N-methyl lansoprazole, 11C-PBB3, 18F-THK523, 18F-THK5105, 18F-THK5117, 18F-T808, and 18F-T807. A summary of the characteristics of each compound is provided in Figure 2. 11C-N-methyl lansoprazole is the 11C-labeled version of the Food and Drug Administration–approved drug lansoprazole and appears to have an exceptionally high affinity for tau (8). However, to the best of our knowledge no human data have been published with this radiotracer yet. 11C-PBB3 shows high specificity for tau deposits over Aβ plaques (9,10). Initial human studies with this radiotracer show limited white matter background signal and minimal Aβ detection as compared with the Aβ ligand 11C-Pittsburgh compound B (Fig. 3A). Preliminary results with 11C-PBB3 have shown that tau accumulation correlates with clinical symptoms and that its localization in the brain follows the Braak and Braak stages, starting in the hippocampus and limbic system in a subset of nondemented elderly subjects and in subjects with mild cognitive impairment, and spreading to the neocortex in subjects with AD. In addition, 11C-PBB3 appears to detect tau pathology in diseases other than AD, for example, corticobasal syndrome, suggesting an ability to recognize multiple isoforms of the tau protein (Fig. 3B). However, 11C-labeled tracers (half-life, 20 min) are not suitable for widespread use, particularly in clinical practice, where 18F-labeled tracers (half-life, 110 min) are preferable.

Summary of characteristics of tau PET radiotracers being tested in humans.

Tau PET scan images in humans. (A) Coregistered MR imaging and 11C-PBB3 parametric standardized uptake value ratio (SUVR) images compared with 11C-Pittsburgh compound B. No significant radiotracer retention is seen in cognitively healthy elderly subject. Note different uptake pattern in hippocampus between 11C-PBB3 and 11C-Pittsburgh compound B across subjects (arrowheads), and spread of 11C-PBB3 accumulation to cortical areas in advanced AD patient, who shows some cortical uptake in 11C-Pittsburgh compound B scan. (B) 11C-PBB3 PET axial slice over 3-dimensional MR imaging of corticobasal syndrome patient with left-sided symptomatic predominance, showing 11C-PBB3 accumulation in right basal ganglia (Courtesy of Drs. Hitoshi Shimada and Makoto Higuchi). (C) 18F-THK-5117 SUVR images (50–60 min after injection). Higher tracer uptake in anterior pole and mesial aspect of temporal lobes in AD patient (87 y old, MMSE 25) compared with healthy control (80 y old, MMSE 28). Activity in midbrain may represent nonspecific binding (Courtesy of Dr. Nobuyuki Okamura). (D) 18F-T807 sagittal images (80–100 min after injection). No significant radiotracer uptake is seen in healthy control (56 y old), whereas progressive radiotracer accumulation and spreading from mesial temporal to neocortex is seen in patients as MMSE scores decrease. (Reprinted with permission of (20).)
From the family of arylquinolines, 18F-THK523 shows a high affinity to and selectivity for tau fibrils in vitro (11–13). In humans, the pattern of cortical 18F-THK523 retention does not correlate with Aβ distribution as assessed by 11C-Pittsburgh compound B; instead, it follows the known distribution of tau deposits in the AD brain, thus suggesting that 18F-THK523 selectively binds to tau in AD patients. Unfortunately, failure to label tau-containing lesions in non-AD tauopathies and high retention of 18F-THK523 in white matter precludes its use in research or clinical settings (14). 18F-THK5105 and 18F-THK5117 have been tested in vitro both on recombinant tau fibrils and on brain homogenates from the mesial temporal cortex, yielding promising affinity values (15). However, as previously mentioned, these in vitro assays should be carefully interpreted. Although both compounds show encouraging results in mice, further evidence is required to confirm the real nature of the signal observed in preliminary human imaging data (Fig. 3C) (16).
18F-T808 and 18F-T807 show strong affinities and selectivity for tau versus Aβ in vitro (17,18). Brain uptake and washout values for both are favorable (Fig. 2). Brain PET images with 18F-T808 in humans, however, show intense bone uptake in the skull due to defluorination, which may hamper visual image interpretation (19). Human 18F-T807 PET results seem to be the most promising, although the reported data come from a limited sample of 6 subjects (20). The kinetics appear to be slower than those of amyloid tracers but still favorable, with clearance from white matter. Static images do not show defluorination, and a pattern of retention consistent with Braak staging has been reported (Fig. 3D). However, no data are currently available on the suitability of this radiotracer in non-AD tauopathies.
CHALLENGES AND FUTURE DIRECTIONS
Human data currently available on tau PET imaging are still limited. Although it looks promising, an ideal radiotracer meeting all the extensive criteria outlined above has not been identified yet. Hence, research aimed at identifying an optimal compound is still active. Additional data are required to further characterize the existing tau radioligands, including quantitative validation toward full kinetic modeling, test–retest studies, and human dosimetry. Ultimately, neuropathologic correlations with PET imaging findings will be necessary to confirm tau selectivity against colocalized key proteins besides Aβ, such as α-synuclein and TDP-43 (21). Head-to-head studies will allow direct comparisons between radiotracers. Finally, evidence on impact in patient management and outcomes should be generated. In the meanwhile, the inclusion of tau PET imaging in clinical trials for disease-modifying therapies could certainly contribute to a faster and more efficient development of efficacious drugs.
CONCLUSION
The development of tau radiotracers for PET imaging constitutes a step toward meeting the clinical needs of biomarkers for neurodegeneration. In clinical practice, such a molecular imaging tool could help in early and more accurate diagnosis, as well as in monitoring disease progression of AD and non-AD tauopathies, including movement disorders and traumatic brain injury–chronic traumatic encephalopathy. In research, it could provide useful insights into the pathophysiology of these diseases and contribute to the development of potential new efficacious therapies. Several tau radiotracers are undergoing evaluation in human imaging studies and yielding encouraging data. Additional radioligands are also being intensely developed, and the future of tau imaging looks full of promise.
DISCLOSURE
Maliha Shah and Ana Catafau are Piramal Imaging GmbH employees. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
Drs. Nobuyuki Okamura, Hartmuth Kolb, Hitoshi Shimada, and Makoto Higuchi provided PET images. Drs. Nobuyuki Okamura, Makoto Higuchi, and Andre Müller provided critical reading. Dr. Heribert Schmitt-Willich and Jörg Jannsen provided assistance with chemical structures and figures, respectively. Drs. Ken Marek, Marwan Sabbagh, Giovanni Frisoni, Raquel Sanchez, Jose Luis Molinuevo, Maria Jose Marti, and Yaroslau Compta provided useful discussions.
Footnotes
Published online May 15, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication March 13, 2014.
- Accepted for publication April 25, 2014.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Evaluation of the {alpha}-synuclein PET radiotracer (d3)-[11C]MODAG-001 in pigs
- Sex Differences in in vivo Alzheimers Disease Neuropathology in Late Middle-Aged Hispanics
- Preclinical Evaluation of 18F-JNJ64349311, a Novel PET Tracer for Tau Imaging
- Tau Positron Emission Tomography Imaging
- Preclinical Characterization of 18F-MK-6240, a Promising PET Tracer for In Vivo Quantification of Human Neurofibrillary Tangles
- Small-Animal PET Imaging of Tau Pathology with 18F-THK5117 in 2 Transgenic Mouse Models