


Abstract
New multiple myeloma (MM) treatments—such as high-dose melphalan therapy plus autologous stem cell transplantation or regimens incorporating bortezomide, thalidomide, and lenalidomide—substantially increase the rate of complete response that is associated with longer patient survival. Thus, maintaining the complete response status by improving the minimal residual disease after induction therapy is a key goal for MM management. Here, we address the question of radioimmunotherapy efficacy in MM minimal residual disease treatment in mice with a low tumor burden. α-emitters are particularly well adapted to this approach because the short range of α-particles enables localized irradiation of tumor cells within the bone marrow and a cytotoxic effect on isolated cells due to the high LET (linear energy transfer) of α-particles. The CD138 antigen was used as a target because of its strong expression on myeloma cells in 100% of patients. Method: Intravenous injection of 106 5T33 mouse myeloma cells into the Syngeneic mouse strain C57BL/KaLwRij resulted in a rapid invasion of the marrow and limb paralysis, as illustrated by bioluminescence imaging with luciferase-transfected 5T33 cells. Radioimmunotherapy was performed 10 d after 5T33 cell engraftment with an intravenous injection of an antimouse CD138 antibody radiolabeled with 213Bi at activities of 1.85, 3.7, 7.4, and 11.1 MBq. A blood cell count was performed weekly to monitor hematologic toxicity. The levels of blood Flt3 ligand were also measured to evaluate the radioimmunotherapy-related myelotoxicity. Disease progression was monitored by titrating the monoclonal IgG2b antibody produced by 5T33 cells. Results: The groups treated with 3.7 and 7.4 MBq exhibited a median survival greater than 300 and 227 d, respectively, compared with 45.5 d in the control untreated group. The highest activity (11.1 MBq) showed short-term toxicity whereas the lowest activity (1.85 MBq) gave results similar to those of the controls. With activities of 3.7 and 7.4 MBq, mice exhibited a transient hematologic toxicity whereas only temporary and moderate myelotoxicity was observed with 7.4 MBq. Conclusion: This study demonstrates promising therapeutic efficacy of 213Bi-labeled anti-mCD138 for the treatment of residual disease in the case of MM, with only moderate and transient toxicity.
Multiple myeloma (MM) is a malignant plasma cell disorder characterized by the proliferation of clonal cells in the bone marrow and, at later stages of the disease, in extramedullary sites (1). MM accounts for approximately 10% of hematologic cancers and 1% of all cancers, with an annual incidence of 4–6 cases per 100,000 population. The median survival of this incurable disease has markedly improved over the last decade because of the extensive use of high-dose therapy and autologous stem cell transplantation in younger patients and the introduction of novel agents (i.e., thalidomide, bortezomib, and lenalidomide used in combination with dexamethasone or alkylating agents) (2). Other drugs, such as inhibitors of histone deacetylase (vorinostat, panobinostat) or monoclonal antibodies (mAbs) (elotuzumab), are also under development in large prospective phase 2 and 3 studies (3).
These new therapeutic approaches have led to an increase in complete response (CR) associated with improved survival. Thus, maintaining the CR status by improving the elimination of minimal residual disease after induction therapy is a major goal for MM therapy. Maintenance therapy after induction or autologous stem-cell transplantation improves CR and survival but at the cost of toxic side effects, especially in elderly patients. One of the challenges in MM therapy is thus to maximize survival outcomes and minimize treatment-related toxicities, while offering the best supportive care. Radioimmunotherapy could satisfy these requirements. Indeed, the use of mAbs has become a realistic strategy for the targeted delivery of therapeutic radionuclides to tumor cells in various B-cell malignancies. The selection of radionuclide–antibody combinations is critical for radioimmunotherapy to become a standard therapeutic modality. To date, 2 radioimmunotherapy agents have been fully approved for commercial use: 90Y-ibritumomab tiuxetan and 131I-tositumomab. Both compounds target CD20 expressed on the surface of normal and malignant B cells.
Besides β-emitters, α-emitters also hold promise for radiation-based therapy because of their high linear energy transfer, enabling localized irradiation while preserving surrounding tissues. The level of cell toxicity achieved with only a few α-particle tracks is adapted for the targeting of isolated cells as is required in hematologic malignancies such as MM. α-particles have been used for systemic injection of bone seeker isotopes such as 223Ra (4) in the palliative treatment of bone metastases of advanced prostatic cancer. However, the osteoclastic property of MM is not adapted to the property of 223Ra to accumulate in bone and osteoblastic sites. We thus favor a more specific targeting of myeloma cells with α-radioimmunotherapy.
Only few α-radioimmunotherapy clinical trials have been performed in the context of hematologic diseases. Jurcic et al. performed radioimmunotherapy assays targeting the CD33 antigen in patients with leukemia. They clearly showed the feasibility of tumor targeting within the bone marrow using 213Bi coupled to a mAb. Treatment was well tolerated, with only transient toxicity, but therapeutic benefit was limited because of a lack of antigen expression on some tumor cells and because the patients’ tumor burden was too high compared with the available radiolabeled mAb (5). This observation led to the conclusion that α-particles are more suited to the treatment of residual disease. Indeed, in a subsequent clinical trial, the same team combined cytoreduction with short-course cytarabin treatment and α-radioimmunotherapy and confirmed the potential of α-radioimmunotherapy in the treatment of residual disease. Consolidation treatment for MM with α-radioimmunotherapy aimed at minimizing residual disease and prolonging CR after induction treatment is an attractive therapeutic alternative. Targeting MM cells by radioimmunotherapy with a radiation-induced mechanism of toxicity would provide the opportunity to reinforce the efficacy of consolidation therapy against residual MM cells that develop resistance to a different mechanism of action of a previous induction treatment.
For α-radioimmunotherapy studies to be successful in MM, the third element of the pathology–radionuclide–target triad still needs to be defined. Targeting CD54 (6) and CD317 (7) in vitro and in vivo in MM xenograft mouse models has been shown to be efficient for the killing of human MM by antibody-dependent cell-mediated cytotoxicity (ADCC), complement-dependent cellular cytotoxicity (CDCC), or antibody-dependent cellular phagocytosis. However, the expression of CD54 and CD317 antigens on the lumen-exposed endothelial lining (8) directly accessible to the blood-borne radiolabeled antibody would impair radioimmunotherapy efficiency by minimizing the amount of antibody available to the target tumor and by causing systemic damage to the vasculature. Immunotherapy with anti-IL-6 mAb has also been performed. A transient tumor cytostasis was achieved, which did not result in a cure (9). More specific targeting has been performed focusing on the CD38 antigen on MM cells. This antigen is highly expressed on myeloma cells, and antibodies directed against CD38 are capable of mediating ADCC and CDCC in vitro or in vivo in a MM xenograft mouse model. The expression of CD38 combined with CD138 is currently used to characterize MM. In this respect, CD138 (also called syndecan-1) is a promising target for mAb-based α-radioimmunotherapy. In this study, we focus on CD138 and evaluate its relevance for α-radioimmunotherapy of MM. Syndecan-1 belongs to the family of heparan sulfate proteoglycans and is expressed by the epithelium as well as by precursor B cells and plasma cells. Syndecan-1 is expressed at high levels in all MM tumors within the bone marrow (10–12) and plays a key role in regulating MM (13).
We thus developed an α-radioimmunotherapy assay with 213Bi-labeled antimouse CD138 in an orthotopic syngeneic mouse 5T33 MM model. The syngeneic model provides the opportunity for insight into the biodistribution of the radiolabeled antibody in healthy tissues expressing the targeted antigen. The 5T33 cell line mimics an aggressive human variant of MM (14), with bone marrow involvement, and in this regard provides information for the possibility of targeting tumor cells within the bone marrow by α-radioimmunotherapy. The radioimmunotherapy was performed 10 d after engraftment at a low tumor burden to estimate the potential of α-radioimmunotherapy for the consolidation treatment of patients in CR after induction therapy.
MATERIALS AND METHODS
MM Mouse Model
The 5T33 murine MM cells line was kindly provided by Dr. Harvey Turner (Department of Nuclear Medicine, Fremantle Hospital) with the permission of Dr. Jiri Radl (TNO Institute) (15). The cells were cultured in RPMI1640 medium (Gibco) containing 2 mM l-glutamine and 10% heat-inactivated fetal calf serum (PAA Laboratories/GE Healthcare Europe GmbH). The cells were incubated at 37°C, 5% CO2, 95% humidity. Aliquots of early passaged cells were frozen in 10% dimethylsulfoxide and 90% fetal calf serum and stored at −196°C for later reconstitution.
Female C57BL/KaLwRij mice were purchased from Harlan CPB and housed in our animal facility at the CRCNA. They were housed under conventional conditions. All mice were 8–10 wk old at the beginning of each experiment. Experiments performed in this study were approved by the local veterinary services (license no. B44.565). One million 5T33 cells were grafted intravenously into the mouse tail. Treatment was initiated 10 d after transplantation.
Bioluminescence Imaging
A sequence containing complementary DNA coding for luciferase was obtained by HindIII-SalI digestion of the pGL3 vector (Promega). The fragment was cloned into HindIII and SalI sites of the retroviral vector pMX (16). Luciferase retroviral supernatant was produced by Phoenix-Ampho packaging cells (CRL-3215; American Type Culture Collection).
Retroviral transduction of 5T33 cells was performed by centrifuging 1 × 106 MM cells twice at 2,400g for 90 min with 1 mL of retroviral supernatant and 8 mg/mL polybrene (Aldrich). Four days after retroviral transduction, 5T33 cells were cloned by limiting dilution.
For in vivo imaging, mice were anesthetized by intraperitoneal injection of 10 μL per gram of mouse weight of phosphate-buffered saline (PBS) supplemented with ketamine chlorhydrate (Ketalar [Panpharma]; 50 mg/mL) and xylazine 2% (Rompun; Bayer) (30:5:3). Live in vivo imaging was performed 5 min after injection of 100 μL of luciferin (12 mg/mL) and analyzed with a photon Imager (Biospace Lab).
Antibody Immunoreactivity and Affinity
The IgG2a k rat anti-mCD138 (BD Pharmingen) recognizes a transmembrane heparan sulfate proteoglycan, syndecan-1, which is expressed by normal and malignant plasma cells. Immunoreactivity was determined according to the Lindmo cell-binding assay using mCD138 mAb-positive 5T33 cells. The number of antigen binding sites per 5T33 cell was determined by Scatchard analysis as previously described (17). The binding data were analyzed by a nonlinear regression using the Prism software package (GraphPad Software Inc.).
Antibody Radiolabeling
The anti-mCD138 rat antibody was modified with 2-(4-isothiocyanatobenzyl)-cyclohexyl-diethylenetriaminepenta-acetic acid (SCN-CHX-A″-DTPA; Macrocyclics) as previously described (18). In brief, the antibody was incubated with 20 equivalents of (mol/mol) CHX-A″-DTPA in carbonate buffer (0.05 M, pH 8.7) and, after overnight incubation at room temperature, purified by high-performance liquid chromatography on a Sephadex G200 gel-filtration column (Amersham Biosciences). The mean chelate number per antibody was 2, as assessed with 4 equivalents of a buffered citrate-acetate (0.02/0.15 M, pH 5.5) 111In solution. For labeling with 213Bi, the immunoconjugate was incubated with 213Bi eluted from a 225Ac/213Bi generator (Institute for Transuranium Elements) for 10 min in 0.8 M ammonium acetate (pH 5.3). The resulting 213Bi-labeled immunoconjugate was separated from unbound 213Bi by size-exclusion chromatography using a PD-10 column (GE Healthcare) (19). Radiochemical purity was greater than 95%, as determined by instant thin-layer chromatography silica gel (ITLC-SG) using 10% trichloroacetic acid (TCA) as the solvent. For 111In radiolabeling, 200 μg (100 μL) of anti-mCD138 rat antibody coupled with CHX-A″-DTPA was mixed with 100 μL of ammonium acetate buffer (0.5 M, pH 5.0), 100 μL of HCl 0.06N, and 4.4 MBq of 111InCl2. The mix was incubated 30 min at 37°C. The radiolabeling was controlled by ITLC-SG using 10% TCA as the solvent. Free 111In was excluded using a size-exclusion chromatography PD-10 column (GE Healthcare). Radiochemical purity was greater than 99%.
Biodistribution
All animal experiments were conducted in accordance with institutional guidelines according to ongoing national regulations issued by INSERM and the French Department of Agriculture. Mice with or without tumors were administered 50 kBq of 111In-labeled anti-mCD138 (3 μg) via the tail vein. Three mice were sacrificed 90 min after the injection, their tumors and organs were removed and weighed, and the radioactivity was counted using a γ-counter. The results were expressed as percentage injected dose per gram (%ID/g). Anti-CD138 binding in femurs and flat bones was compared between normal mice and mice that had received a tumor-graft via intravenous administration of 1 million 5T33 cells via the tail. The analysis was performed 10 d after engraftment and 90 min after 111In-labeled anti-mCD138 injection. The comparison was made with an unpaired t test using Prism software package (GraphPad software Inc.).
Radioimmunotherapy Dose Escalation Study
MM radioimmunotherapy using the 213Bi-labeled anti-mCD138 antibody was performed in groups of 10 mice, with 4 injected activities (1.85, 3.7, 7.4, and 11.1 MBq). Two control groups were included: one receiving PBS and the other receiving a control antibody, 6H4, targeting human beta2 microglobulin, which was also labeled with 213Bi (injected activity, 3.7 MBq). The endpoint of the study was death without prior signs of pain, a body weight loss greater than 10%, or signs of paralysis leading to mobility impairment. Mice were killed according to our animal protocol. Groups were compared using the nonparametric ANOVA with Bonferroni adjustment. Survival curves were calculated according to the Kaplan–Meier method and compared with the log-rank test. All analyses were 2-sided. P values of 0.05 or less were considered significant. These analyses were performed using Prism (GraphPad Software Inc.).
Quantification of Mouse Myeloma IgG2b by Enzyme-Linked Immunosorbent Assay (ELISA)
The levels of monoclonal IgG2b produced by 5T33 cells in vivo were measured in the plasma of treated mice by a sandwich ELISA. ELISA microplates (Nunc) were coated overnight at 4°C with goat antimouse IgG2b (2 μg/mL) (BD Pharmingen). Plates were washed 3 times with PBS–0.05% polysorbate-20 and blocked with 200 μL of PBS–1% bovine serum albumin for 1 h at room temperature. After blocking, serial dilutions of samples (1/1,000, 1/10,000, and 1/100,000) and of an IgG2b standard (from 10 ng/mL to 2.5 μg/mL) were added, and plates were incubated for 2 h at room temperature. Plates were then washed 3 times with PBS–0.05% polysorbate-20. Plates were then incubated with alkaline phosphatase–coupled goat antimouse IgG2b (BD Pharmingen) at 1:2,000 in PBS–1% bovine serum albumin for 2 h at room temperature. Finally, all the plates were developed with p-nitrophenyl phosphate (1 mg/mL) (R&D) for 20–30 min at 20°C. Measurements were performed at 405 nm with an ELISA microplate reader.
Toxicity Monitoring
White blood cells, red blood cells, and platelet counts were automatically measured by a quantitative automated hematology analyzer (Melet-Schloesing Laboratories) over a period of 6 wk, and blood samples were obtained by retroorbital bleeding every 7 d after treatment. Blood samples were collected on ethylenediaminetetraacetic acid.
Flt3-L was measured in the plasma of treated mice using a commercially available ELISA system (R&D Systems), according to the manufacturer’s recommendations.
Plasma prepared from samples used for blood cell counts and monoclonal Ig titration was pooled in equal volumes for each surviving mouse. Aspartate transaminase (ASAT), alanine transaminase (ALAT), and creatinine were quantified on a Hitachi 917 Chemistry Analyzer (Roche).
RESULTS
Targeting 5T33 MM Cells with Anti-mCD138 mAb
Equilibrium binding assays with the 125I-labeled anti-mCD138 antibody revealed that 5T33 cells express approximately 200,000 CD138 molecules at their cell surface. The antibody affinity (dissociation constant) was 4 nM. The coupling of the anti-mCD138 with the bifunctional chelating CHX-A″-DTPA-agent used for radiolabeling with 213Bi did not impair the immunoreactivity of the mAb because the affinity measured with the modified mAb was unchanged, compared with the 125I-labeled anti-mCD138 (data not shown). This antigenic site number and antibody affinity were appropriate for radioimmunotherapy.
Therapeutic Window for Consolidation Treatment of MM with Radioimmunotherapy
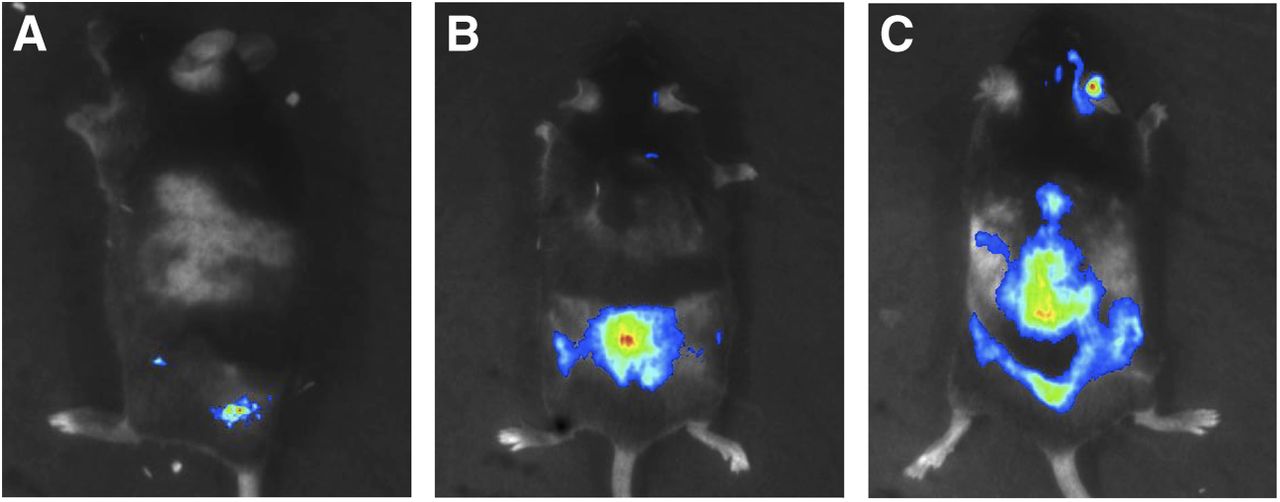
In mice MM models, chemotherapeutic treatment delays death but never leads to a state of CR (defined in humans treated with the same molecules as negative immunofixation and disappearance of monoclonal protein in serum and urine). In this syngeneic mouse model of MM, the appearance of a significant increase in 5T33 monoclonal Ig coincides with limb paralysis and death within a week, indicating an advanced stage of the MM progression at the time of monoclonal Ig detection. We used luciferase-transfected 5T33 cells to monitor in vivo tumor progression to determine the treatment window that would be representative of complete remission with undetectable residual disease, as defined in humans, so as to evaluate the efficacy of α-radioimmunotherapy for consolidation treatment. After intravenous injection of 1 M 5T33 cells transfected with luciferase (5T33-Luc+), bone marrow involvement was first detectable at day 12. MM then progressively invaded the skeleton within 2 wk and by day 44, 5T33-Luc+ cells had invaded most of the rachis (Fig. 1), as observed in humans at the later stages of disease progression. We thus chose to treat animals at day 11, after MM cell injection and just before objective bone marrow involvement. We chose the 5T33 cell line instead of the 5T33 Luc+ cells to prevent the immune response against Luc+ cell lines reported by others in an immunocompetent mouse model (20) that could artificially modify the response to treatment, compared with the nontransfected syngeneic 5T33 MM cell line.

Bioluminescence imaging of early invasion of 5T33-Luc+ MM cells in C57BL/KaLwRij mice. Images were obtained by bioluminescence at 12 (A), 20 (B), and 44 (C) days after intravenous injection of 106 5T33-Luc+ cells. Imaging was performed under general anesthesia and 5 min after intraperitoneal injection of luciferin.
Biodistribution of Anti-mCD138 mAb
The biodistribution of 111In-labeled anti-mCD138 antibody was studied in C57BL/KaLwRij mice without tumor engraftment to monitor anti-mCD138 accretion in healthy organs.
Tissue distribution and concentration (%ID/g), analyzed 90 min after injection, are shown in Figure 2. With the exception of the liver, the overall 111In-labeled anti-mCD138 mAb uptake in other healthy organs was low (Fig. 2). The high liver uptake is related to the expression of CD138 on the microvilli of hepatocyte basal membranes, facing the space of Disse (21). We confirmed that liver uptake of anti-CD138 antibody depends on antigen binding by immunohistochemistry (Supplemental Fig; 1; supplemental materials are available at http://jnm.snmjournals.org). To validate the ability of anti-mCD138 mAb to bind to MM cells in vivo, we compared the distribution of the anti-mCD138 antibody in the bone of engrafted mice with control animals. A significant difference was observed between the %ID/g of control bone and bone invaded by MM. At, 90 min, anti-mCD138 targeted MM cells in the femur (P = 0.014) and in flat bones (P = 0.0256). However, although significant, these biodistribution data in the bone of 5T33-engrafted mice are insufficient to estimate mAb uptake by tumor tissues, because it is impossible to estimate the tumor mass within the femur red marrow. These results are presented in the supplemental data (Supplemental Fig. 2).
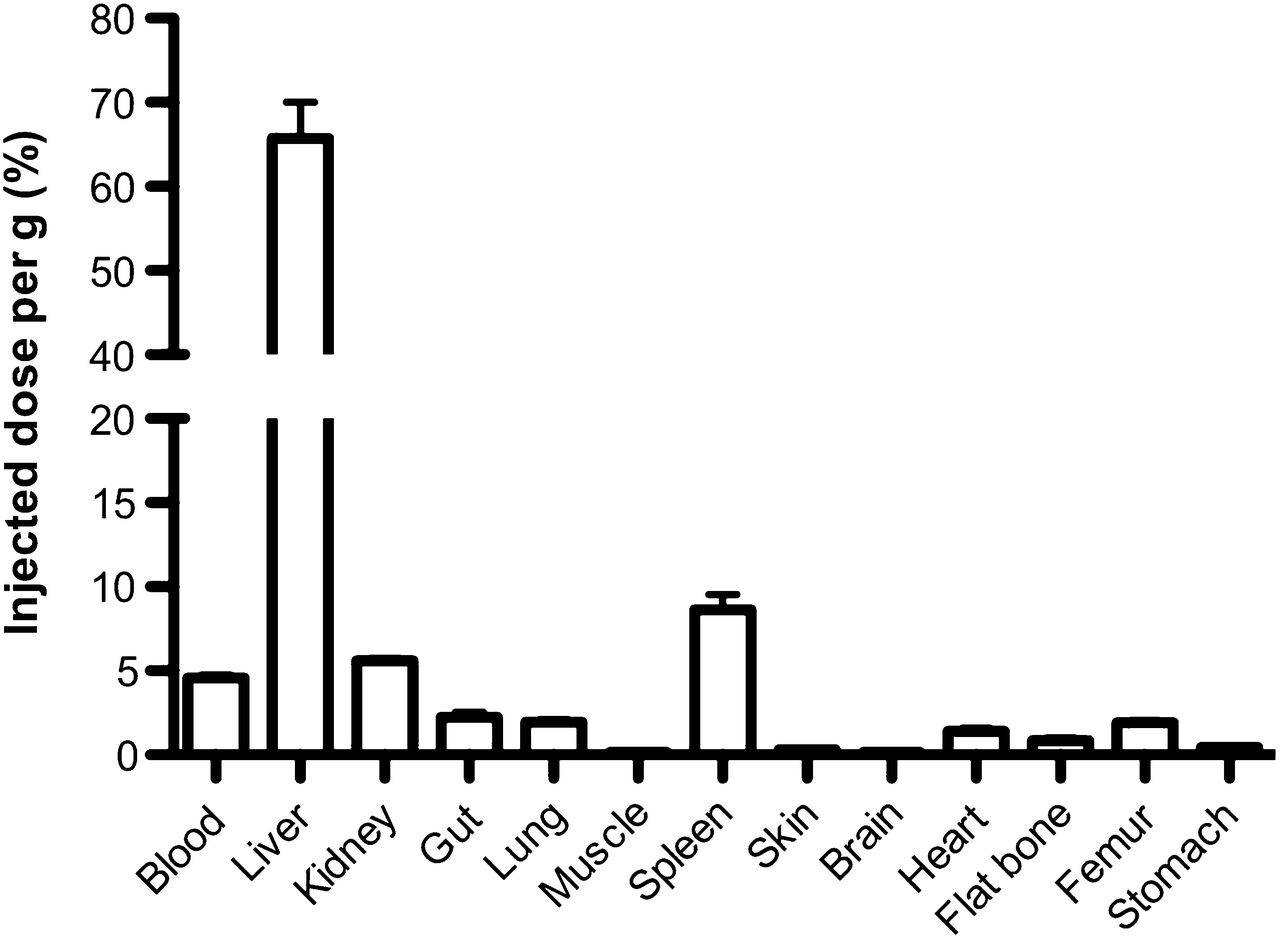
Biodistribution of 111In-anti-mCD138 in C57BL/KaLwRij mice. Biodistribution of 111In-anti-mCD138 in %ID/g in different tissues 90 min after injection of 111In-anti-mCD138.
Radioimmunotherapy with 213Bi-Labeled Anti-mCD138
Radioimmunotherapy of MM in mice using the 213Bi-labeled anti-mCD138 was performed 10 d after engraftment with 106 5T33 cells. Groups of 10 mice received an intravenous injection of 1.85, 3.7, 7.4, and 11.1 MBq of 213Bi-labeled anti-mCD138 and were compared with a control group of mice that received an injection of PBS and with a second control group that received 3.7 MBq of the irrelevant 213Bi-labeled 6H4 antibody specific for human beta2 microglobulin.
Kaplan–Meier survival curves showed a significant improvement in survival of C57BL/KaLwRij MM mice treated with 3.7 and 7.4 MBq of 213Bi-labeled anti-mCD138, compared with the PBS or 6H4 control groups (Fig. 3). Although the lowest activity (1.85 MBq) appeared to be inefficient at treating MM in this model, median survival increased from 46 d in the PBS control group to 227 d in the group treated with 7.4 MBq of 213Bi-labeled anti-mCD138 antibody (P < 0.0001) and to more than 300 d in the group treated with 3.7 MBq (P < 0.0001). No significant survival difference was observed between mice that received either 3.7 or 7.4 MBq at the end of the study; mortality in the 7.4-MBq group was higher than in the 3.7-MBq group, a sign of acute toxicity at this injected activity. At the highest injected activity (11.1 MBq), all mice died within 7 d after treatment, indicating that this activity was toxic.
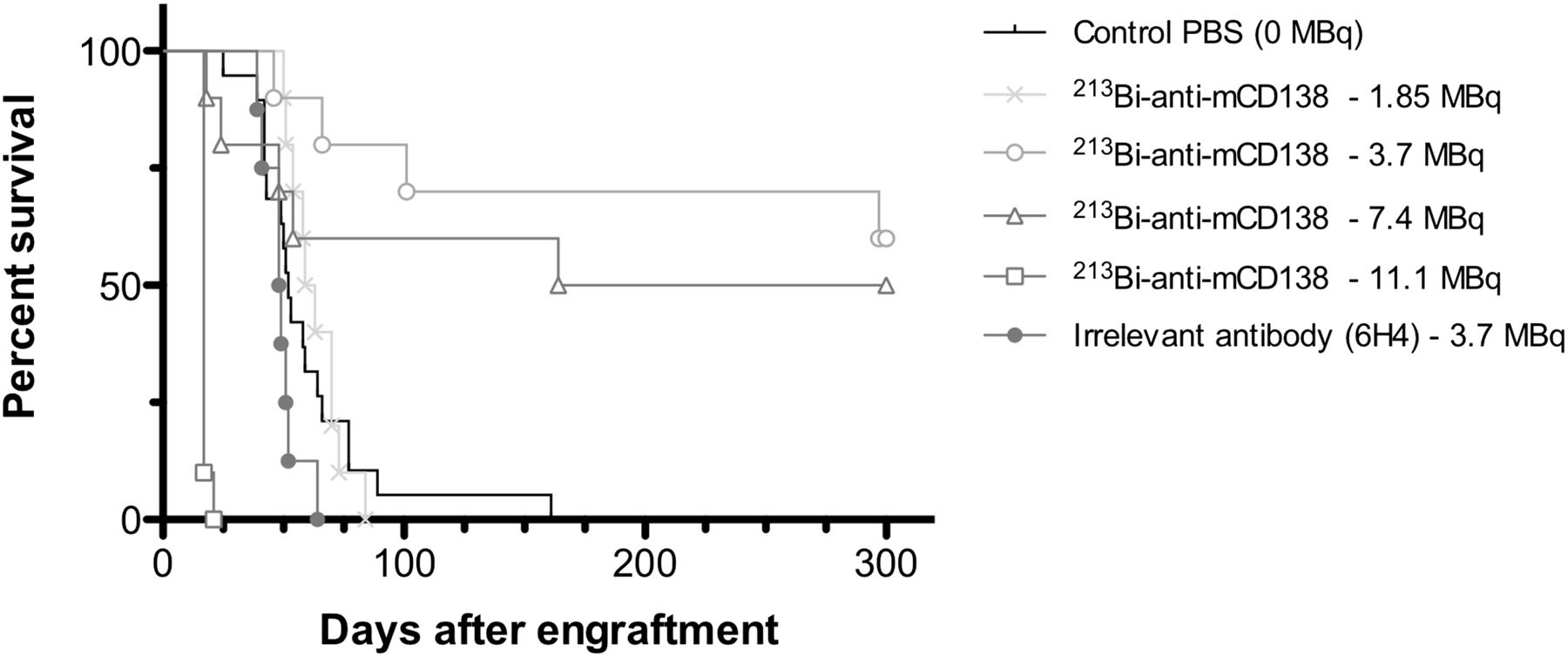
Kaplan–Meier survival curves of C57BL/KaLwRij mice grafted with 106 5T33 MM cells treated with 213Bi-anti-mCD138 at 1.85, 3.7, 7.4, and 11.1 MBq and irrelevant mAb at 3.7 MBq and PBS.
Monitoring of MM Monoclonal Ig Blood Concentrations During Radioimmunotherapy
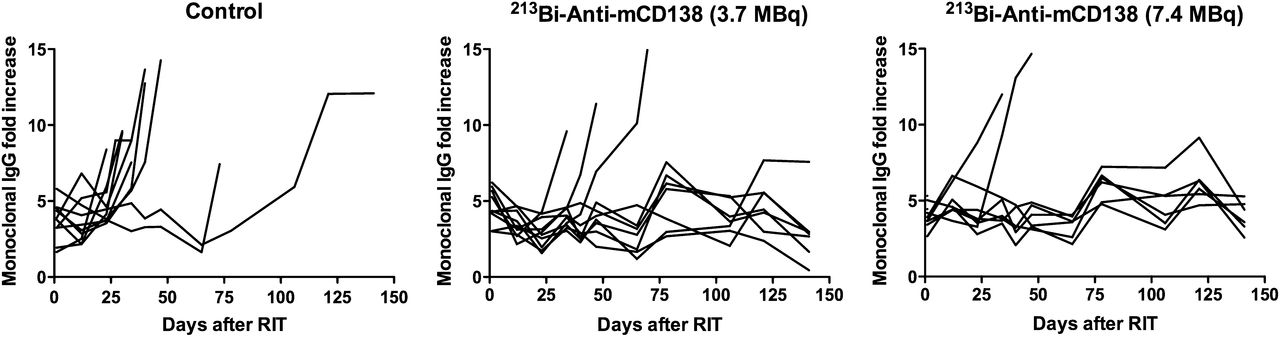
To further investigate the efficacy of radioimmunotherapy for MM treatment, the blood concentration of 5T33 MM monoclonal Ig was monitored using a specific ELISA (Fig. 4). Disease progression was clearly accompanied by an increase in MM monoclonal Ig level: in the control group, MM monoclonal Ig levels increased rapidly between 40 and 60 d (except for 2 animals that survived longer), in accordance with the 46-d mean survival. This was also observed in the 3.7-MBq treated group, in which MM monoclonal Ig levels dramatically increased a few days before the death of the 3 animals that were not cured. Conversely, in the 7.4-MBq treated group, among the 4 mice that died before day 75, 2 displayed an increase in blood MM monoclonal Ig, whereas the other 2 died without monoclonal Ig being detected, probably from treatment toxicity.

Immunomonitoring of blood mAb produced by 5T33 MM cells in response to 213Bi-anti-mCD138 at 1.85, 3.7, and 7.4 MBq and PBS control. Isotype-specific ELISA was used to monitor plasma monoclonal Ig levels over 22 wk. RIT = radioimmunotherapy.
Radioimmunotherapy Toxicity
Treatment toxicity was more specifically monitored by measuring animal weight (Fig. 5). In the PBS control group, the mice slowly lost weight as the diseased progressed. No significant weight loss was observed in the 3.7-MBq groups, indicating that the 3.7-MBq activity was not toxic. In the 7.4-MBq group, a slight weight loss around 10% of the initial weight was observed within the 15 d after radioimmunotherapy, suggestive of an acute toxicity at this injected activity. This weight loss was even more dramatic for the 11.1-MBq treated group in which all mice died of toxicity.

Monitoring weight and liver (with ASAT and ALAT) and kidney (with creatinine) toxicities in plasma of C57BL/KaLwRij mice grafted with 106 5T33 MM cells treated with 213Bi-anti-mCD138 at 3.7 and 7.4 MBq and PBS. Mice were weighed weekly over 20 wk after radioimmunotherapy. Results are expressed as percentage of initial weight at day 0 (A). At each time point, creatinine (B), ASAT (C), and ALAT (D) were measured in pool of equal volume of plasma of surviving mice for mice injected with 3.7 MBq, 7.4 MBq, and PBS (0 MBq). RIT = radioimmunotherapy.
Hematologic Toxicity
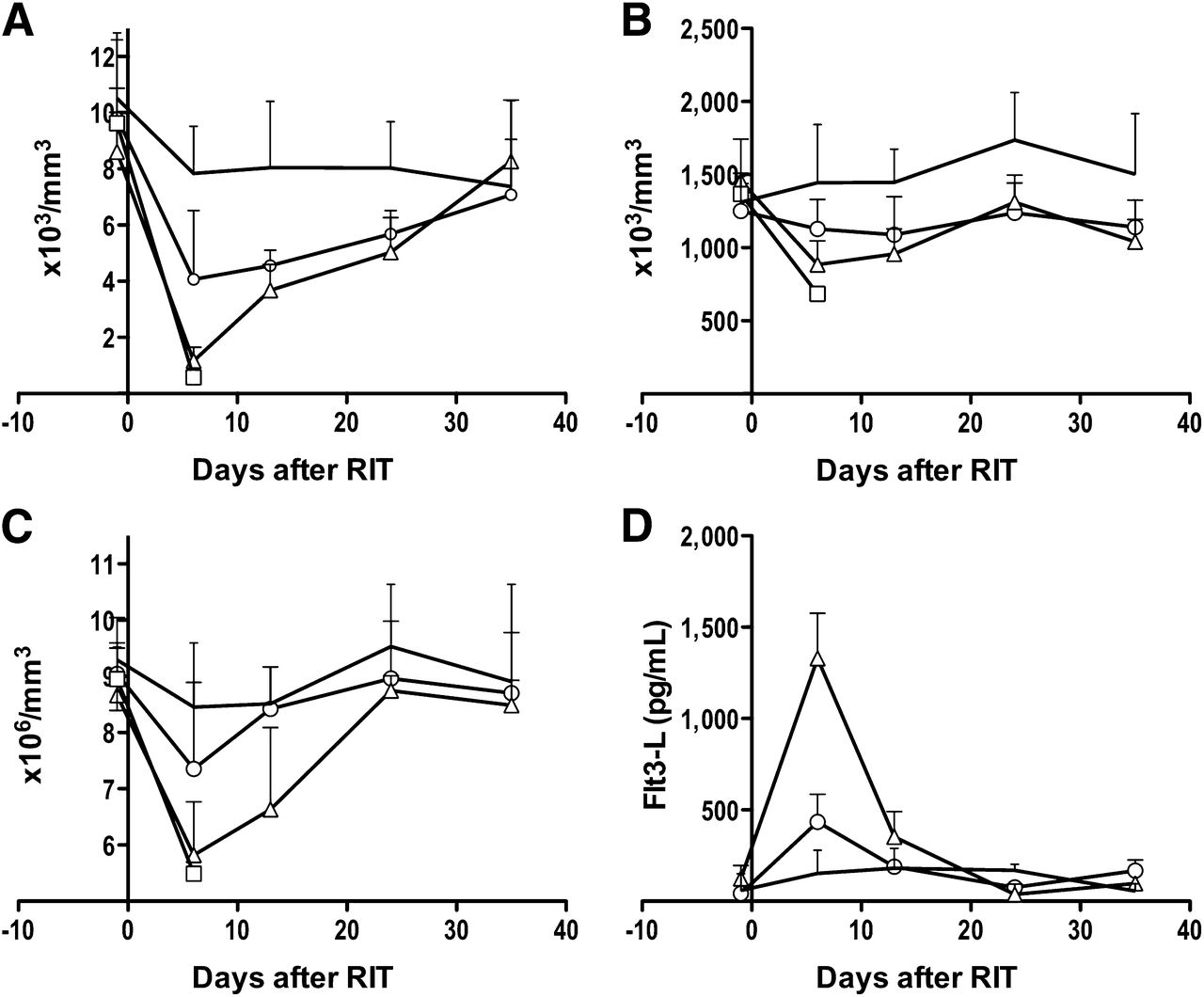
Blood cell count monitoring showed that the toxicity affected leukocytes and, to a lesser extent, platelets and red blood cells (Fig. 6). The leukocyte count dropped early and sharply in the treated groups. As early as 6 d after radioimmunotherapy, the leukocyte counts were reduced to 15% and 50% of the normal levels at the 7.4-MBq and 3.7-MBq injected activity, respectively (Fig. 6). Platelet counts were little affected by α-radioimmunotherapy in the 3.7- and 7.4-MBq groups, compared with day 0 (Fig. 6). On the other hand, red blood cell counts dropped with kinetics identical to those of leukocytes and this was more pronounced at the 7.4-MBq than at the 3.7-MBq activity, with, respectively, 33% and 19% red blood cell loss at day 6 (Fig. 6). This red blood cell toxicity was quite unexpected with regard to the toxicity that is observed in radioimmunotherapy protocols using β-emitters. The high α-particle lineic energy transfer combined with their relatively high dose rate irradiation may account for this particular form of hematologic toxicity.

Hematologic toxicity analysis of C57BL/KaLwRij mice grafted with 106 5T33 MM cells treated with 213Bi-anti-mCD138. Mice treated at 3.7 (○), 7.4 (△), 11.1 MBq (□), and PBS control (bar). Hematologic toxicity was evaluated in surviving mice for each experimental group after radioimmunotherapy. Leukocytes (A), platelets (B), and red blood cells (C) were analyzed weekly over 8 wk using quantitative automated hematology analyzer. (D) Plasma Flt3-L concentration after radioimmunotherapy for animals receiving 3.7 and 7.4 MBq of 213Bi-anti-mCD138 and PBS control have been measured by specific ELISA. Results are given as means and SD of 4 animals per group. RIT = radioimmunotherapy.
Altogether, these results show that the blood cell count decrease was transient and that normal leukocyte, platelet, and red blood cell counts were quickly recovered, independent of the injected activity.
One concern with α-radioimmunotherapy for the treatment of MM is myelotoxicity due to the location of the targeted MM cells within the red marrow. Plasma Flt3-L concentration correlated with radiation-induced bone marrow damage (22). To assess myelotoxicity, we thus measured the Flt3-L concentration on day 6 after irradiation in the plasma of control mice and mice treated with either 3.7 or 7.4 MBq (Fig. 6). The 3.7-MBq activity, which was efficient at treating MM, did not induce any significant increase in plasma Flt3-L, compared with the control group, confirming its low myelotoxicity. Conversely, in the 7.4-MBq activity group, an early and transient peak of Flt3-L at day 6 was indicative of marrow damage. A normal level of Flt3-L in the blood was recovered as rapidly as 12 d after radioimmunotherapy in both groups of treated mice, in accordance with a mild myelotoxicity of the α-radioimmunotherapy at the activities administered.
Nonhematologic Toxicity
Taken together, the results of the radioimmunotherapy show that 3.7 and 7.4 MBq both induced prolonged complete remission of mice, but for the latter dose a transient toxicity was observed, characterized by weight loss, death of mice without an increase in monoclonal Ig, and a transient myelotoxicity. We additionally investigated toxicity to the liver and kidneys using a biochemical approach—that is, measuring the level of plasma creatinine for kidney toxicity and ASAT and ALAT for liver toxicity (Fig. 5). Enzyme activity was measured on a pool of equal volume of plasma collected from the mice of both groups, giving an overview of kidney and liver damage over time. The creatinine was found to remain constant throughout the follow-up period in the 7.4- and 3.7-MBq groups, showing that both doses of radioimmunotherapy were safe for the kidneys. However, a slight and transient increase in creatinine around day 14 after radioimmunotherapy in the 7.4-MBq group may have been related to an acute toxic phase with damage to the kidneys that resolved over time (Fig. 5).
The high level of 213Bi-radiolabeled anti-CD138 uptake by the liver observed by biodistribution analysis suggested that the mortality observed may have been the result of irradiation-induced organ failure. No increase in ALAT and ASAT was observed between the day of radioimmunotherapy and day 50, the time frame for acute toxicity. After day 50, a progressive increase in ASAT and ALAT was observed in the 7.4-MBq group but not in the 3.7-MBq group in which the ASAT and ALAT remained around the baseline level (Fig. 5). Only 1 mouse in the 7.4-MBq group died at day 154 after radioimmunotherapy with no evidence of plasma monoclonal IgG increases, indicating that the death in this animal was probably related to radio-induced toxicity. This indicated that although the 7.4-MBq dose of injected activity was efficient at treating mice with MM, it was accompanied by a chronic radio-induced liver failure, observed with aging in accordance with biodistribution in the liver. This chronic toxicity may be related to the shift in the weight curve in the 7.4-MBq group at day 95, compared with the 3.7-MBq group (Fig. 5). Conversely, 3.7 MBq appeared to be a safe dose because no side effects were observed on the healthy organs and the mice continued to gain weight.
DISCUSSION
MM is a heterogeneous disease with variable cytogenetic abnormalities, response to therapy, and prognosis (23,24). Despite recent therapeutic advances including novel agents, all patients ultimately relapse and new therapeutic options are needed.
In this context, targeted therapies can find their place within the therapeutic arsenal against MM. Within these targeted therapies, mAbs still remain the best means to bring specifically targeted radionuclides to tumor sites. This technique has demonstrated its efficiency in the treatment of B-cell non-Hodgkin lymphoma by targeting different antigens such as CD20 and CD22, with β-particle emitters such as 90Y or 131I (25,26). In the context of MM, the strong expression of syndecan-1 on myeloma tumors makes it a good candidate as a target antigen (27).
α-particles are capable of powerful cytotoxicity (28) with relatively short effective path lengths in tissues. A single atom emitting an α-particle can kill a target cell (29). Therefore, radionuclides emitting α-particles are attractive for cancer therapy, especially to kill isolated malignant cells such as those observed in MM. In their paper, Press’s group discussed this point in the setting of α-radioimmunotherapy in non-Hodgkin lymphoma using anti-CD20 mAb labeled with 213Bi (30). Even though the use of a short-half-life radionuclide (46 min) requires a fast biodistribution of the injected activity, which favors pretargeting, conventional targeting approaches remain realistic in several cases. For instance, clear antitumor efficacy has been observed with intracavitary injection of 213Bi-labeled antibodies for the treatment of ovarian carcinoma (31,32) and bladder cancer (33) and for intrathecal administration for the treatment of brain tumors (34) and breast carcinomatous meningitis (35). In the particular case of MM, the location of tumor cells in the bone marrow, which is highly perfused and almost freely accessible to large molecules such as whole immunoglobulins, enables direct targeting to deliver the activity to tumor cells quickly enough with respect to the radionuclide half-life. In this MM mouse model, the use of a complete antibody did not appear to be limiting for the distribution of α-particles to tumor sites. Indeed, the biodistribution data showed that bone marrow targeting was compatible with short-half-life radionuclides. This is consistent with a phase I/II clinical study using an 131I-labeled antibody targeting human CD138 in MM patients with high tumor burden with the aim of assessing the biodistribution and dosimetry of the 131I-B-B4. In this assay, antibody distribution to the tumor cells in the bone marrow was obtained within minutes after injection. Dosimetry results also suggest the feasibility of radioimmunotherapy for the treatment of advanced stage MM using anti-CD138 (B-B4) radiolabeled with β-emitters whose long persistence in the blood flow make it possible to irradiate large tumor masses over days (36).
Regarding healthy organs, activity uptake was also observed in the liver (∼50 %ID/g at 90 min), which can be linked to the expression of CD138 on hepatocytes (21). This liver uptake in the mouse model is consistent with the dosimetric results obtained in humans for whom liver uptake of the radiolabeled B-B4 antibody was high. In this clinical trial, no hepatic toxicity was observed. The fast decay of 213Bi limited its diffusion from the blood, in contrast to the 131I-labeled antibody that remained stable for days. However, we observed long-term toxicity in the liver for the 7.4-MBq injected activity, as shown by an increase in ALAT and ASAT in mice in CR after day 100.
In this study, we demonstrated that CD138 was an excellent target for MM radioimmunotherapy and that the use of α-emitters was feasible when coupled to anti-mCD138 antibody. The survival study of treated animals showed that an injected activity of 3.7 MBq resulted in 60% survival at 300 d. The injected activity of 7.4 MBq, which gave 50% survival, was nevertheless associated with some signs of toxicity. The optimal activity of 3.7 MBq is coherent with data reported in the literature (37). At this activity, we did not observe any major hematologic toxicity, except for a minor effect on white blood cells. The overall amount of Flt3-L in the blood of patients during external radiotherapy correlates directly with both the cumulated radiation dose and the proportion of irradiated bone marrow (38). In this study, bone marrow toxicity, which was checked by measuring blood levels of Flt3-L, was also weak.
CONCLUSION
CD138 targeting with a mAb coupled to a radionuclide emitting α-particles represents a potential new therapeutic modality for MM consolidation treatment. The use of α-emitters with longer half-lives, such as 211At (7.2 h), should be evaluated to develop α-radioimmunotherapy of MM in the clinic.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported by grants from the TARCC contract no. Health-F2-2007-201962 that is supported by funding under the Seventh Research Framework Program of the European Commission and by grants from InCa (ACI 2007—Innovative delivery systems for cancer radionuclide therapy). No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication July 30, 2012.
- Accepted for publication March 14, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}