


Abstract
Whole-body PET/CT was used to characterize the radiation dosimetry of 11C-DPA-713, a specific PET ligand for the assessment of translocator protein. Methods: Six healthy control subjects, 3 men and 3 women, underwent whole-body dynamic PET scans after bolus injection of 11C-DPA-713. Subjects were scanned from head to mid thigh with 7 passes performed, with a total PET acquisition of approximately 100 min. Time–activity curves were generated in organs with visible tracer uptake, and tissue residence times were calculated. Whole-body dosimetry was calculated using OLINDA 1.1 software, assuming no voiding. Results: The absorbed dose is highest in the lungs, spleen, kidney, and pancreas. The lungs were determined to be the dose-limiting organ, with an average absorbed dose of 2.01 × 10−2 mSv/MBq (7.43 × 10−2 rem/mCi). On the basis of exposure limits outlined in the U.S. Food and Drug Administration Code of Federal Regulations (21CFR361.1), the single-dose limit for 11C-DPA-713 radiotracer injection is 2,487.6 MBq (67.3 mCi). Conclusion: 11C-DPA-713 has an uptake pattern that is consistent with the biodistribution of translocator protein and yields a dose burden that is comparable to that of other 11C-labeled PET tracers.
Translocator protein (TSPO), known formerly as the peripheral benzodiazepine receptor (PBR) (1), is established as an important marker of neuroinflammation in central nervous system disease or brain injury, as reviewed by various authors (2–5). Historically, the TSPO ligand used most commonly with PET is 11C-R-PK11195. Although it has been used successfully for numerous clinical studies, 11C-R-PK11195 has pharmacokinetic properties, such as high nonspecific binding, that are suboptimal for imaging. Given the importance of TSPO as a molecular target, in recent years there has been tremendous interest in developing an alternative radiotracer for PET (6–9). One such ligand is 11C-DPA-713 (10), which has been shown to have greater uptake and higher affinity than 11C-R-PK11195 (11). However, it has also been shown that 11C-DPA-713 is susceptible to multiple-affinity state binding (12,13). Nevertheless, 11C-DPA-713 shows promise as a prospective TSPO ligand; thus, we evaluated the radiation dose burden in healthy human control subjects after bolus tracer injection.
MATERIALS AND METHODS
Human Subjects
Six healthy volunteers (3 women, 3 men) were included in this study (Table 1). Subjects with a history of recent nosocomial infection, central nervous system lymphoma, neurologic disorder, structural central nervous system abnormality, head injury, or active substance abuse were excluded from participating. Female subjects were also screened and excluded for pregnancy. This study was approved by the Johns Hopkins Institutional Review Board. Subjects received an explanation of the purpose of the study, the study procedure, and associated risks and provided written informed consent before participation.
Summary of Subjects and Injected Dose of 11C-DPA-713
PET/CT Protocol
This study was performed under Investigational New Drug 78,283. 11C-DPA-713 was synthesized according to the procedures of Thominiaux et al. (14). Radiochemical purity was greater than 95%. A Discovery Rx VCT scanner (GE Healthcare), equipped with high-performance lutetium yttrium oxyorthosilicate PET crystals and a 64-slice CT component, was used. Subjects were positioned supine and imaged at rest. Before PET, a helical transmission CT scan (120 kVp; 20–200 mA, automatically adjusted) was acquired at each bed position. The CT scan was used for attenuation correction of the PET data and to delineate organ boundaries. 11C-DPA-713 (injected dose, 668 ± 21 MBq; specific activity, 668 ± 21 GBq/μmol; mass dose, 0.985 ± 0.13 μg) was delivered as a bolus via a catheterized vein over an approximately 30-s injection time. The catheter could not be accessed readily with the subject positioned in the field of view. Thus, after the CT scan, the patient bed was positioned to allow access to the catheter for radiotracer injection. The bed was then moved back (∼30 s) so that the PET acquisition was initiated about 1 min after radiotracer delivery. PET was performed using a sequence of 7 passes. For each pass, 8 or 9 contiguous single-bed-position PET images were acquired in 3-dimensional mode, with an 11-slice (5-mm) overlap. The scan durations per bed position for the 7 passes were 15, 30, 45, 60, 120, 240, and 240 s. PET images were reconstructed as described previously (15) using a 3-dimensional ordered-subset expectation maximization algorithm with 2 iterations, 21 subsets, a 3.0-mm postreconstruction gaussian filter, 4.7 × 4.7 mm (in-plane), and 3.27-mm (transaxial) voxels. To obtain images in Bq/mL, the scanner was calibrated with a 20-cm diameter, 20-cm-long 18F water phantom. The activity was measured using a dose calibrator that had been previously calibrated for 18F using a National Institute of Standards and Technology–traceable source.
Regions of Interest (ROIs)
ROI analysis was performed using Analyze 10.0 (Mayo Clinic Foundation) (16). Tissue ROIs were drawn on the standard regions used by OLINDA 1.1 (Vanderbilt University) for dosimetry calculation (17). To measure total disintegrations in gallbladder and urinary bladder contents, large ROIs were drawn to encompass the entire volume. For other organs, the regions were delineated by subsampling the organ, with care taken to ensure that the ROI included perceived regions of high radioactivity. Testes on male subjects and uterus, breast tissue, and ovaries on female subjects were identified. However, for 1 female subject (F2), ovaries could not be identified. To ensure a conservatively high dose estimate, the small intestine and stomach were subsampled by drawing ROIs that encompassed the organ wall and contents in slices of highest activity in each organ. Because 11C-DPA-713 does not accumulate in bone, it was assumed that all femoral radioactivity was located in red marrow. ROIs were not drawn on muscle, skin, or thymus. For the purpose of validating the use of subsampled ROIs, whole-organ ROIs were drawn for 2 subjects (F2 and M3). All ROIs were applied to the dynamic data to generate time–activity curves. Time–activity curves were generated without decay correction, and the acquisition time was taken to be the mid-point time of the bed acquisition that contained the region. There were 11 overlap slices for adjacent beds, in which case the acquisition time was taken to be the average of the mid-point times of the 2 beds. A complicating factor in determining the acquisition time precisely is that in some cases, particularly for whole-organ ROIs, regions extended across both single-bed and overlap regions, in which case the within-region radioactivity corresponds to 2 or more different time points. In that case, if most (>90%) of the region was located in a specific bed or overlap region, the corresponding time was used to generate the time–activity curves. If the region was split more evenly, then an average time weighted by the number of voxels at each bed or overlap region was used. In all subjects, we noticed that the catheter tubing and the site of catheter insertion were clearly visible throughout the study. This visibility indicates that some residual activity remained in the catheter and thus did not effectively enter the circulatory system. To determine the catheter residual, an ROI was drawn around the tubing and injection site. The total radioactivity remaining in the catheter was then compared with the total injected radioactivity, accounting for radioactive decay. The mean percentage activity remaining in the catheter was 2.4% ± 2.3%, with individual values ranging from 0.5% to 6.2%. For the purpose of dose normalization required for computing residence times, the injected 11C-DPA-713 radioactivity was adjusted by subtracting the measured catheter residual radioactivity. With subtraction of the catheter activity, the percentage injected dose to all organs is increased because the radiotracer uptake is attributed effectively to a smaller injected dose.
Residence Times and Absorbed Dose Calculations
To compute residence times, time–activity curves were expressed as percentage of the injected dose and then multiplied by the organ volume. We used sex-specific organ masses (adult women, adult men) that were provided in OLINDA and are based on a 56.9-kg woman and a 73.7-kg man. To convert standard organ mass to standard volume, each organ mass was divided by organ-specific tissue densities (18,19). After multiplying by the standard volumes, time–activity curves were integrated using trapezoidal integration up to the last measurement time point. Beyond the last time point, the integral to infinity was computed assuming exponential decay of 11C with a half-life of 20.3 min. The total sum integral for each organ is the residence time. For gallbladder contents and urinary bladder contents, instead of normalizing to standard volumes, total disintegrations were estimated from the large ROIs that were drawn about those regions. For dosimetry calculation, we made the most conservative assumption that the entire dose was deposited in tissue, thus giving the maximum possible residence time of 0.488 h (i.e., half-life/ln(2)) (ln(2) = 0.693 is the natural log of 2). The remainder-of-body radioactivity was thus computed as the sum of the residence times in all identified tissues, subtracted from 0.488. For each subject, the residence times were input to OLINDA using a sex-specific model (adult women, adult men), and the effective dose equivalent was based on the tissue-weighting factors recommended in International Commission on Radiological Protection (ICRP) publication 60 (20). We report mean ± SD of residence times and effective dose equivalent values averaged across all subjects. For comparison of dose estimates obtained with whole-organ and subsampled ROIs, we take the values obtained with whole-organ ROIs as the standard values and compute the percentage difference in the dose estimates obtained with subsampled ROIs.
RESULTS
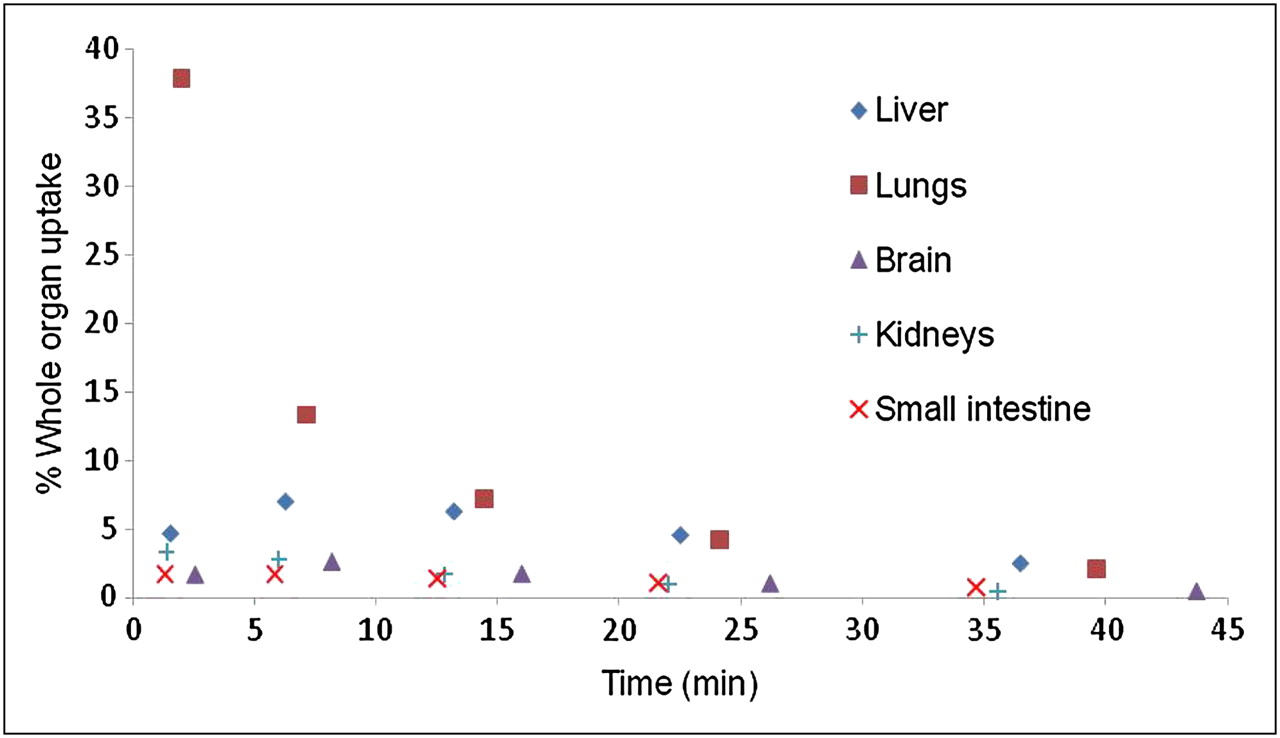
The whole-body biodistribution of 11C-DPA-713 is shown in 2-dimensional coronal projections in Figure 1. Tissue residence times are shown in Table 2, and the absorbed dose estimates are in Table 3. Figure 2 shows the whole-organ uptake curves expressed as a percentage of the injected dose; these are the curves that are integrated to compute residence times. The highest residence times were obtained in the lungs, liver, red marrow, brain, kidney, and small intestine. The highest absorbed doses were obtained in the lungs, spleen, kidney, pancreas, heart, and liver. For the 2 subjects (F2 and M3, Table 1) who had whole-organ ROIs drawn, the total-body dose estimates and the effective dose obtained using either whole-organ or subsampled ROIs agreed to within 1%. The effective dose equivalent obtained with either method agreed within 10% for both subjects (F2, 2.4%; M3, 9.0%), with subsampling giving the larger dose estimate. The individual organ dose estimates were also similar, with 75% of the organ doses agreeing to within 10% with either whole-organ or subsampled ROIs. Of particular importance to 11C-DPA-713 dosimetry is that the lungs were again determined to be the critical dose-limiting organ, with dose estimates using whole or subsampled regions agreeing to within 3% for both subjects (F2, 1.4%; M3, 2.3%).

Summed coronal 2-dimensional projections of tracer activity after bolus injection of 11C-DPA-713. Seven whole-body passes were performed as described. Images from left to right are from passes 1, 3, and 5 and show tracer biodistribution from 1 to 3, from 10 to 16, and from 28 to 42 min after injection, respectively. Images are displayed to same maximum. Lung uptake is prominent immediately after injection. Substantial tracer uptake is also observed in kidneys, spleen, liver, and brain.
11C-DPA-713 Residence Times in Measured Tissues (Hours)
Absorbed Dose Estimates After Bolus Injection of 11C-DPA-713
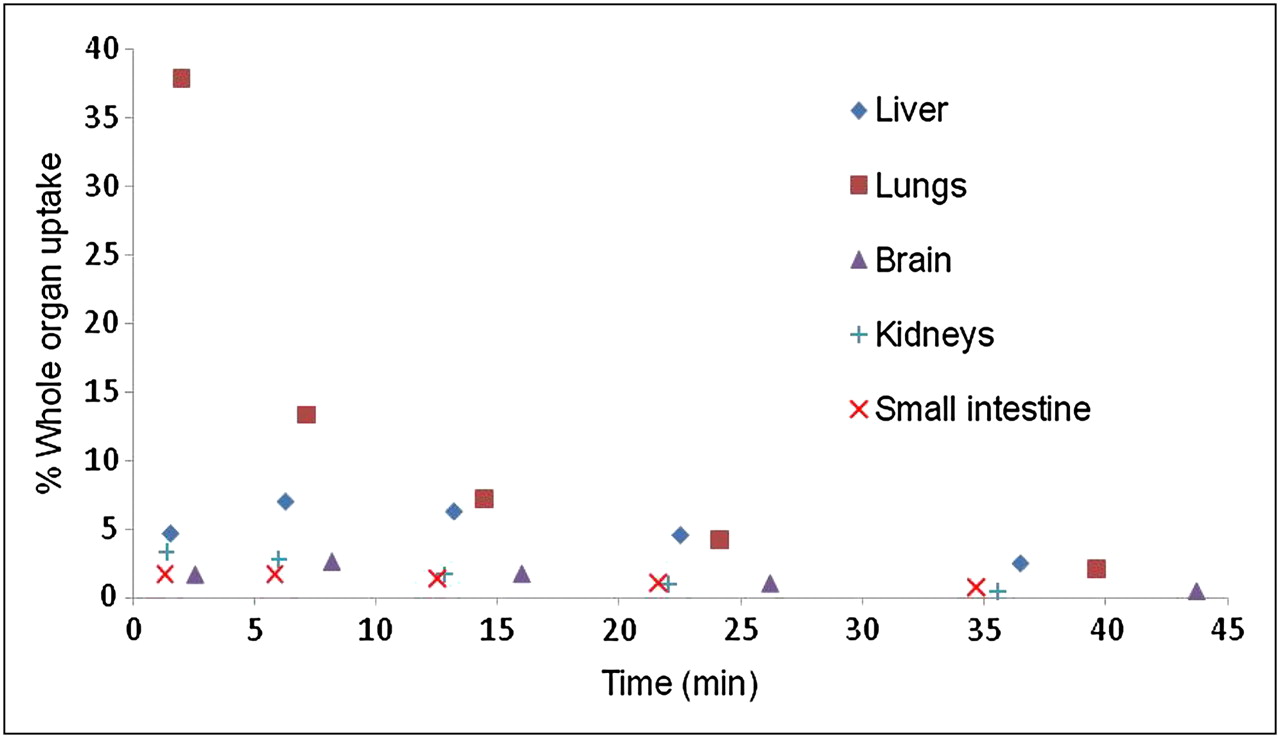
Whole-organ uptake after bolus injection of 11C-DPA-713. Values are total organ activity expressed as percentage of initial bolus activity. For each subject, 7 whole-body dynamic scans were obtained, with 8–9 bed positions that proceeded from thigh to head. Thus, brain was imaged in last bed position. Plot shows first 5 whole-body passes, and values reflect average of all 6 subjects. Both axes are averaged, because the postinjection scan times are slightly different for each subject.
DISCUSSION
The biodistribution of 11C-DPA-713 was found to be generally consistent with the known distribution of TSPO (21–23). The dosimetry is also similar to that of the TSPO ligand 11C-PBR28 (24), which is expected because 11C-DPA-713 and 11C-PBR28 have similar pharmacokinetics (11,25). In particular, for both 11C-DPA-713 and 11C-PBR28, the highest residence times were in the lungs and liver, and the highest absorbed doses were in the lungs, kidney, and spleen. For 11C-DPA-713, the lungs were determined to be the dose-limiting organ. On the basis of a single exposure limit of 5 rem (50 mSv), the single-administration dose limit is 2.49 GBq, or 67.3 mCi. A typical human PET study is performed with 555–740 MBq (15–20 mCi); thus, multiple tracer injections are possible, making test–retest and longitudinal studies quite feasible. The allowed dose limit is similar to that of other 11C-labeled radiotracers, and the effective dose of 11C-DPA-713 (5.9 μSv/MBq) is virtually at the median of 11C dosimetry values reported previously (as shown in Table 3 of Virta et al. (26) and also in Table 3 of Hirvonen et al. (27)).
Regarding tissues that are more radiation-sensitive, according to the Food and Drug Administration title 21 Code of Federal Regulations (CFR), part 361, only 3 rem are allowed in a single-dose administration to the whole body, active blood-forming organs, lens of the eye, and gonads (28). When needed for dosimetry reports, it is recommended that the brain dose be used as an estimate of the lens-of-eye dose. Even if the more stringent public lens-of-eye exposure (15 mSv) recommended by ICRP publication 103 (29) is applied, the single-dose limit is 4.49 GBq (121 mCi); thus, the lens of the eye is not dose-limiting relative to the lungs. The organ-weighting factors recommended in ICRP 103 (29) were not applied here, but it was found for 11C-R-PK11195 that the effective dose estimates obtained with either ICRP 60 or ICRP 103 weighting factors are nearly identical (27). 11C-DPA-713 is also nontoxic, because the no-observed-effect-limit dose is 49.3 μg/kg/d according to the SRI international study (30). At typical specific activity levels, approximately 1 μg is injected in a human study.
Drawing subsampled regions, as opposed to the time-consuming method of delineating whole-organ boundaries, is a practical approach to measuring activity in various organs (31–33). For the 2 subjects who were examined (F2 and M3) with whole-organ ROIs, the total-body dose and the effective dose were within 1% of the values obtained from subsampled ROIs. The lung dose was also quite similar, with subsampled ROIs yielding a 2% higher absorbed dose estimate. To further assess if subsampling was sufficient to quantify the dose to the critical organ, a whole-lung region was created for all subjects using the semiautomated ROI thresholding tool in Analyze (16). Lung residence times using the whole-lung ROIs were 6.1% less than the residence times obtained with subsampling; thus, the lung dose was not underestimated by subsampling.
To simplify the labor-intensive procedure of generating non–decay-corrected time–activity curves with acquisition times corresponding to specific bed positions, we attempted to perform the dosimetry with the time–activity curves decay-corrected to the start of each pass. In principle, that will yield the same residence time integral as non–decay-corrected data if there is negligible tracer redistribution from the start of the pass to the time of the specific bed acquisition. The benefit of decay correction to the start of each pass is that the activity throughout the body corresponds to the same time. That is, this procedure removes the ambiguity of the acquisition time when an organ is imaged in adjacent beds. In general, the dosimetry values were quite similar to those obtained without decay correction. However, for the lungs, performing the decay correction led to a consistent underestimation (>10%) in absorbed dose. Because the lungs are the critical organ, the result was a corresponding increase in the allowed dose limit. Thus, we used the non–decay-corrected results to ensure we obtained the most conservative, as well as the most accurate, dose estimate.
The biodistribution of 11C-DPA-713 is similar to that of other TSPO ligands, as is evident when comparing whole-body images of the present study (Fig. 1) with the corresponding figures for 11C-R-PK11195 (27) and 11C-PBR28 (24). However, in contrast to the present study that found the lungs to be the critical organ, for both 11C-R-PK11195 and 11C-PBR28 the critical organ was the kidneys, with the spleen receiving the next highest dose. A comparison of whole-body biodistribution showed that 11C-R-PK11195 has low lung uptake, compared with 11C-PBR28 (34); thus, it is not surprising that the lungs are not the critical organ for 11C-R-PK11195 dosimetry. On the other hand, 11C-PBR28 and 11C-DPA-713 share some similar properties, including similar affinity and lipophilicity (11). 11C-PBR28 and 11C-DPA-713 do, however, show differences in protein binding (11), pharmacokinetics of labeled metabolites (25), and sensitivity to multiaffinity state binding (12). Differences in methodology for dosimetry calculation may also contribute to the determination of different critical organs for 11C-PBR28 and 11C-DPA-713. For 11C-PBR28, it has been reported that the binding affinity affects dosimetry calculation (24). In particular, in a single subject with low binding affinity binding, there was a large decrease in dose to the spleen, kidney, and lungs, with a corresponding increased dose to the liver, gallbladder wall, and urinary bladder wall. Furthermore, the effective dose was reported to be 28% less. PBR28 has a particularly large ratio in TSPO binding affinity (50-fold) between low- and high-affinity states (12). 11C-DPA-713 has only a 4-fold ratio; thus, the impact of affinity on dosimetry estimates should be attenuated considerably. In the present study, on the basis of the consistency of tracer uptake in the brain and lungs, all subjects are believed to exhibit high-affinity binding. In principle, 11C-DPA-713 and 11C-PBR28 have favorable properties to be effective PET agents (11), although the presence of multiple-affinity-state binding has confounded efforts to demonstrate clearly that these tracers will improve on 11C-R-PK11195 for clinical investigation. Another TSPO ligand that may affect the future use of 11C-DPA-713 is the compound 18F-DPA-714, which has a similar chemical structure (35). 18F-DPA-714 has an inherent advantage for clinical use because of labeling with 18F, whereas 11C-DPA-713 is amenable to research protocols that call for multiple PET studies on the same day. Both 11C-DPA-713 and 18F-DPA-714 have been shown to give improved contrast over 11C-R-PK11195 in animal models of neuroinflammation (36,37). DPA-714 increases pregnenolone synthesis, which is indicative of a TSPO agonist, whereas DPA-713 has no effect and appears to be an antagonist (38). In that case, 11C-DPA-713 and 18F-DPA-714 have the potential to provide complementary information.
CONCLUSION
Absorbed dose estimates after 11C-DPA-713 bolus injection reveal the lungs to be the critical organ, yielding a single-injected-dose limit of 2,487.6 MBq (67.3 mCi). The dosimetry is consistent with other 11C tracers and indicates that multiple injections per year are easily allowable under current federal guidelines (21CFR361.1), especially given that typical radiotracer injections are no more than 740 MBq (20 mCi).
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
For radioisotope production, we thank the radiochemistry staff at the Johns Hopkins Nuclear Medicine PET Center, directed by Robert Dannals. We thank the PET/CT technologists for study preparation and image acquisition. We thank George Sgouros and Srinivasan Senthamizhchelvan for helpful comments and discussion. This study was supported by the JHU NIMH Toxicological Evaluation of Novel Ligands Program, NIH T32MH015330, NIH T32EB006351, and NIH R21MH082277. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 12, 2012.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication June 20, 2011.
- Accepted for publication September 12, 2011.





{kind=link}
{kind=link}