


Abstract
The purpose of this study was to assess the utility of 18F-FDG PET/CT for detection of inflammation in granulomatous sites and management of patients with chronic sarcoidosis. The 3 specific aims were to assess differences between 18F-FDG PET/CT and multidetector CT (MDCT) findings, to compare 18F-FDG PET/CT results with serum levels of angiotensin-converting enzyme (ACE), and to determine whether 18F-FDG PET/CT findings are associated with the decision to change therapy. Methods: We studied 90 sarcoidosis patients (mean age ± SD, 47 ± 12 y; 32 men and 58 women) with persistent symptoms who were referred for 18F-FDG PET/CT evaluation to assess the extent of inflammation. They also underwent MDCT and measurement of serum ACE level. After the follow-up (12 ± 5 mo after 18F-FDG PET/CT), the clinical status and changes in therapy were analyzed. Results: 18F-FDG PET/CT detected inflammation in 74 patients (82%) (maximum standardized uptake value, 8.1 ± 3.9). MDCT was positive for sarcoidosis in 6 additional patients (80, 89%). The difference between the 2 methods was not significant (P = 0.238, McNemar test), and their agreement was fair (κ = 0.198). Although ACE levels were significantly higher in patients with positive than negative 18F-FDG PET/CT results (P = 0.002, Mann–Whitney test), 38 patients (51%) with positive 18F-FDG PET/CT results had normal ACE levels. The therapy was initiated or changed in 73 out of 90 patients (81%). Both univariate and multivariate logistic regression analyses indicated that positive 18F-FDG PET/CT results were significantly (P < 0.001) associated with changes in therapy, with no contribution from age, sex, ACE level, CT results, or previous therapy. Conclusion: Our results indicate that 18F-FDG PET/CT is a useful adjunct to other diagnostic methods for detecting active inflammatory sites in chronic sarcoidosis patients with persistent symptoms, especially those with normal ACE levels. 18F-FDG PET/CT proved advantageous for determining the spread of active disease throughout the body and influenced the decision to adjust the therapy.
Sarcoidosis is a chronic granulomatous multiorgan disease of unknown etiology. It has a worldwide distribution and typically affects young to middle-aged white adults, with a higher incidence in women than men (1,2). The lungs and thoracic lymph nodes are most commonly involved (3). Extrathoracic manifestations are present in 25%–50% of the patients, typically in combination with thoracic disease (1). The diagnosis is confirmed by a histologic verification of noncaseating granulomas in the presence of typical clinical and radiographic findings and after exclusion of other granulomatous diseases. Various imaging techniques and the serum level of angiotensin-converting enzyme (ACE) produced by sarcoid granulomas are commonly used for evaluation and for planning of treatment (4). However, the ACE level is above normal limits in only about 60% of patients with chronic sarcoidosis and is unrelated to disease severity, progression, clinical course, and response to therapy (5).
Assessing the presence of granulomatous inflammatory activity and the extent of chronic sarcoidosis remains a challenge (6). Although important for detection and staging of pulmonary sarcoidosis, routine diagnostic procedures, such as chest radiography and multidetector CT (MDCT), are unable to reveal active inflammation (3,7). Nuclear medicine techniques, such as 67Ga scintigraphy and less often somatostatin receptor scintigraphy, have long been used for diagnosis and evaluation of the extent of disease (8,9). Nowadays, however, these are generally considered to play a limited role (8,10).
Recent advances in functional and molecular nuclear medicine imaging, such as 18F-FDG PET and 18F-FDG PET/CT, have broadened the spectrum of available methods for assessment of sarcoidosis (9,11,12). 18F-FDG PET is a well-established functional imaging technique for diagnosing cancer because it can detect increased glucose metabolism in the lesion (13). 18F-FDG PET also allows visualization of glucose metabolism in activated inflammatory cells (14–16). To date, however, the usefulness of 18F-FDG PET/CT for detection of inflammation in the granulomatous tissue of chronic sarcoidosis patients with persistent symptoms has not been thoroughly evaluated, particularly whether the results affect patient management (17–19).
The lack of reliable parameters for monitoring disease activity led to a hypothesis that 18F-FDG PET/CT may be useful for identifying patients with the active form of chronic sarcoidosis who exhibit persistent symptoms. Specifically, we postulated that the degree of activity and spread of disease may be more precisely assessed by 18F-FDG PET/CT than by MDCT. It was further assumed that the 18F-FDG PET/CT findings would provide new information to the clinicians, who might therefore consider adjusting the therapy. Thus, the objective of this study was to evaluate the utility of 18F-FDG PET/CT for detection of inflammation in granulomatous sites and subsequent management of chronic sarcoidosis in patients with persistent symptoms. The specific aims were to assess the difference between 18F-FDG PET/CT and MDCT findings, to compare 18F-FDG PET/CT with serum levels of ACE, and to determine whether 18F-FDG PET/CT findings are associated with subsequent changes in therapy.
MATERIALS AND METHODS
Study Population
This prospective study included 94 consecutive patients with chronic sarcoidosis who were referred for 18F-FDG PET/CT to the National PET Center at the Clinical Center of Serbia between January 2010 and May 2011. The eligibility criteria were chronic sarcoidosis confirmed by biopsy; presence of prolonged symptoms or new clinical, biochemical, or imaging findings suggestive of active disease; no evidence of cancer or other diseases that resemble sarcoidosis on MDCT and PET/CT (Wegener syndrome, tuberculosis, aspergillosis); and glucose level no greater than 11 mmol/L (20). Of 94 referred patients, 4 were excluded because of the detected cancer (2 Hodgkin lymphoma, one lung cancer, and 1 rectal carcinoma). Thus, the final sample consisted of 90 patients (mean age ± SD, 47 ± 12 y, 32 men and 58 women).
Procedures
Before 18F-FDG PET/CT, the subjects underwent standard radiography and high-resolution CT of the chest and serum measurement of ACE level (reference range, 8–52 U/L). The referring physicians first reviewed all results except the 18F-FDG PET/CT report. They were then asked to make a note about the suggested therapy. After reviewing the 18F-FDG PET/CT report, the physicians were asked to make a final decision about the therapy. The choice of therapy was at the discretion of each physician. The patients returned for follow-up 12 ± 5 mo after 18F-FDG PET/CT, at which point the information about the current symptoms was recorded. After the follow-up, clinical, imaging, and laboratory data were extracted from the medical records. The medication initially suggested and finally prescribed before and after the 18F-FDG PET/CT results had been considered was collected. The study protocol was approved by the Ethics Committee of the Faculty of Medicine of the University of Belgrade, and written inform consent was obtained.
Data Acquisition, Reconstruction, and Image Analysis
The patients underwent 18F-FDG PET/CT examination on a 64-slice hybrid PET/CT scanner (Biograph; Siemens Medical Solutions USA Inc.). They fasted for 8 h before receiving an intravenous injection of 5.5 MBq of 18F-FDG per kilogram. PET/CT acquisitions started 60 min after tracer injection. A 3-dimensional PET scan (6–7 fields of view, 3 min/field) and low-dose nonenhanced CT scan were acquired from the skull to the mid thigh. If deemed necessary, a total-body study was also performed. MDCT was acquired with 120 kV and with automatic, real-time dose-modulation amperage (CareDose4D [Siemens], with the baseline being 45 mA); a slice thickness of 5 mm; pitch of 1.5; and a rotation time of 0.5 s. CT, PET (attenuation-corrected), and combined PET/CT images were displayed for analysis on a syngo Multimodality Workplace (Siemens AG).
18F-FDG PET/CT findings were scored as positive or negative for inflammation. The findings were considered positive in cases of increased 18F-FDG uptake above the level in blood vessels in the mediastinum or lung parenchyma, or in extrathoracic sites, including lymph nodes, visceral organs (parotid gland, liver, spleen), nasopharynx, skin, muscle, or bone (18). Quantitative analysis of 18F-FDG uptake in the lesion was based on maximum standardized uptake value per focus. This value was calculated as the activity concentration measured at the end of the scan and corrected for individual body weight and dose injected, as follows: tissue activity (counts/pixel/s) multiplied by calibration factor divided by injected 18F-FDG dose (MBq/kilogram of body weight) (20). 18F-FDG PET/CT data were interpreted separately by 3 investigators: 2 nuclear medicine physicians and a radiologist. Consensus was reached in cases of discrepancy.
Statistical Analysis
The difference between MDCT and 18F-FDG PET/CT findings was tested by the McNemar test, and the κ-coefficient was used to determine agreement between the 2 methods. The Mann–Whitney U test was used to evaluate whether ACE levels were different between patients with negative and positive 18F-FDG PET/CT results. Univariate and multivariate logistic regression analyses were conducted to determine whether changes in therapy during follow-up were associated with sex, age (≤35 vs. > 35 y), serum level of ACE (abnormal vs. normal), or 18F-FDG PET/CT and MDCT results (positive vs. negative).
In secondary analyses, the relationship between 18F-FDG PET/CT results and a change in treatment among patients with a normal ACE serum level was evaluated with the Fisher exact test. Also, the Cox proportional hazards regression model was used to determine whether sex, age, and ACE level were associated with the presence of more pronounced symptoms in patients with positive 18F-FDG PET/CT findings. The results were presented as mean ± SD, and a P value of less than 0.05 was considered significant.
RESULTS
Patient Characteristics
The demographic and clinical characteristics of the 90 patients are given in Table 1. All were nonsmokers. The mean duration of the disease was 6 ± 3 y (range, 3–25 y). Most patients complained of more than one symptom, including fatigue (33%), bone pain (22%), cough (18%), headaches (13%), chest pain (12%), and fever (2%). Lung function tests showed a broad range of findings that were on average below the normative values, including a forced expiratory volume in 1 s of 83% ± 7% (range, 43%–127%), a forced vital capacity of 93% ± 4% (range, 50%–153%), and a carbon monoxide diffusing capacity of 83% ± 13% (range, 41%–107%).
Summary of Demographic and Clinical Characteristics of the 90 Patients According to PET/CT and MDCT Results
18F-FDG PET/CT Findings in Comparison to Other Tests
18F-FDG PET/CT detected active sarcoidosis in 74 patients (82%), with a mean maximum standardized uptake value of 8.1 ± 3.9 (range, 2.8–23.9). MDCT detected sarcoidosis in 6 additional patients (89%). The CT portion of the 18F-FDG PET/CT examination in these 6 patients revealed bilaterally enlarged hilar lymph nodes (stage 1 sarcoidosis; size, 12–28 mm) but without increased accumulation of 18F-FDG (Table 2). Despite disagreement between the 2 methods in stages 1 and 2 (Table 2), the difference was not statistically significant (P = 0.238, McNemar test). Agreement between 2 methods was fair (κ = 0.198).
Imaging Results and ACE Level in Patients with Sarcoidosis
The disease was limited to the thorax in 69 patients (77%) and was both thoracic and extrathoracic in 30 patients (33%) (Fig. 1). Isolated extrathoracic sarcoidosis was found in 5 patients only on 18F-FDG PET/CT. Retroperitoneal and cervical lymph nodes were the most frequent extrathoracic sites found on 18F-FDG PET/CT, followed by skin, parotid gland, and adrenal glands (Table 3).

Maximum-intensity-projection 18F-FDG PET/CT findings in patient with chronic active sarcoidosis. Multiple sites of increased 18F-FDG uptake are seen in mediastinal and retroperitoneal lymph nodes, liver, and spleen.
Most Common Sites of Extrathoracic Sarcoidosis on 18F-FDG PET/CT Scans
The ACE level was significantly higher in patients with positive than negative PET/CT findings (P = 0.002, Mann–Whitney U test) (Fig. 2). Moreover, 18F-FDG PET/CT findings were positive in 38 of 51 patients (75%) with normal ACE levels (Table 2).
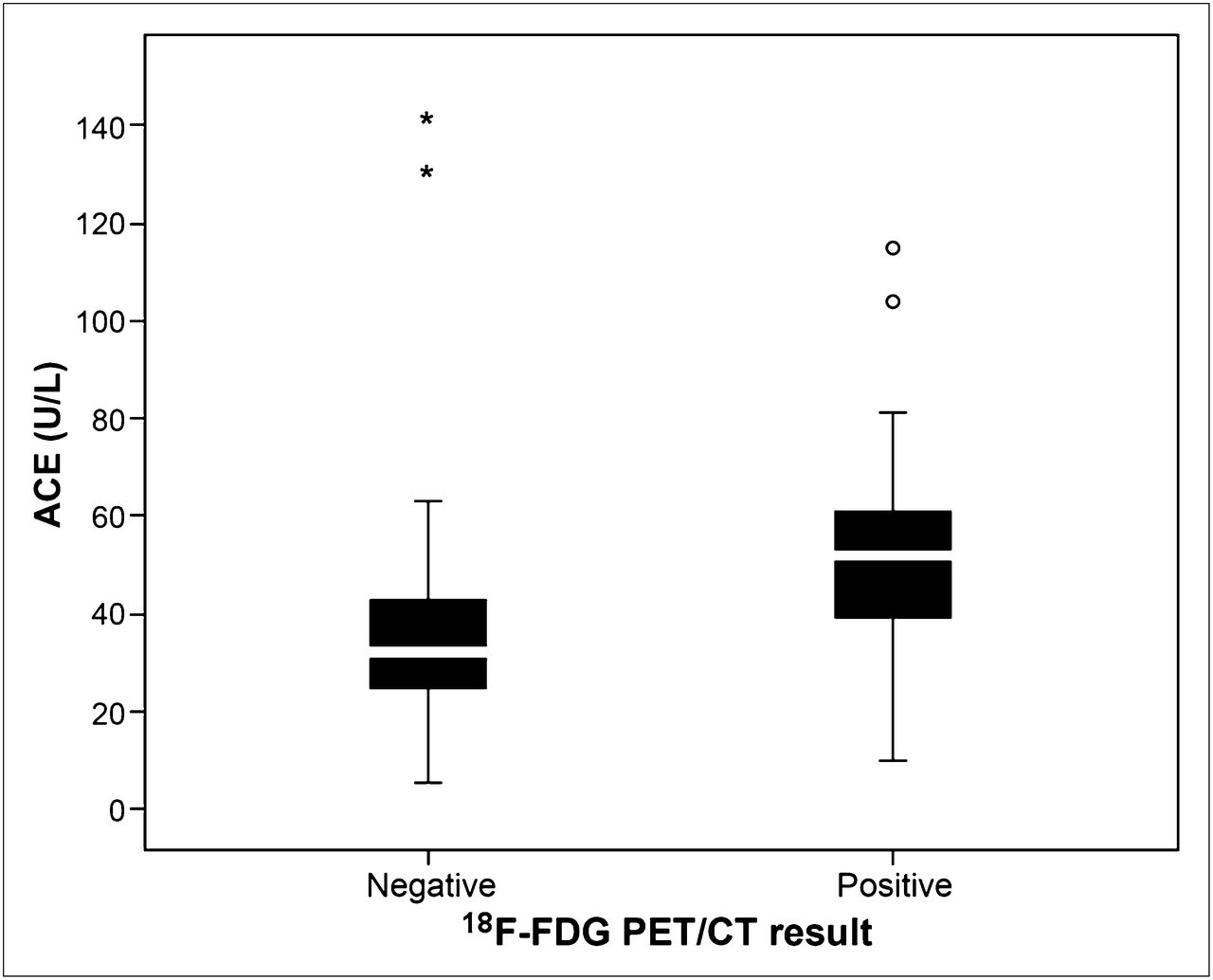
ACE serum levels for patients with negative and positive 18F-FDG PET/CT findings. Boxes and whiskers denote 5th, 25th, 50th, 75th, and 95th percentiles, with outliers indicated.
Relationship Between 18F-FDG PET/CT and Follow-up Findings
Clinical management changed in 73 patients (81%) over the course of follow-up, for whom either the previous treatment was modified or a new treatment was introduced (Table 4). In most patients with positive 18F-FDG PET/CT results, higher doses of only corticosteroids or of corticosteroids and methotrexate were introduced. In only 1 patient was the existing corticosteroid dose (20 mg/d) decreased because of side effects. On the other hand, in most patients with negative 18F-FDG PET/CT results, the existing dose was reduced or therapy was discontinued. Among the patients with normal ACE levels (n = 51), the therapy was changed significantly more often for those who showed positive 18F-FDG PET/CT findings (n = 33, 65%; P = 0.003, Fischer exact test) (Table 5).
Clinical Management After 18F-FDG PET/CT Examination
Clinical Management of Patients with Normal ACE Serum Levels
Both univariate (odds ratio, 13.47; 95% confidence interval, 3.89–46.59; P < 0.001) and multivariate (odds ratio, 17.1; 95% confidence interval, 3.89–74.60; P < 0.001) logistic regression analyses revealed that positive 18F-FDG PET/CT results were significantly associated with a change in therapy over the course of follow-up (Table 6), with no impact from age, sex, CT findings, ACE level, or presence of therapy.
Variables and Their Significance in Predicting Change in Therapy
At follow-up, 42 patients (47%) reported no or less pronounced symptoms, 38 (42%) had the same symptoms, and 10 (11%) had more pronounced symptoms. Cox regression multivariate analysis showed that only older patients with positive 18F-FDG PET/CT findings had more pronounced symptoms (hazard ratio, 1.03; 95% confidence interval, 1.00–1.05; P = 0.030) without an impact from other variables (sex, ACE level).
DISCUSSION
This study revealed new findings about the utility of 18F-FDG PET/CT for diagnosis and management of patients with chronic sarcoidosis. First, 18F-FDG PET/CT detected active inflammatory lesions in 82% of patients with persistent symptoms, including many in extrathoracic sites. Second, although ACE levels were on average higher in patients with positive 18F-FDG PET/CT results, in almost half these patients ACE fell within normal limits. Finally, positive 18F-FDG PET/CT results were significantly associated with the decision to adjust the therapy.
The assessment of inflammatory activity in chronic sarcoidosis patients with persistent symptoms remains a challenge due to the lack of a gold standard (21). The goal is to detect and quantify the degree of inflammatory and granulomatous reactions in the lungs and elsewhere in the body. This study demonstrated that this goal can successfully be achieved with 18F-FDG PET/CT because it detected one or more sites of active inflammation in 82% of our patients. Active inflammation on 18F-FDG PET/CT was found in the thorax in most patients, as agrees with previous studies (18,22,23). However, pulmonary infiltrates and their distribution are usually better visualized on MDCT. A more detailed examination of the lung parenchyma can help differentiate whether the disease has a predominantly vascular, airway, or lymphatic distribution or remains limited to the interstitial tissue. Although MDCT is informative about disease distribution, the findings do not correlate better than radiography findings with clinical and functional impairment in sarcoidosis (24).
Despite fair agreement between the 18F-FDG PET/CT and MDCT findings in this study, 18F-FDG PET/CT appeared to be superior in detecting previously unknown sites of inflammation. The agreement between the 2 methods can be ascribed to the fact that most of our patients had already-known lung disease detected on both18F-FDG PET/CT and MDCT. However, nodular opacities, lung consolidation, and ground glass opacity on MDCT may represent granulomatous inflammation, fibrosis, or a combination of both (25). The 18F-FDG PET/CT scan revealed previously unrecognized active sites of disease in bone, the retroperitoneum, the cervical region, the spleen, and the liver in 18% of patients. Such an increased diagnostic yield closely corresponds to the results of Teirstein et al., who found occult sites on 18F-FDG PET in 15% of patients that went undetected clinically or by conventional radiography and MDCT (22). An even higher prevalence (34%) of bone and bone marrow involvement undetected on CT has been reported (26). The additional information provided by 18F-FDG PET/CT is likely to influence clinical management.
Interstitial pneumonitis with infiltration of macrophages and lymphocytes represents an initial lesion in pulmonary sarcoidosis followed by the appearance of characteristic epithelioid granulomas. ACE produced by the granuloma is considered to reflect the degree of inflammation (27). Thus, serum ACE level is the most commonly used marker of inflammation in sarcoidosis, with a sensitivity between 34% and 77% (28–30). In our study, ACE levels were significantly higher in patients with positive than negative 18F-FDG PET/CT findings. It has previously been shown that a rising level of ACE in serum is associated with worsening clinical status and positive findings on 67Ga scans (31). However, almost half our patients with positive 18F-FDG PET/CT findings showed ACE levels within normal limits. These results support the recent findings of Mostard et al. (18) that the negative predictive value of ACE is only moderate (65%). That is, normal ACE levels do not exclude the existence of active inflammatory sites. Therefore, 18F-FDG PET/CT examination seems particularly useful for patients with negative ACE results because detection of inflammatory activity in such patients is expected to affect clinical decision making.
Several published case reports and small case series indicate the usefulness of 18F-FDG PET and 18F-FDG PET/CT for monitoring the effect of therapy in patients with sarcoidosis (19,32–34). To our best knowledge, however, this was the first prospective study to specifically address the association between 18F-FDG PET/CT results and subsequent patient management. Our follow-up data revealed that in 81% of the patients a new therapy was initiated or the existing therapy was changed. In the multivariate analysis, which included several potentially relevant variables, positive 18F-FDG PET/CT findings emerged as the only significant predictor of a change in therapy during follow-up. Elimination of MDCT in the model can be ascribed to a partial overlap with the results of 18F-FDG PET/CT, as documented by the lack of a significant difference between the 2 imaging methods. On the other hand, the differential sensitivity of MDCT and 18F-FDG PET/CT for detecting sarcoid lesions should also be considered. MDCT was superior in stages 1 and 2, whereas 18F-FDG PET/CT was better at picking up the active granulomatous sites in bones, liver, spleen, and retroperitoneal lymph nodes. The overall results suggest that the clinicians were more inclined to change the therapy when the disease was spread throughout the body, as could be detected only with 18F-FDG PET/CT. Although the presence of distortion, cysts, or bronchiectasis on CT has been associated with a poor response to therapy (35), less reliance on CT in our study may also be explained by recent doubts of whether CT can reliably predict disease outcome and response to therapy (36).
We recognize that the decision to change therapy on the basis of 18F-FDG PET/CT results may have been confounded by the relatively recent introduction of this technique at our institution. However, several previously discussed findings support the assertion that the clinicians took the 18F-FDG PET/CT results in earnest when considering changes in therapy. First, 18F-FDG PET/CT showed an advantage over standard radiography and MDCT for detecting extrathoracic sites of inflammation. Second, 18F-FDG PET/CT detected active sites in a large proportion of patients with normal ACE levels. Last, 18F-FDG PET/CT findings were frequently positive in older patients with more pronounced symptoms and provided further justification to adjust the therapy.
This study had several limitations. Because no single test is available to accurately assess the presence of inflammatory activity in chronic sarcoidosis, our results could not be validated against the gold standard. In the absence of a gold standard, we compared the results against the serum level of ACE, which is considered a marker of inflammation in sarcoidosis despite its shortcomings. Of further interest might be to correlate the results of histopathology, imaging, and serum ACE levels—a correlation that was not done here. Another potential limitation was the relatively short follow-up. The finding that half our patients were still symptomatic despite changes in therapy can be explained by the fact that it may take up to 2 y to favorably respond to corticosteroid treatment (37,38). Thus, it remains to be seen whether the apparent association between the 18F-FDG PET/CT findings and the decision to change therapy altered the course of disease or affected quality of life in patients with chronic sarcoidosis.
CONCLUSION
This study revealed that 18F-FDG PET/CT is a useful technique for detecting active inflammatory sites in patients with chronic sarcoidosis and prolonged symptoms, especially in elderly patients with persistent symptoms and those with normal ACE levels. The 18F-FDG PET/CT results provided relevant new information about the spread of active disease that influenced the decision to change therapy. Further studies should determine the long-term impact of 18F-FDG PET/CT results on clinically meaningful outcomes in patients with chronic sarcoidosis.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
This work was supported by the Serbian Ministry of Education and Science (grants 175018, 175046, and 175081). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 9, 2012.
- © 2012 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication February 13, 2012.
- Accepted for publication May 15, 2012.





{kind=link}
{kind=link}