


Abstract
The aim of our retrospective study was to assess the incidence of increased uptake of 68Ga-DOTANOC in the head of the pancreas among a large population of patients with extrapancreatic neuroendocrine tumors studied with serial 68Ga-DOTANOC PET/CT. Methods: Patients who had undergone at least two 68Ga-DOTANOC PET/CT studies over time were included. Uptake in the head of the pancreas was measured and compared with uptake in normal liver parenchyma (target-to-liver ratio). Patients were followed up for 6–24 mo. Results: We reviewed 245 studies performed on 100 patients and classified the pancreatic uptake as either diffuse or focal. Twenty-three patients (66 scans) showed diffuse uptake; 8 patients (16 scans) showed focal uptake. None of these 31 patients had negative findings on their subsequent scans, and vice versa. During follow-up, localization of neuroendocrine tumors in the pancreas was not suspected in any patient. Conclusion: Focal and diffuse uptake of 68Ga-DOTANOC in the head of the pancreas occurred, respectively, in 23% and 8% of the patients. The main finding of our study was that increased pancreatic uptake was stable over time.
The introduction of β-emitter 68Ga-radiolabeled peptides (68Ga-DOTA peptides) has been giving promising results in the field of neuroendocrine tumor (NET) imaging, with a direct impact on clinical management (1–5).
68Ga-DOTANOC is a somatostatin analog radiotracer that, compared with other 68Ga-DOTA peptides, shows improved affinity to somatostatin receptor (SSTR) type 2 and high affinity to types 3 and 5 (6–8). 68Ga-DOTANOC PET/CT has been used for staging, restaging, controlling therapy, and detecting unknown primary tumors in patients with NET (9–11). Compared with other radiopharmaceuticals, such as 18F-FDG and 18F-3,4-dihydroxyphenylalanine (12–14), or other conventional imaging methods, such as CT or bone scanning (15,16), 68Ga-DOTANOC has proved to be more accurate in the diagnosis of NET.
The pancreas carries all the SSTR subtypes on the acinar and islet cellular surface (17). However, pancreatic tissue usually does not show significantly increased uptake of 68Ga-DOTANOC. Some cases of increased uptake of 68Ga-DOTA peptides in the pancreas have been sporadically reported (11,18), but to our knowledge this finding has never been deeply investigated.
The aim of our retrospective study was to assess the incidence and characteristics of increased uptake of 68Ga-DOTANOC in the head of the pancreas among a large population of patients with extrapancreatic NET studied with sequential 68Ga-DOTANOC PET/CT.
MATERIALS AND METHODS
We retrospectively reviewed the 68Ga-DOTANOC PET/CT studies of 100 patients (60 men and 40 women; age range, 35–78 y) with NET not involving the pancreas. The 245 studies were performed between March 2007 and April 2010. To evaluate the variation of uptake within the same patient, we included only patients who had undergone at least 2 scans over time (range, 2–6 scans per patient; time between scans, 3–36 mo). 68Ga-DOTANOC PET/CT was performed for restaging in 67 patients, therapy monitoring in 15 patients, staging in 11 patients, and localizing an unknown primary NET in 7 patients.
The inclusion criteria were pathologic confirmation of extrapancreatic NET and a previous CT or MRI scan showing normal pancreatic density without evidence of disease in the head of the pancreas.
68Ga-DOTANOC was synthesized by the radiopharmacy of our nuclear medicine unit. 68Ga was eluted from a 68Ge/68Ga generator (Eckert and Ziegler), and DOTANOC (ABX) was labeled with 68Ga following the procedure described by Zhernosekov et al. (19) and according to the recommendations of the European Association of Nuclear Medicine on good radiopharmacy practice in the preparation of radiopharmaceuticals (20).
68Ga-DOTANOC PET/CT (administered dose, 1.5–2 MBq/kg; uptake time, 50–70 min after injection) was performed on a dedicated hybrid scanner (Discovery STE or Discovery LS; GE Healthcare). PET emission images were recorded for 4 min/bed position from the skull base to the mid thigh. The CT attenuation-correction acquisition parameters were 140 kV, 90 mA, a 0.8-s tube rotation, and a 5-mm slice thickness. The images were retrospectively evaluated by 3 independent readers. Disagreements were discussed, and a final diagnosis was reached by consensus. The readers reported the presence of any increased uptake in the head of the pancreas, the intensity and shape (faint/intense; focal/diffuse) of the radiotracer uptake, and any variation in uptake over time. Uptake in the head of the pancreas was measured using maximal standardized uptake value (SUVmax) and compared with uptake in normal liver parenchyma (target-to-liver ratio) for each scan. Patients were followed up for 6–24 mo after the last 68Ga-DOTANOC PET/CT scan.
RESULTS
After reviewing the images, we retrospectively classified 2 different uptake patterns in the pancreas. The first was a pattern of diffuse, homogeneous uptake involving the pancreatic uncus and the head of the pancreas proximal to the duodenum. This finding was usually elongated longitudinally. The second was a pattern of focal, intense uptake that usually was small and localized in the inferior aspect of the head of the pancreas (pancreatic uncus). The diffuse pattern (23 patients; 66 scans) was seen much more frequently than the focal pattern (8 patients; 16 scans) (Table 1).
Summary of Results on Patient and Scan Basis
Interestingly, none of the patients with increased pancreatic uptake, either focal or diffuse, had subsequent scans negative for uptake, and vice versa: the 69 patients with negative findings continued to have negative findings over time, the 23 patients showing a diffuse pattern continued to show a diffuse pattern over time, and the 8 patients showing a focal pattern continued to show a focal pattern over time. No significant differences in age, sex, location of primary tumor, or administration of any kind of therapy were observed between patients with and without increased uptake. For the diffuse pattern, the target and liver had a similar mean SUVmax (5 ± 1.6 for target and 6.3 ± 2.1 for liver; target-to-liver ratio, 0.8), whereas for the focal pattern, the mean SUVmax was higher for target than for liver (12.6 ± 2.2 for target and 6.4 ± 1.5 for liver; target-to-liver ratio, 1.9). No significant changes in target-to-liver ratio were seen over time in patients with either a focal or a diffuse pattern (Table 2).
Pancreatic SUVmax and Target-to-Liver Ratio in Scans Positive for Uptake
During follow-up (6–24 mo), localization of NET in the head of the pancreas was not suspected in any patient.
DISCUSSION
Usually, and in most patients, the normal biodistribution of 68Ga-DOTA peptides in the pancreas appears as a faint, almost undetectable, uptake along the head, body, and tail of the organ. Only a few studies have described unusually increased uptake of 68Ga-DOTA peptides in the pancreas. Gabriel et al. (11) described an increased uptake of 68Ga-DOTATOC in the head of the pancreas in 57 of 84 patients, but the authors did not mention whether they observed differences in the intensity of the uptake. Prasad et al. (18) saw this finding using 68Ga-DOTANOC but did not report how frequent the finding was.
In the pancreas, SSTR distribution differs between exocrine and endocrine cells: although islet cells express more of SSTR types 2A, 2B, 1, and 3, acinar cells lightly express more of types 5 and 4 (17). Because 68Ga-DOTANOC has a high affinity for SSTR types 2, 3, and 5, it is more likely that 68Ga-DOTANOC labels islet cells in the pancreas.
After reviewing the images, we grossly classified pancreatic uptake into 2 patterns: faint and diffuse or intense and focal. The diffuse pattern was relatively frequent (23% of patients), whereas the focal pattern was rare (8%). We observed a clear dichotomy in the intensity of pancreatic uptake (Table 2). In our opinion, it is not possible to prove whether the differences between the 2 groups are caused by 2 distinct mechanisms or are an expression—with different intensity—of the same mechanism. It seems more probable that only one mechanism could be the cause of this finding. However, answering this question exceeds the purpose of the present study.
The most relevant finding—and one that has not, to our knowledge, yet been described—was that the increased uptake or its absence was stable in all patients over time. Whatever the management of the patient, patients showing no increased uptake in the pancreas continued to show no increased uptake over time, and patients showing increased uptake showed stability in that uptake over time regardless of the pattern (Table 2). Therefore, this observation was due to stability in increased expression of SSTR types 2, 3, or 5 in that particular region of the organ and not to any functional and transient cause. Moreover, focal or diffuse increased uptake has never, to our knowledge, been described other than in the head or uncinate process of the pancreas. In the present large series of patients, we did not obtain histologic findings through biopsy or surgery because there was no clinical or biochemical parameter prompting the clinicians to perform it. However, over a prolonged follow-up of 24 mo, the multiple 68Ga-DOTANOC PET/CT examinations showing a stable picture in the pancreas, and the absence of biochemical and clinical symptoms, appear to indicate that the diffuse and even focal uptake is likely due to physiologic variability in SSTR expression by pancreatic endocrine cells and to variability in their anatomic distribution in the organ (diffuse vs. focal uptake). Awareness of this physiologic variability in SSTR expression and endocrine cell distribution within the pancreas is of paramount importance for correct interpretation of 68Ga-DOTANOC PET/CT findings, especially to avoid misdiagnosis of a tumor in a patient with physiologic focal uptake in the head of the pancreas. Prasad and Baum (18) suggested an SUVmax cutoff of 8.6 to discriminate between the presence of cancer and the presence of physiologic or nonneoplastic uptake in the pancreas. In our series, the application of this cutoff would have led to erroneous interpretation of neoplastic locations in sixteen 68Ga-DOTANOC PET/CT scans (8 patients) that had an SUVmax above this threshold. We believe, on the contrary, that not only the intensity of the uptake but also its site and shape, as well as the likelihood of NET localization in the head of the pancreas, should be considered in order to correctly interpret the finding. We suggest that visual analysis of this finding be done with care (Figs. 1–4⇓⇓⇓), and we strongly recommended that PET/CT readers report with caution every area of increased 68Ga-DOTANOC uptake in the head of the pancreas.
Faint and diffuse pattern: 64-y-old man with ileac NET resected in 2006. (A) 68Ga-DOTANOC PET/CT performed in March 2008. Typical faint and diffuse pattern is seen, with longitudinally elongated area involving head and uncinate process of pancreas. SUVmax of target is 5.0, SUVmax of liver is 5.0, and T/L ratio is 1.0. (B) 68Ga-DOTANOC PET/CT performed in April 2010. Finding in head of pancreas is substantially unchanged. SUVmax of target is 4.5, SUVmax of liver is 4.5, and T/L ratio is 1.0.
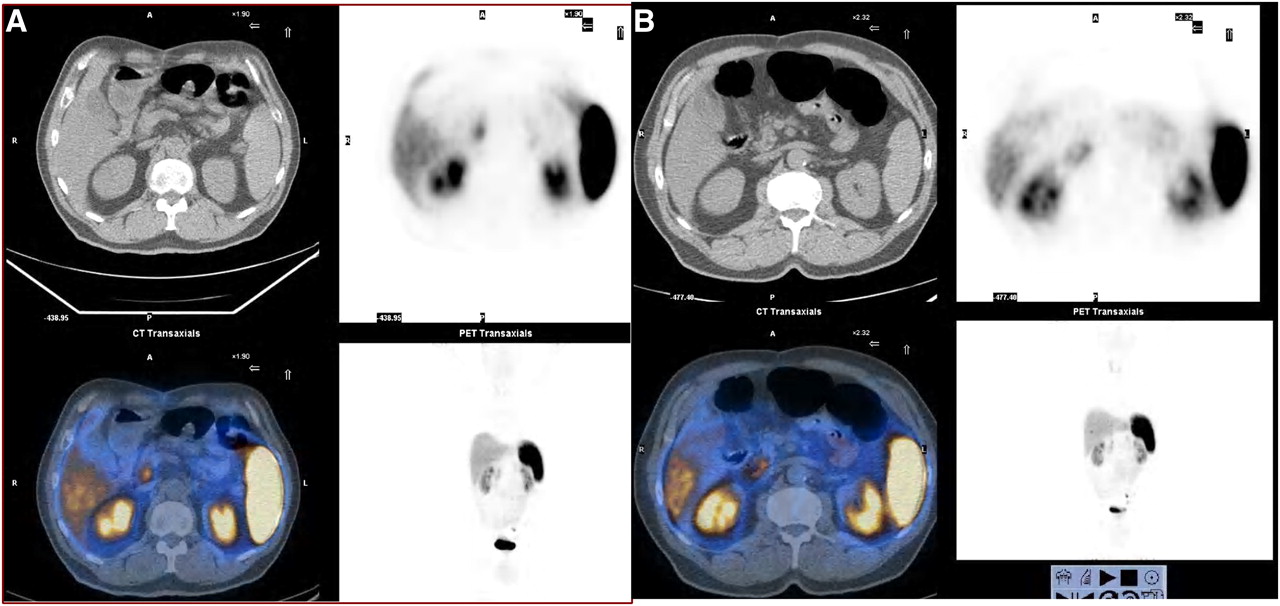
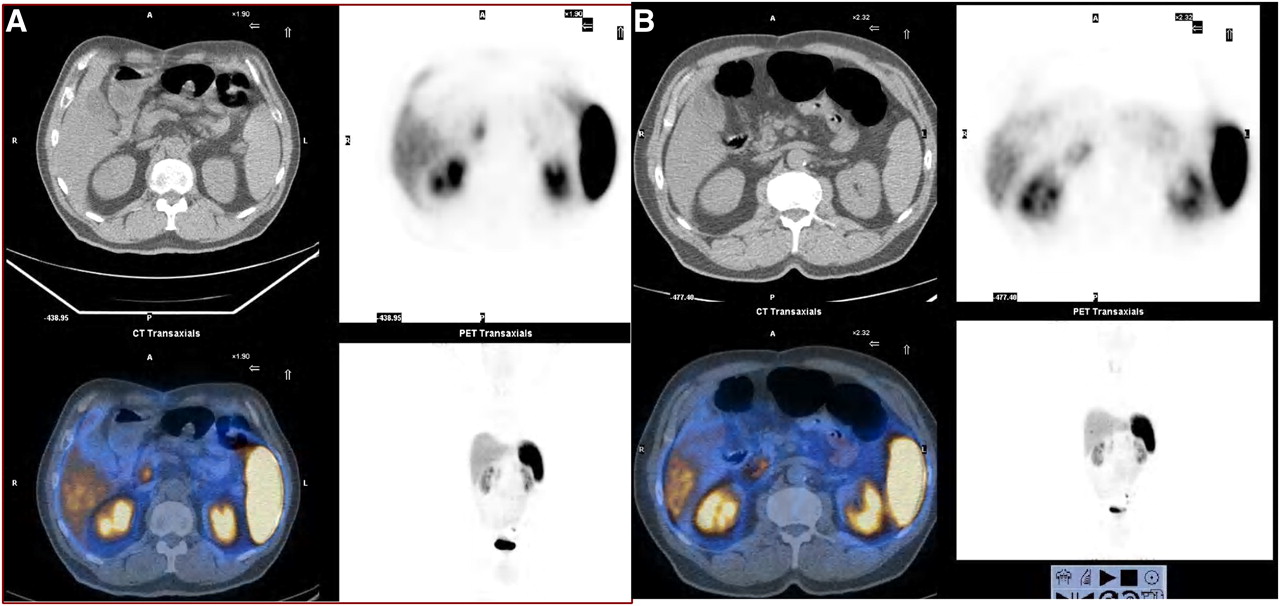
Focal and intense pattern: 46-y-old woman with pulmonary NET resected in 2005. (A) 68Ga-DOTANOC PET/CT performed in January 2009. Area of increased uptake is relatively small and round and involves only uncinate process of pancreas. SUVmax of target is 10.5, SUVmax of liver is 6.0, and T/L ratio is 1.7. (B) 68Ga-DOTANOC PET/CT performed in September 2009. Finding in head of pancreas is substantially unchanged. SUVmax of target is 10.0, SUVmax of liver is 5.9, and T/L ratio is 1.7.

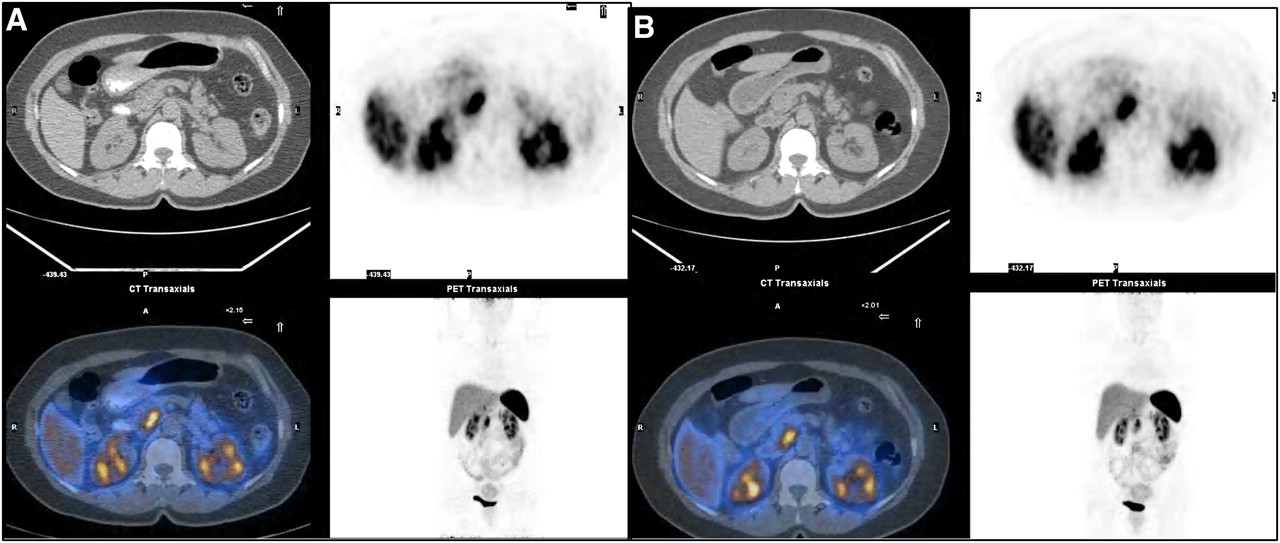
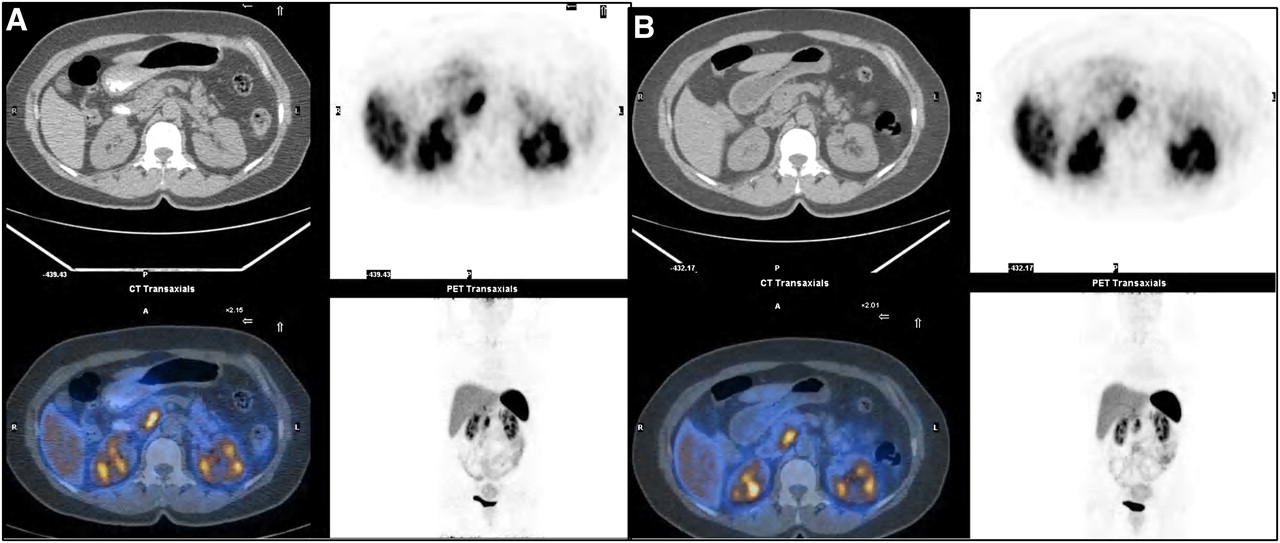
Focal and intense pattern: 67-y-old man with gastric NET resected in 2005. (A) 68Ga-DOTANOC PET/CT performed in May 2007. Area of increased uptake is relatively small and involves uncinate process only. SUVmax of target is 9.5, SUVmax of liver is 5.0, and T/L ratio is 1.9. (B) 68Ga-DOTANOC PET/CT performed in July 2009. Finding in head of pancreas is substantially unchanged. SUVmax of target is 11.2, SUVmax of liver is 7.0, and T/L ratio is 1.6.

Faint and diffuse pattern: 35-y-old woman with appendicular NET resected in 2008. (A) Maximum-intensity projection of 68Ga-DOTANOC PET/CT performed in October 2008. Large, longitudinally elongated area involving whole head of pancreas is evident. SUVmax of target is 7.2, SUVmax of liver is 6.0, and T/L ratio is 1.2. (B) Maximum-intensity projection of 68Ga-DOTANOC PET/CT performed in February 2010. Shape of finding in head of pancreas is absolutely unchanged. SUVmax of target is 6.9, SUVmax of liver is 5.8, and T/L ratio is 1.1.
CONCLUSION
Physiologic faint or intense uptake of 68Ga-DOTANOC in the head of the pancreas is relatively frequent: this finding occurred in, respectively, 23% and 8% of the 100 patients of our population and 26% and 6% of the 245 scans. The main finding of our retrospective study was that increased uptake of the tracer was stable over time regardless of the intensity or shape of the uptake. According to our data, any 68Ga-DOTANOC PET/CT study showing increased uptake in the head of the pancreas should be interpreted with caution and with reference to the specific clinical signs and symptoms.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication January 21, 2011.
- Accepted for publication February 23, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}