


Abstract
Despite advances in reperfusion therapy, acute coronary syndromes can still result in myocardial injury and subsequent myocardial infarction (MI). Molecular, cellular, and interstitial events antecedent to the acute MI culminate in deleterious changes in the size, shape, and function of the left ventricle (LV), collectively termed LV remodeling. Three distinct anatomic and physiologic LV regions can be described after MI: the infarct, border zone, and remote regions. Given the complexity of post-MI remodeling, imaging modalities must be equally diverse to elucidate this process. The focus of this review will first be on cardiovascular MRI of the anatomic and pathophysiologic LV regions of greatest interest with regard to the natural history of the post-MI remodeling process. This review will then examine imaging modalities that provide translational and molecular insight into burgeoning treatment fields for the attenuation of post-MI remodeling, such as cardiac restraint devices and stem cell therapy.
- basic cardiology
- technical cardiology
- clinical cardiology
- MRI
- cardiac MRI
- infarct expansion
- myocardial remodeling
Acute coronary syndrome, which can be defined as a constellation of clinical symptoms associated with acute myocardial ischemia, strikes nearly a million people in the United States each year (1) and is responsible for tens of billions of dollars in hospital charges (2). Optimal treatment with timely reperfusion therapy and pharmacologic intervention has made acute coronary syndrome increasingly survivable, even in the face of a rising incidence given the growing elderly population (1). Despite advances in reperfusion therapy, acute coronary syndromes can still result in myocardial injury and subsequent myocardial infarction (MI), evoking cellular and extracellular processes in the reperfusion phase leading to cell death, inflammation, and scar formation. Molecular, cellular, and interstitial events antecedent to the acute MI culminate in changes in the size, shape, and function of the left ventricle (LV), collectively termed LV remodeling. Despite successful reperfusion, lifestyle modification, and pharmacotherapy, the LV remodeling process continues unabated, resulting in an accrual rate of almost 1 million new patients per year at risk for developing heart failure (1). Accordingly, strategies to selectively and specifically monitor the molecular pathways that underlie the LV remodeling process hold great import to alleviate the socioeconomic and healthcare resource burden of post-MI remodeling.
To identify appropriate imaging targets in the context of post-MI LV remodeling, the anatomic and biologic underpinnings of the process must be considered. For the purposes of the remodeling process, the post-MI LV can be divided into 3 distinct anatomic regions: the MI itself, the surrounding border zone, and the remaining remote myocardium. Regardless of reperfusion, degradation of normal extracellular matrix occurs within the MI region, accompanied by invasion of inflammatory cells and induction of bioactive peptides and cytokines, leading to the necessary substructure for scar formation (3,4). The fully perfused myocardium surrounding the MI, described as the border zone, is a metabolically active amalgam of inflammatory cells, fibroblasts, and viable myocytes. The border zone is also the site of infarct expansion, a dynamic process defined as the extension of changes in structure and function between the MI and remote myocardium. Infarct expansion is a process of great import, as it has been identified as an independent predictor of mortality for post-MI patients (5). The remote region is normally perfused and can be millimeters to centimeters away from the MI region and border zone. Despite conventional belief, the remote region is not immune to the post-MI remodeling process, as changing wall strain patterns after MI lead to myocyte hypertrophy and interstitial fibrosis (6). Each of these 3 anatomic regions is distinctly different, and therefore the heterogeneity of the regions and cellular targets within the post-MI LV must be recognized in order to achieve appropriate imaging modalities.
Although post-MI remodeling is a continually evolving process, the 30th day after MI can be described as a milestone time point at which the infarct itself is roughly healed. Several large-animal studies have been conducted examining this period of the remodeling process and the unique events happening in each of the 3 anatomic regions (7–18). Jugdutt et al. used a canine model to characterize the collagen dynamics, as well as the effects of angiotensin-converting enzyme inhibition on collagen deposition, within the infarct zone during this time frame (7,8). Subsequently, MI collagen and the myofibroblasts that produce it have become molecular imaging targets, capable of reflecting the therapeutic effects of angiotensin-converting enzyme inhibition (9). In the border zone, vascular endothelial growth factor, a marker of angiogenesis during the post-MI remodeling process, has been studied in pigs, providing a molecular imaging target to assess border zone myocardial perfusion status (10–12). Integrins specific to angiogenic vessels have also been used as a novel target for imaging angiogenesis in post-MI large-animal models (13). Noninvasive imaging of angiogenesis in the border zone holds important implications for risk stratification of patients after MI and the potential to evaluate the response to therapeutic measures aimed at myocardial angiogenesis. Unique portfolios of matrix metalloproteinases, a family of proteases that have been shown to be integral to the extracellular matrix remodeling process, have been characterized in all post-MI regions in sheep models (14,15) and provide noninvasive molecular imaging targets to interrogate the post-MI remodeling process. Apoptotic markers are clearly involved with pathways that can contribute to adverse remodeling after MI (16). At present, the imaging of apoptotic pathways has been limited to small-animal models (19) but clearly holds relevance for clinically relevant large-animal models. A summary of domains of the biologic remodeling process (i.e., extracellular matrix, vasculature, and signaling pathways) is presented in Table 1, as well as potential imaging targets. Imaging of the post-MI remodeling process holds great import for both prognostic information and potential monitoring of therapeutic interventions.
Molecular Imaging Targets in Post-MI Remodeling Process
Given the complexity of post-MI remodeling, imaging modalities must be equally diverse to elucidate this process. Consequently, it is not possible to integrate the entire body of imaging studies that are applicable to LV remodeling in this brief review. Rather, the focus of this review will first be on cardiovascular MRI of the anatomic and pathophysiologic LV regions of greatest interest with regard to the natural history of the post-MI remodeling process. Second, this review will examine imaging modalities that provide translational and molecular insight into burgeoning treatment fields for the attenuation of post-MI remodeling, such as cardiac restraint devices and stem cell therapy.
POST-MI LV REMODELING: BIOPHYSICAL CHARACTERIZATION BY MRI
By being able to provide accurate, reproducible images of high spatial and temporal resolution in any plane, cardiac MRI is especially suited for longitudinal assessment of post-MI LV remodeling (Fig. 1) (20,21). Several studies have used MRI techniques to gain molecular and cellular insight into the post-MI remodeling process. Specifically, Friedrich et al. have demonstrated the use of MRI to characterize reversibly and irreversibly injured myocardium in and around the MI region (Fig. 2) (22). They hypothesize that mapping areas of post-MI myocardial edema, using T2-weighted and late enhancement MRI, can guide therapeutic modalities to the border zone in attempts to attenuate infarct expansion. Other reports have targeted the reduction of post-MI edema, as detected by MRI, as a novel method to attenuate LV remodeling at the molecular level (23). After MI, contrast-enhanced MRI techniques provide visualization of microvascular obstruction in the infarct region (24). Regions of microvascular obstruction, which can persist despite reperfusion, appear as subendocardial dark areas surrounded by hyperenhanced injured myocardium and have been reported as a marker for adverse LV remodeling (25). In a landmark report by Wu et al., contrast-enhanced MRI showed that microvascular obstruction and infarct size correlated with long-term prognosis, including the development of heart failure (26).

Examples of delayed-enhancement MRI of 2 different MIs demonstrating relationship between LV remodeling and functional recovery. (A) Large anteroseptal transmural acute MI with areas of microvascular obstruction within infarct region (arrow) is shown in acute phase. Images 6 mo after MI show substantial LV remodeling, with wall thinning and absence of regional functional recovery. (B) Small inferolateral subendocardial MI with regional hypokinesis is shown in acute phase. Subsequent 6-mo post-MI images show lack of LV remodeling and complete recovery of regional contractility, in contrast to MI shown in A. (Reprinted with permission of (21).)

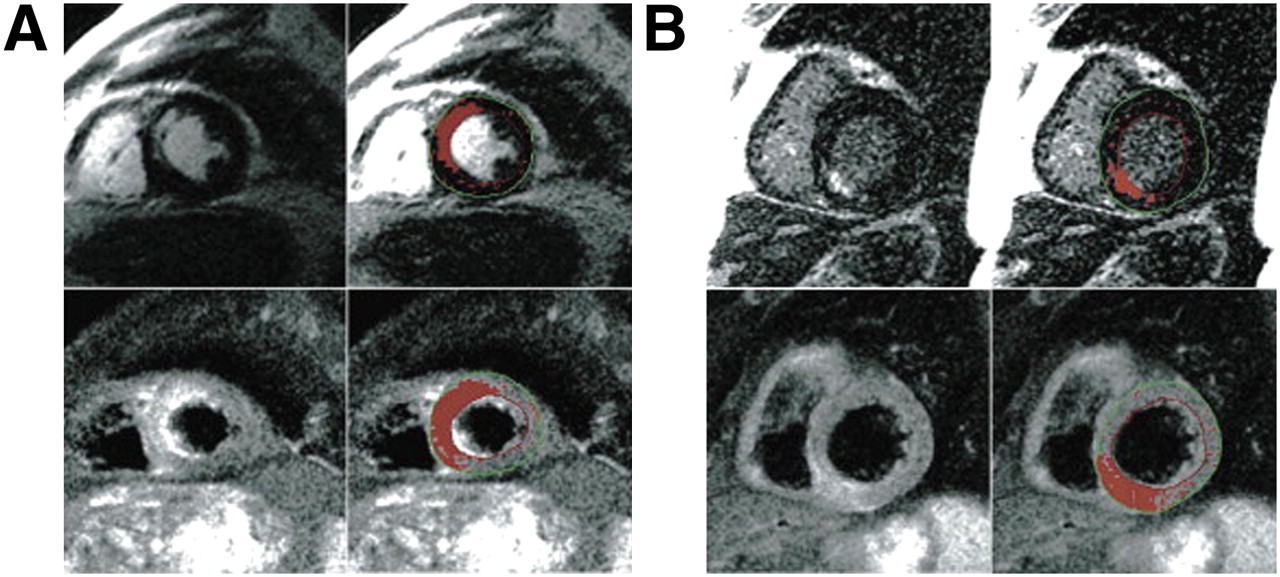
In 2 patients, irreversible and reversible injury in acute reperfused infarcts as visually and semiautomatically defined. (A) Cardiac MRI 3 d after acutely reperfused infarct with subtotal (99%) occlusion of left anterior descending artery in 71-y-old patient. (B) Cardiac MRI 1 d after reperfusion of occluded right coronary artery in 57-y-old patient. Red areas indicate result of semiautomatic delineation of pixels with abnormal signal as defined by signal intensity more than 2 SDs above mean signal intensity of remote myocardium. Spatial extent of myocardial injury in edema-sensitive T2 imaging is consistently larger than that of necrosis-sensitive late enhancement. (Reprinted with permission of (22).)
The topography of the LV after MI is a heterogeneous landscape, with great prognostic value held in the infarct characteristics and myocardial perfusion status (27,28). This landscape is made traversable to researchers and clinicians with the help of a variety of imaging modalities. Although CT can provide high-resolution static images to identify the region of MI, the current consensus is that MRI is able to provide better cardiac images than CT (29,30) with an additional feature of superior tissue characterization. For example, both clinical and preclinical studies (31,32) have used diffusion tensor MRI to study myocardial fiber architecture characteristics, describing distinct unique qualities among the MI region, border zone, and remote region. Specifically, the percentage of left-handed helical fibers was shown to have increased from the remote zone (13.3% ± 5.8%) to the border zone (19.2% ± 9.7%) and infarct zone (25.8% ± 18.4%) in patients at a median of 26 d after MI (32). Myocardial fiber architecture correlated with infarct size and LV function in these studies, linking structural and functional post-MI remodeling (32). Furthermore, by identifying these distinct anatomic LV regions, this imaging technology can enable scientists and clinicians to intervene in the post-MI remodeling process.
Another technique that has been used to characterize the distinct myocardial regions involved in post-MI remodeling is magnetic resonance spectroscopy (MRS). A multitude of myocardial metabolites can be noninvasively detected using MRS, characterizing the regional metabolic changes that occur in post-MI remodeling. Hu et al. reported a 50% reduction in the phosphocreatine–to–adenosine triphosphate ratio in the border zone, as compared with the remote region of a porcine MI model, indicating that border-zone energy defects likely contribute to local dysfunction after MI (33). Feygin et al. used MRS to examine border-zone bioenergetics after mesenchymal stem cell injection, reporting significant improvement in the phosphocreatine–to–adenosine triphosphate ratio 4 wk after MI in a porcine model (34). Hence, MRS allows interrogation of specific myocardial regions after MI and provides an assessment of therapeutic response. Presently, however, the spatial and temporal resolution limitations of MRS have not yet allowed high-resolution cardiac metabolic imaging to become a clinical reality.
REGIONAL IMAGING AFTER MI: PROGNOSTIC AND THERAPEUTIC POTENTIAL
Molecular imaging of the unique regions involved in post-MI LV remodeling holds great prognostic importance. Noninvasive, longitudinal assessment of qualities such as the fiber architecture and metabolism of the border zone hold the potential to risk-stratify patients. By identifying those at risk for continued post-MI adverse remodeling, we can direct these patients to adjuvant therapies in an effort to reduce the morbidity of the LV remodeling process. Hence molecular imaging techniques hold promise for further individualizing the treatments patients receive after MI.
Given the prevalence and dire consequences of the LV remodeling process, a multitude of devices and therapies have been developed in an effort to battle this clinical entity. The high-quality images produced by cardiac MRI have become an excellent tool for guiding the use of such technologies. One specific group of devices aimed at attenuating LV remodeling after MI are ventricular restraint devices, which apply epicardial pressure to combat dilation of the LV and reduce LV wall stress (35,36). Magovern et al. used cardiac MRI to evaluate the placement of a nitinol mesh device (Paracor Surgical Inc.) in an ovine MI model. MRI at 6 wk after MI demonstrated less increase in LV end-diastolic volume index and end-systolic volumes in device-treated animals than in controls, as shown in Figure 3 (35). This study set the stage for future work that would use MRI techniques to characterize the regional effects of a cardiac restraint device on post-MI remodeling. Specifically, Blom et al. used cardiac MRI and novel 3-dimensional surface modeling techniques to measure the degree of infarct expansion and global LV remodeling in an ovine MI model with the CorCap (Acorn Cardiovascular) ventricular restraint device (36). The study found that animals treated with the device at 3 d after MI had a decreased infarct area and improved contractile function in the border zone, compared with control animals at 12 wk after MI (36). Device-treated animals demonstrated no expansion in either the infarcted or perfused regions after device placement, compared with control animals, which displayed more than 300% expansion in the surface area of the infarct region. These results supported the conclusion that early ventricular restraint after MI is effective in limiting infarct expansion and LV remodeling. Cardiac MRI techniques have transitioned the examination of these specific devices from preclinical studies to clinical application, providing valuable noninvasive follow-up capabilities (Fig. 4).

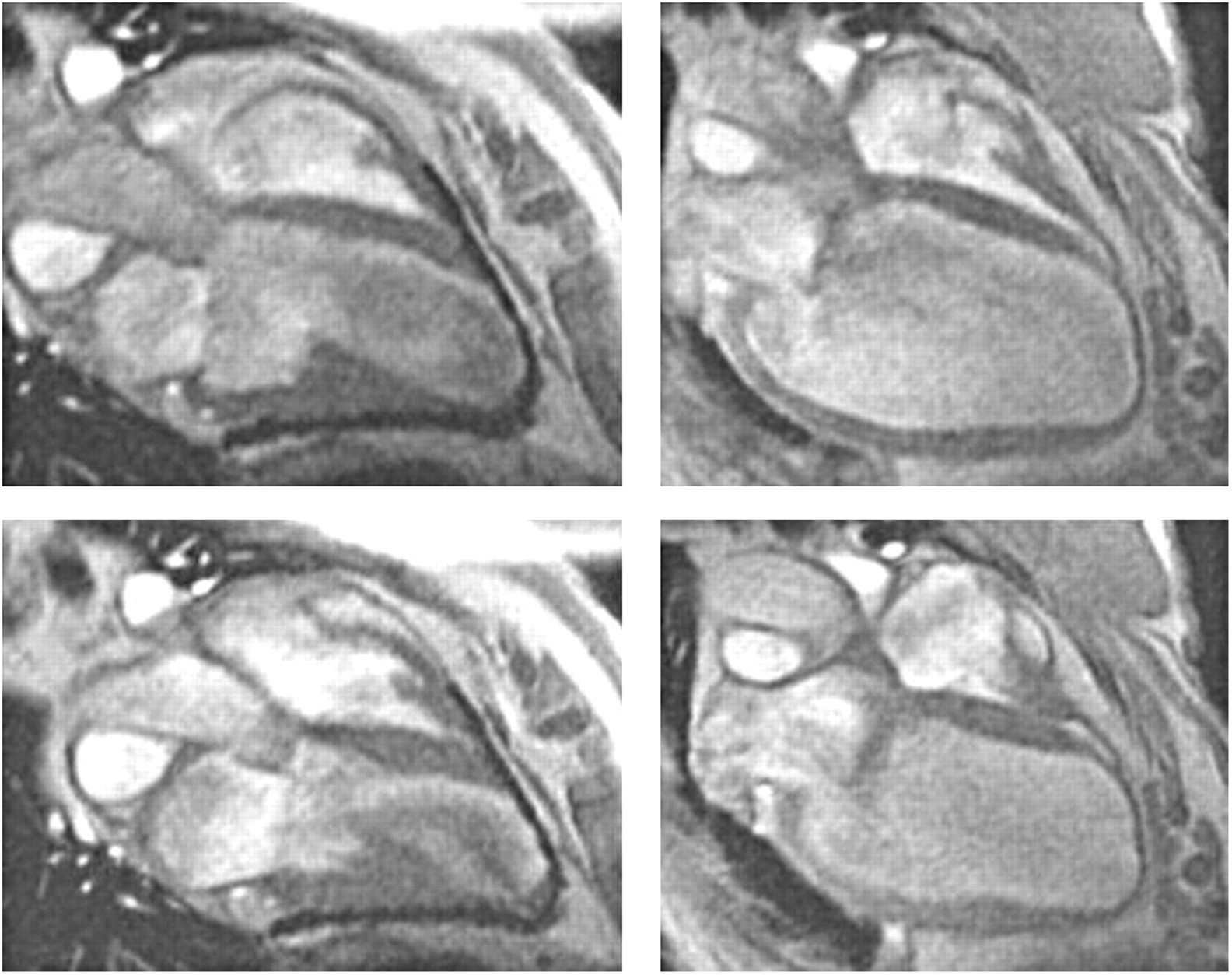
Long-axis MR images obtained 6 wk after infarction of device (left) and control (right) sheep hearts. Hearts are shown in diastole in top panels and systole on bottom. Mesh appears as dark area around ventricles. (Reprinted with permission of (35).)

Epicardial elastic support device in dilated cardiomyopathy. Left panel shows preoperative cardiac MR images from patient with dilated cardiomyopathy. Right panel shows same patient 6 mo after placement of HeartNet (Paracor Medical, Inc.). (Courtesy of Robert W.W. Biederman, Allegheny General Hospital, Pittsburgh, PA).
Another field that has drawn great attention in the treatment of LV remodeling is the use of cellular therapies. Specifically, the use of various types of stem cells in the post-MI context has been extensively studied (37–39). MRI techniques using magnetically labeled stem cells have demonstrated the ability to track these cells after delivery to the myocardium. In a preclinical study, Kim et al. used MRI techniques to track magnetically labeled mesenchymal stem cells for up to 3 mo after injection into a prior MI site and to assess the functional response to the cell injection (37). The study found that the cells were able to be seen on MRI up to 10 wk after injection (Fig. 5) and that LV ejection fraction was improved, compared with control animals. Using similar MRI techniques, Hill et al. demonstrated the ability to track iron fluorophore particle–labeled mesenchymal stem cells in a porcine model up to 3 wk after MI (Fig. 6). The study also demonstrated that the iron-labeled mesenchymal stem cells retained in vitro viability, proliferation, and differentiation capability as well as in vivo viability after allogeneic transplantation (38). The minimum detectable amount of cells on serial MRI was found to be 105 cells per injection. These findings make MRI detection of iron-labeled cells an attractive alternative for the noninvasive evaluation of cellular therapies. This technique holds the potential to answer questions about cell engraftment, migration, and honing, to elucidate disparate results from early clinical trials involving cellular therapies in the post-MI context (38,39).

In vivo serial MRI. Serial short-axis views obtained at 1 (A), 2 (B), 4 (C), and 10 (D) wk show persistent signal void after injection of mesenchymal stem cells labeled with ferumoxides (Feridex; Bayer HealthCare Pharmaceuticals). (Reprinted with permission of (37).)

Serial in vivo and ex vivo MRI. Serial short-axis views of diastolic frames show persistent signal void after injection of 105 mesenchymal stem cells labeled with iron fluorophore particles. Imaging was performed on days 1 (A), 4 (B), and 21 (C). (D) Corresponding view of explanted heart on high-resolution 3-dimensional MRI showing signal void. (Reprinted with permission of (38).)
CONCLUSION
The post-MI remodeling process involves a heterogeneous anatomic and physiologic regional LV landscape. Although this complex landscape is rife for therapeutic intervention, its intricacies must first be elucidated. Each unique anatomic region holds potential targets to attenuate the progression toward heart failure. With the assistance of advancing cardiac MRI techniques, these potential targets will progress toward becoming valuable clinical therapies, and current treatment modalities will continue to be refined.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 1, 2009.
- Accepted for publication January 15, 2010.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.