


Abstract
We encountered local reactions at injection sites in 7 patients after an intravenous injection of 99mTc-hydroxymethylene diphosphonate (99mTc-HDP). Archived bone scans showed radiopharmaceutical extravasation at injection sites in all patients. To identify the mechanism underlying these local reactions, we challenged BALB/c mice with an 99mTc-HDP injection and investigated the mechanism involved. Methods: Seven solutions were prepared: 0.1 M acetic acid, 0.1 M NaOH, 2.1 mM 99mTc-HDP, 4.7 mM 99mTc-methylene diphosphonate (99mTc-MDP), 1.05 mM 99mTc-HDP diluted with normal saline, 37 MBq of 99mTc-pertechnetate, and normal saline. Six female BALB/c mice were subcutaneously injected in their backs with 0.04 mL of each solution. Backs were observed, and skin and subcutaneous tissues were acquired on days 5, 7, and 19 after injection. Two pathologists interpreted the histologic specimens. Results: The pH values of the 0.1 M acetic acid, 0.1 M NaOH, 2.1 mM 99mTc-HDP, 4.7 mM 99mTc-MDP, 1.05 mM 99mTc-HDP diluted with normal saline, 37 MBq 99mTc-pertechnetate, and normal saline were 3.28, 14.3, 4.79, 6.45, 6.16, 6.85, and 6.53, respectively. A slight redness was observed at 99mTc-HDP injection sites on day 5 after injection, and many inflammatory cells, such as neutrophils, were found to infiltrate subcutaneous tissues by light microscopy, suggesting active inflammation. However, no abnormality was found at 99mTc-MDP injection sites. On day 19, 99mTc-HDP injection sites appeared to have recovered and showed healed scars and almost-normal microscopic features. Conclusion: Our results indicate that the local reaction induced by extravasation of 99mTc-HDP is probably caused by high acidity, and 99mTc-HDP should be administered carefully to avoid adverse reactions.
- 99mTc-hydroxymethylene diphosphonate (99mTc-HDP)
- 99mTc-methylene diphosphonate (99mTc-MDP)
- extravasation
Diphosphonate is a widely used radiopharmaceutical for bone scanning, and no significant toxic effects have been reported to date (1). Regarding adverse reactions, only 0.5 were reported for every 100,000 administrations in 1984 (2).
We started to use 99mTc-hydroxymethylene diphosphonate (99mTc-HDP) as a bone scanning agent instead of 99mTc-methylene diphosphonate (99mTc-MDP) at the Seoul National University Hospital in January 2008 because 99mTc-HDP has better physiochemical and biologic characteristics than 99mTc-MDP (3). After this change, 7 of 2,700 patients (0.26%) complained of a sharp pain at the injection site immediately after 99mTc-HDP administration and continued to experience pain and inflammation at injection sites 2 wk later. Retained bone scans showed radiopharmaceutical extravasation in all patients. The reported adverse reactions to diphosphonate included typical drug reactions such as rash, headache, dizziness, nausea, myalgia, and fever (4). However, we have not encountered adverse reactions of pain or inflammation over more than 30 y of 99mTc-MDP use, and we infer that these 99mTc-HDP reactions are not systemic but local because patient responses were immediate and the pain was localized.
No previous study has been conducted on the local adverse reactions induced by 99mTc-HDP. Accordingly, we compared histologic changes induced by 99mTc-HDP and 99mTc-MDP after administering them subcutaneously to BALB/c mice and investigated the mechanism underlying the pain and redness at 99mTc-HDP injection sites in an effort to avoid these reactions.
MATERIALS AND METHODS
Animals
Six adult female BALB/c mice (18–20 g) were used in this study. The animals were 6–8 wk old at the start of the experiment.
Radiopharmaceuticals and Control Materials
99mTc-HDP and 99mTc-MDP were synthesized in the usual manner, as described in the manufacturer's directions for use, and the concentration of 99mTc-HDP and 99mTc-MDP were 2.1 and 4.7 mM, respectively. 99mTc-HDP vials (Mallinckrodt Medical BV) contained oxidronate sodium (3.0 mg), stannous chloride (0.24 mg), gentisic acid (0.84 mg; a stabilizer), and sodium chloride (30.0 mg). 99mTc-MDP vials (GE Healthcare) contained sodium medronate (6.25 mg), stannous fluoride (0.34 mg), and sodium p-aminobenzoate (2 mg) as a freeze-dried mixture.
As a positive control, we used 0.1 M acetic acid as an acid solution and 0.1 M sodium hydroxide as an alkali solution. Normal saline was used as a negative control. For comparison purposes, 37 MBq of 99mTc-pertechnetate and 1.05 mM 99mTc-HDP diluted with normal saline were prepared.
Measurement of pH
The pH values of each solution (2-mL aliquots) were measured in triplicate and averaged. To evaluate pH changes caused by radiopharmaceutical decay, we checked the pH values of each solution after 2 d of cold storage.
Injection and Assay
The 7 solutions (0.04 mL) were injected subcutaneously, more than 1 cm apart, into the backs of each mouse. Injection sites were observed daily. Two mice were sacrificed on days 5, 7, and 19 after injection.
Subcutaneous tissues for histologic examinations were fixed in 10% buffered formalin for 24 h. Paraffin-embedded tissue sections were stained with hematoxylin and eosin.
RESULTS
Measurement of pH
The pH values of the 7 solutions—0.1 M acetic acid, 0.1 M NaOH, 2.1 mM 99mTc-HDP, 4.7 mM 99mTc-MDP, 1.05 mM 99mTc-HDP diluted with normal saline, 37 MBq of 99mTc-pertechnetate, and normal saline—were 3.28, 14.3, 4.79, 6.45, 6.16, 6.85, and 6.53, respectively. Because the pH of 99mTc-HDP (4.79) was substantially lower than that of 99mTc-MDP (6.45), its higher acidity could have caused the pain during injection. The pH values of radiopharmaceutical solutions were not found to change significantly during storage.
Time Course of Inflammation
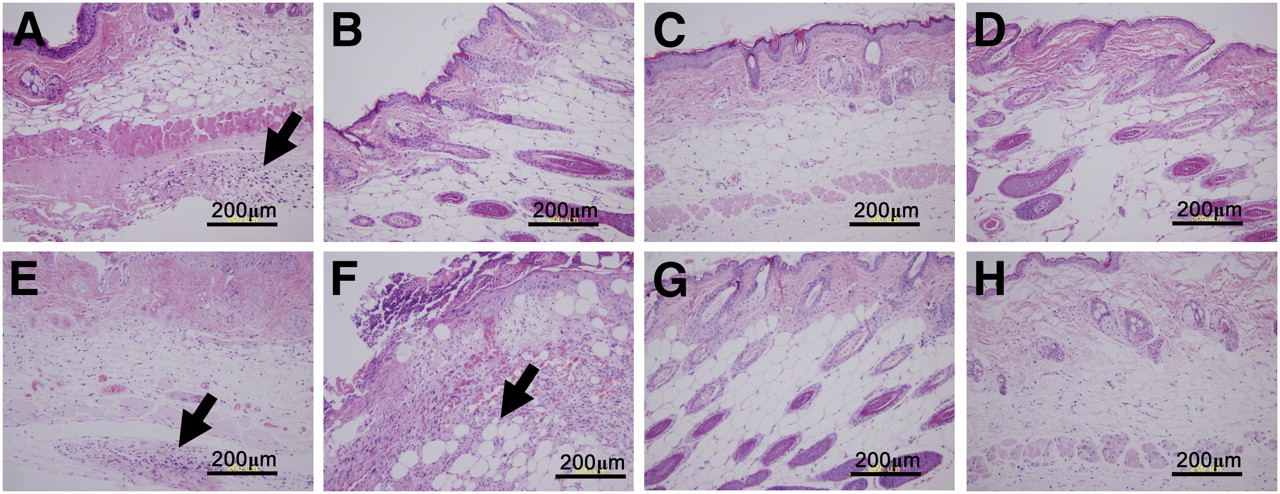
Red ulceration developed at 99mTc-HDP injection sites in BALB/c mice macroscopically, but no abnormality was found at 99mTc-MDP injection sites at 5 d after injection. Mononuclear and polymorphonuclear leukocytes were present in subcutaneous tissues with fibrinoid necrosis at 99mTc-HDP injection sites at 5 d after injection, suggesting active inflammation, and this inflammation completely resolved on day 19 (Fig. 1). However, no severe inflammation was seen at 99mTc-MDP injection sites at 5 or 19 d after injection.

Comparison of histologies at 99mTc-HDP and 99mTc-MDP injection sites. 99mTc-HDP injection site at 5 d after injection (A) shows multiple neutrophils in subcutaneous area (black arrow), suggesting active inflammation and fibrinoid necrosis. 99mTc-HDP injection site at 19 d after injection (B) revealed only focal inflammatory cells. No severe inflammation was seen at 99mTc-MDP injection sites at 5 (C) or 19 d after injection (D). Acetic acid injection site at 5 d after injection (E) has multiple neutrophils in subcutaneous area (black arrow), suggesting active inflammation. NaOH injection site at 5 d after injection (F) shows multiple neutrophils and liquefaction necrosis in subcutaneous area (black arrow). However, no evidence of inflammation was found at injection site for 99mTc-HDP diluted with normal saline (G) or injection site for just normal saline (H) at this time. (Hematoxylin and eosin, ×200).
Large ulceration developed at acetic acid and NaOH injection sites macroscopically at 5 d after injection. Neutrophils, eosinophils, and necrotic materials were observed at acetic acid injection sites at 5 d after injection, suggesting active inflammation. Necrotic epidermal ulceration, liquefaction, coagulation, subcutaneous fibrinoid necrosis, and multiple neutrophils were observed at NaOH injection sites at 5 d after injection. Fibrotic healings were observed at acetic acid and NaOH injection sites at 19 d after injection.
Only minimal inflammatory cells were found at injection sites for 99mTc-HDP diluted with normal saline and 99mTc-pertechnetate at 5 d after injection, an almost normal finding. No evidence of inflammation was found at normal saline injection sites at this time.
DISCUSSION
The present study demonstrates that 99mTc-HDP injections into subcutaneous tissues induce active inflammation. To explain the adverse reaction at 99mTc-HDP, but not at 99mTc-MDP, injection sites, we considered the greater acidity of 99mTc-HDP to be the potential cause.
The results of the present study concur with those of an earlier study, in which the incidence of infusion thrombophlebitis increased when a solution with a low pH and high tonicity was administered subcutaneously (5).
The ideal pH of a radiopharmaceutical is 7.4 (the pH of blood), although pH can vary between 2 and 9 because blood has a substantial buffering effect (6). However, stricter standards for subcutaneous administration are required because the buffering ability of subcutaneous tissues is less than that of blood. An allowable pH range of 5.5–8.0 for radiopharmaceuticals has been suggested by Chung and Lee (7), and caution is necessary when 99mTc-HDP is administered because the pH of 99mTc-HDP is less than 5.5 in the present study and 99mTc-HDP extravasation might cause irritation.
With respect to chemical skin injury, solutions with pH values of less than 2 can produce coagulation necrosis on contact with the skin, and similarly, alkalis with pH values greater than 11.5 can produce severe tissue injury due to liquefaction necrosis (8). Regarding the allowable pH range for subcutaneous infusions, both acidic agents (ondansetron at pH 3.5, morphine sulfate at pH 2.5–6.5) and alkaline agents (sodium phenobarbitone at pH 9.2–10.3) are being administered successfully subcutaneously without inducing skin irritation (9). However, in this previous study, successful administration without skin irritation was assessed physiologically and was not based on patients’ complaints.
We experienced 7 adverse reactions out of 2,700 99mTc-HDP administrations, and because these patients appeared to have serious complaints, we stopped using 99mTc-HDP as a bone scanning agent and resumed 99mTc-MDP use.
CONCLUSION
Patient complaints of a sharp pain after an 99mTc-HDP injection could be explained by the low pH of 99mTc-HDP. Available information provides direct in vivo evidence that extravasation of 99mTc-HDP may cause active inflammation. Accordingly, we recommend that 99mTc-HDP be administered carefully to avoid adverse reactions.
Acknowledgments
We thank Dr. Yun-Sang Lee, who kindly provided radiopharmaceutical information, and Dr. Hyo Sang Lee, Jin Uee Kim, and Sung Wook Cho, for their excellent technical and generous support. This work was supported by Priority Research Centers Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (2009-0093820).
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication May 4, 2010.
- Accepted for publication July 8, 2010.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.