


Article Figures & Data
Figures
- FIGURE 1.
Window settings for lumen and outer vessel boundary by CTA are the same as those for IVUS imaging. (A) Curved multiplanar reconstructed CTA image reveals significant stenosis in left anterior descending artery (arrow). (B) IVUS cross-section reveals lumen area of 2.1 mm2 and vessel area of 15.4 mm2. Cross-sectional CTA images show luminal CSA of 2.1 mm2 (C) and vessel CSA of 15.4 mm2 (D).
- FIGURE 2.
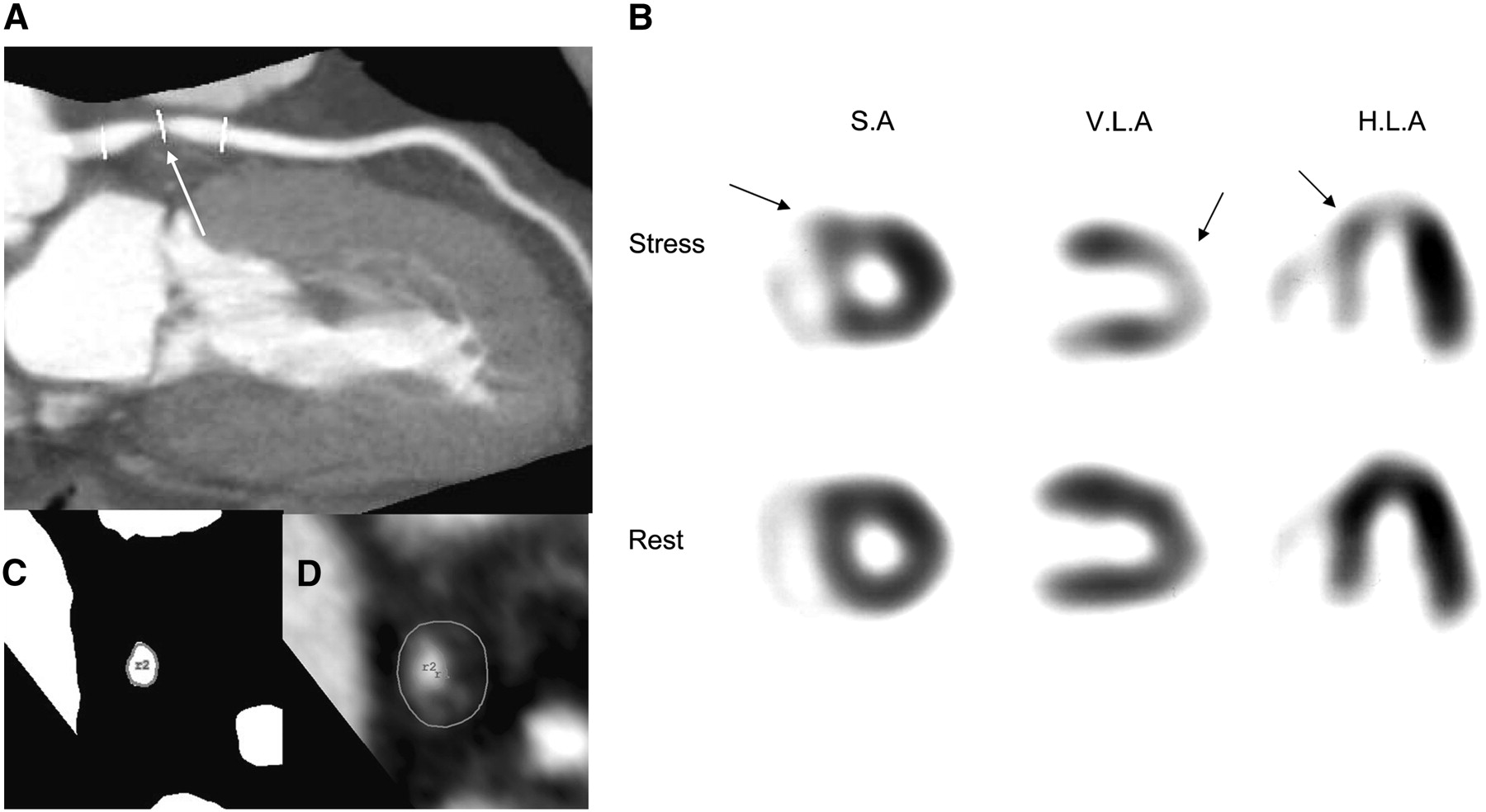
A 65-y-old woman with chest pain. (A) CTA image using maximum-intensity projection reveals presence of significant stenosis in proximal left anterior descending artery (arrow). (C) Minimal luminal CSA is 2.6 mm2. (D) Vessel CSA is 20.9 mm2. (B) Corresponding tomograms show reversible perfusion abnormality in anterior, septal, and apical wall (arrows). S.A = short axis; V.L.A = vertical long axis; H.L.A = horizontal long axis.
- FIGURE 3.
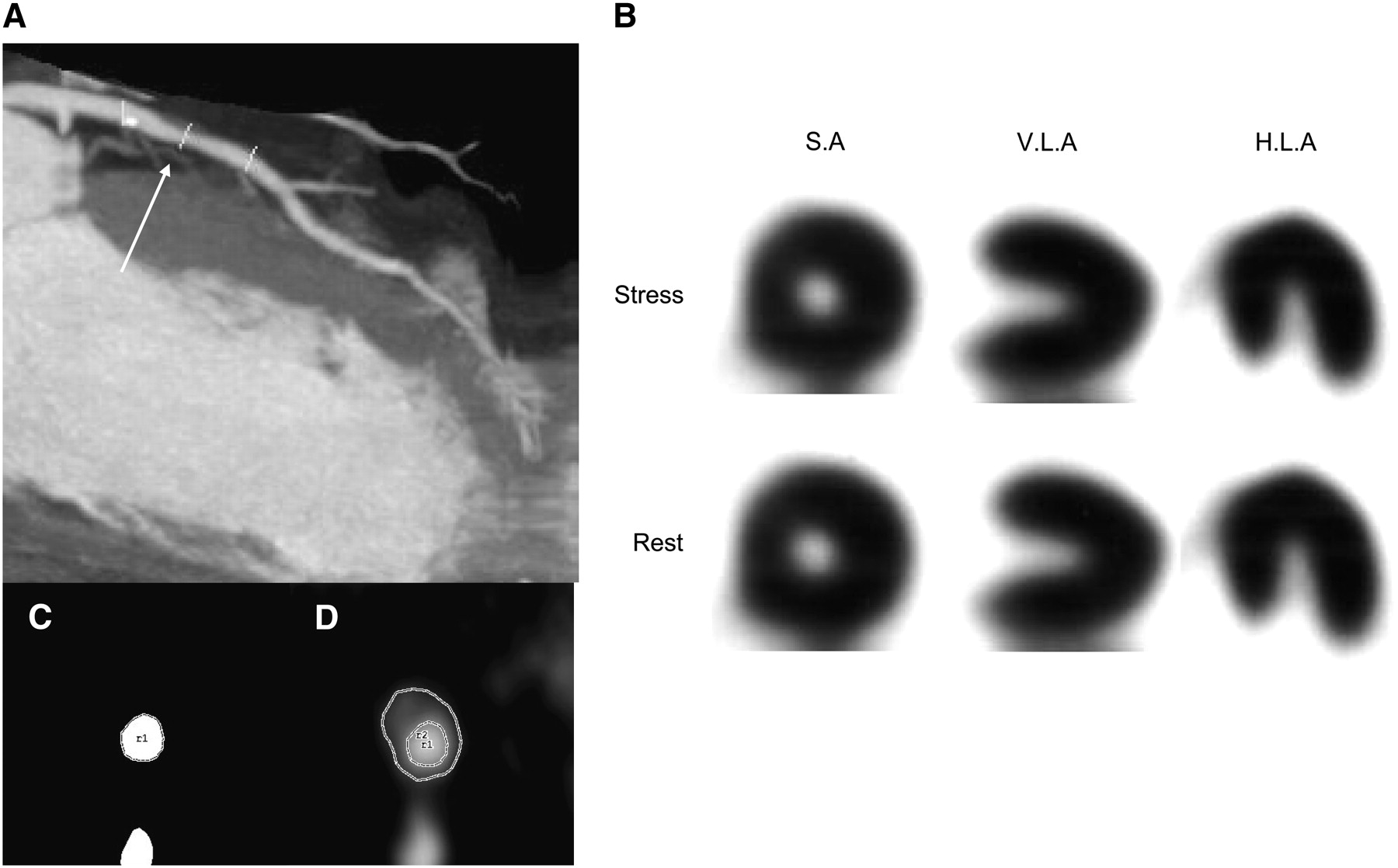
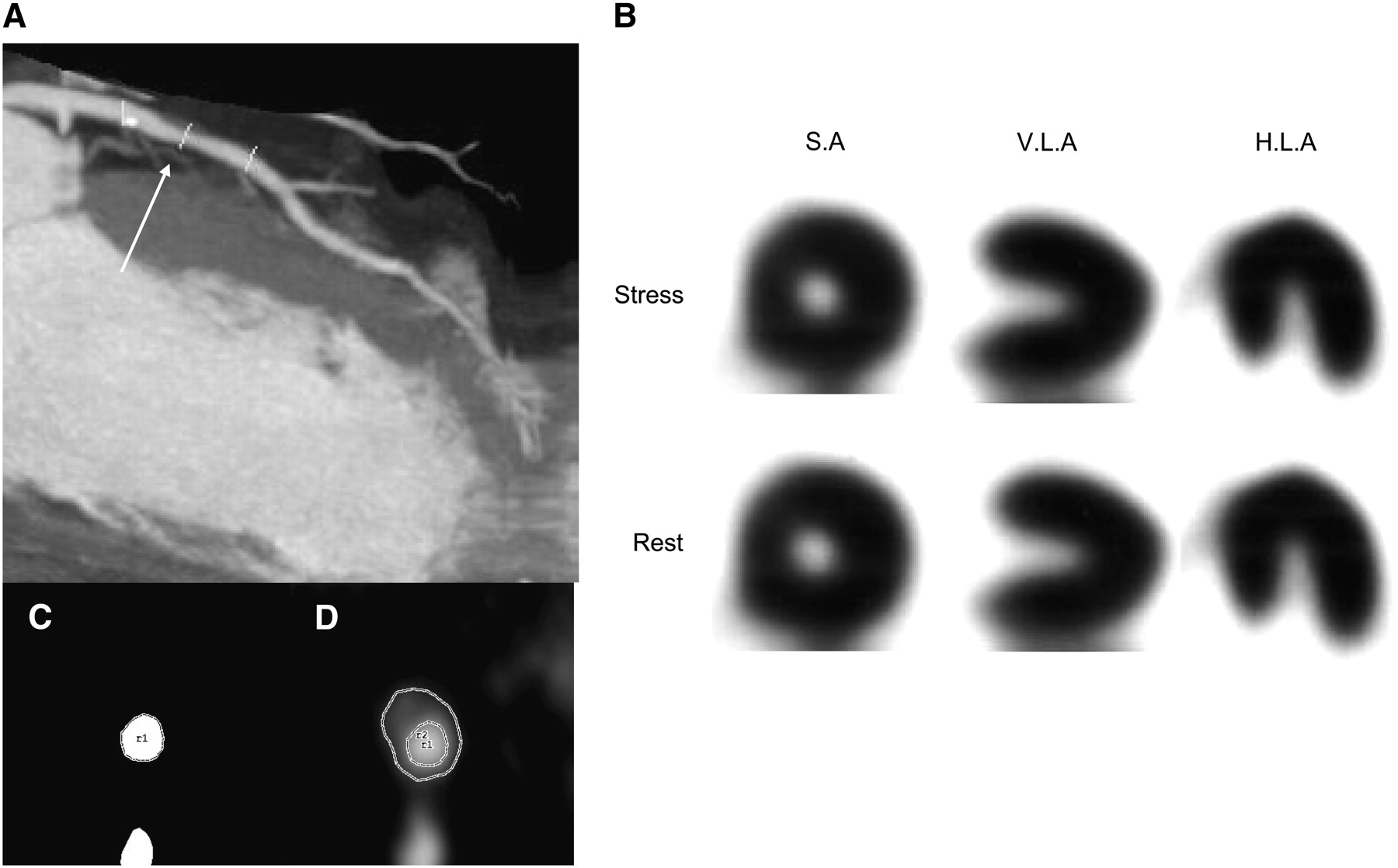
A 63-y-old man with chest pain. (A) CTA image using maximum-intensity projection shows noncalcified plaque in left anterior descending artery (arrow). (C) Minimal luminal CSA is 4.2 mm2. (D) Vessel CSA is 12.5 mm2. (B) Corresponding tomograms show normal perfusion at peak exercise and rest. S.A = short axis; V.L.A = vertical long axis; H.L.A = horizontal long axis.
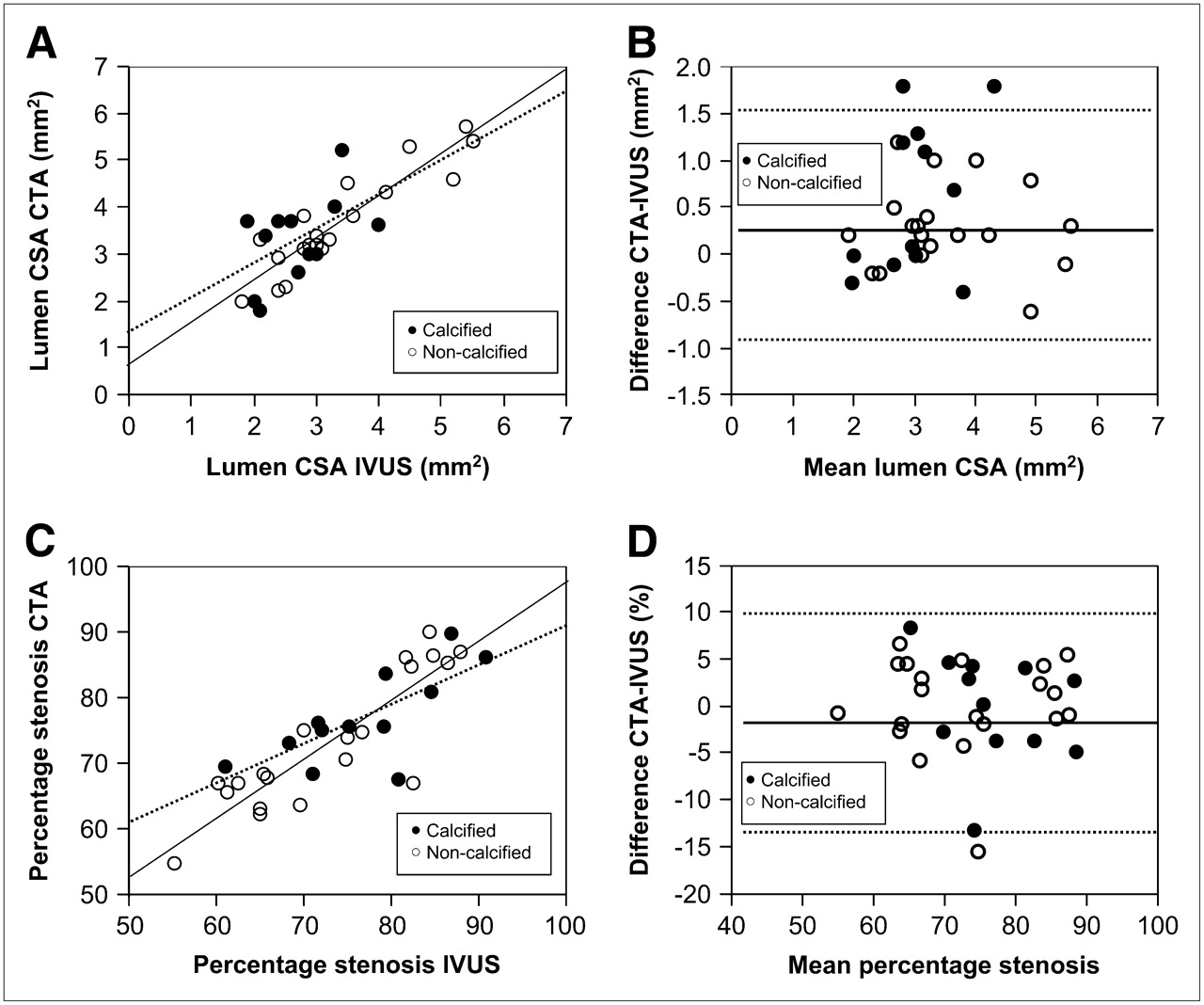
- FIGURE 4.
(A) Correlation between lumen CSAs measured by 64-slice CTA and IVUS (n = 32). Dashed lines correspond to correlation of calcified plaques (n = 12, y = 0.74x + 1.34, r = 0.55, P = 0.09), whereas solid lines correspond to correlation of noncalcified plaques (n = 20, y = 0.88x + 0.66, r = 0.91, P < 0.0001). (B) Bland–Altman analysis of differences between the lumen CSAs (mean difference, 0.27 ± 0.64 mm2). Dashed lines correspond to mean ± 2 SDs (−1.01 to 1.55 mm2). (C) Correlations between percentage stenosis measured by 64-slice CTA and IVUS (n = 32). Dashed lines correspond to correlation of calcified plaques (n = 12, y = 0.61x + 30.1, r = 0.73, P = 0.0069), whereas solid lines correspond to correlation of noncalcified plaques (n = 20, y = 0.88x + 8.43, r = 0.87, P < 0.0001). (D) Bland–Altman analysis of differences between percentage stenosis (mean difference, −0.22% ± 11%). Dashed lines correspond to mean ± 2 SDs (−11.2% to 10.7%). Open circles indicate noncalcified plaques, whereas solid circles indicate calcified plaques.
- FIGURE 5.
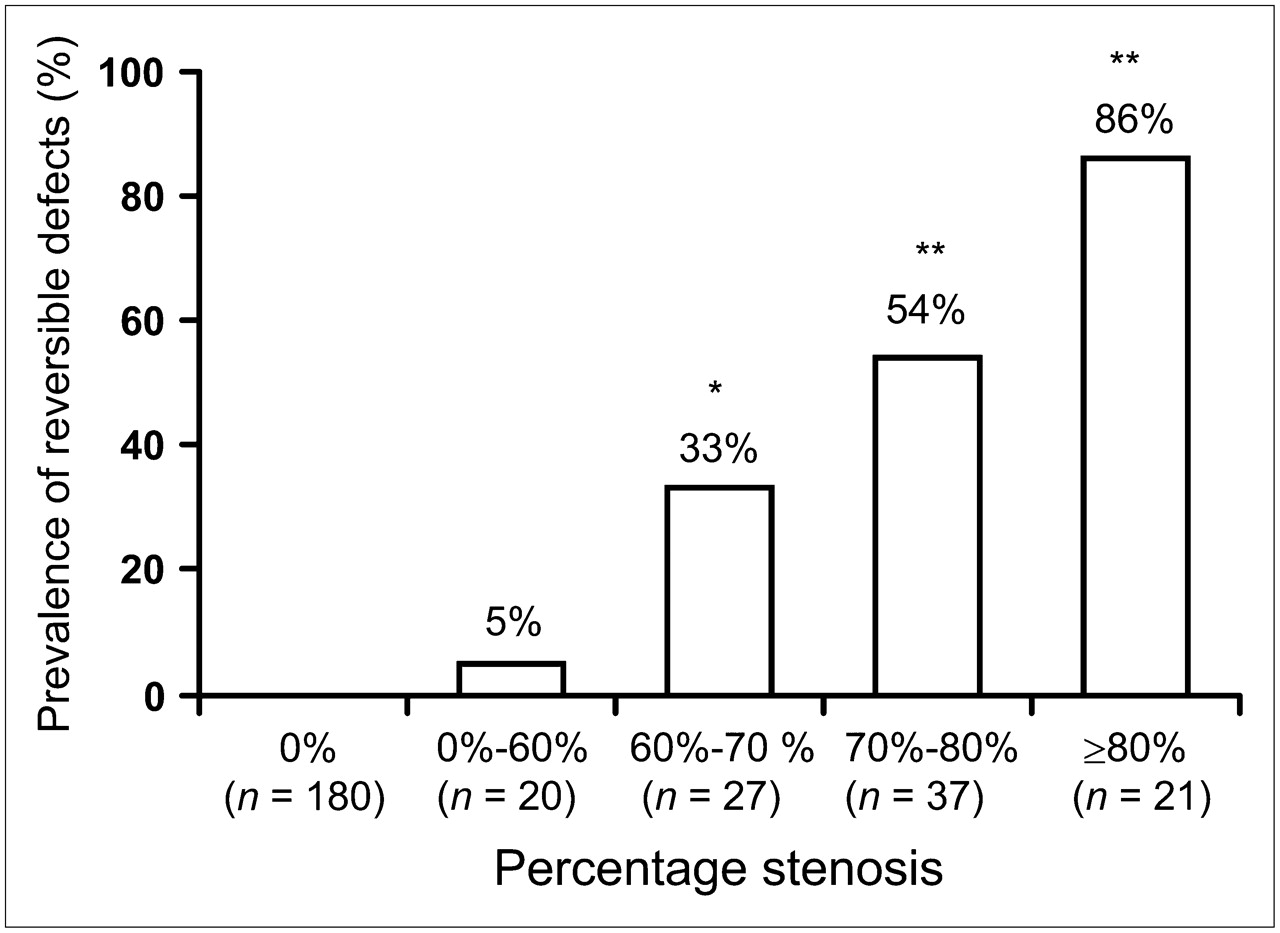
Prevalence of reversible defects evaluated by SPECT in study groups defined according to percentage stenosis obtained by CTA. Numbers under the bars represent number of vessels. *P = 0.018. **P < 0.0001 vs. percentage stenosis of 0%–60%.
- FIGURE 6.
(A) Quantitative perfusion defects in relation to percentage stenosis by CTA. (B) Quantitative perfusion defects in relation to minimal luminal CSA. Open circles indicate negative SPECT, and solid circles indicate positive SPECT.
- FIGURE 7.
Diagnostic value of CTA measurements for assessment of functionally significant coronary artery stenosis using stress 201Tl SPECT. ROC curves of lesion luminal CSA (A) and lesion percentage stenosis (B).




Tables
Characteristic Value Age (y) 66.9 ± 11 Male/female 76/28 Hypertension (%) 55 (53%) Hyperlipidemia (%) 57 (55%) Diabetes (%) 41 (39%) Smoking (%) 47 (45%) BMI (kg/m2), median (IQR) 23.8 (21.1–25.6) Symptoms Anginal chest pain 65 (62%) Atypical chest pain 22 (21%) Pretest likelihood of CAD Low 6 (6%) Intermediate 78 (75%) High 20 (19%) Resting ECG Negative T 7 (7%) ST depression 14 (13%) Left ventricular hypertrophy 25 (24%) BMI = body mass index; IQR = interquartile range.
- TABLE 3
Diagnostic Accuracy of Functionally Significant Coronary Artery Stenosis According to Stenosis Severity by 64-Slice CTA
Stenosis criterion (%) Sensitivity (%) Specificity (%) PPV (%) NPV (%) Vessels for analysis only with evaluable vessels >60 98 84 55 99 >70 79 92 66 96 >80 38 98 86 89 All vessels for analysis with positive nonevaluable vessels >60 98 77 46 99 >70 81 84 51 96 >80 43 90 48 89





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Coronary Microvascular Dysfunction: Clinical Considerations and Noninvasive Diagnosis
- SNMMI/ASNC/SCCT Guideline for Cardiac SPECT/CT and PET/CT 1.0
- Reply
- Impact of Coronary Plaque Composition on Cardiac Troponin Elevation After Percutaneous Coronary Intervention in Stable Angina Pectoris: A Computed Tomography Analysis
- 64-slice CT angiography for the detection of functionally significant coronary stenoses: comparison with stress myocardial perfusion imaging
- Quantitative Relationship Between the Extent and Morphology of Coronary Atherosclerotic Plaque and Downstream Myocardial Perfusion
- Quantification of Coronary Arterial Stenoses by Multidetector CT Angiography in Comparison With Conventional Angiography: Methods, Caveats, and Implications
- Comparison of the Extent and Severity of Myocardial Perfusion Defects Measured by CT Coronary Angiography and SPECT Myocardial Perfusion Imaging
- ACCF/ACR/AHA/NASCI/SAIP/SCAI/SCCT 2010 Expert Consensus Document on Coronary Computed Tomographic Angiography: A Report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents
- ACCF/ACR/AHA/NASCI/SAIP/SCAI/SCCT 2010 Expert Consensus Document on Coronary Computed Tomographic Angiography: A Report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents
- Cardiac PET Imaging for the Detection and Monitoring of Coronary Artery Disease and Microvascular Health
- Risk Assessment and Predictive Value of Coronary Artery Disease Testing
- Is Computed Tomography Coronary Angiography the Most Accurate and Effective Noninvasive Imaging Tool to Evaluate Patients With Acute Chest Pain in the Emergency Department?: CT Coronary Angiography Is the Most Accurate and Effective Noninvasive Imaging Tool for Evaluating Patients Presenting With Chest Pain to the Emergency Department: Antagonist Viewpoint
- The Year in Cardiac Imaging
- Noninvasive Diagnosis and Prognosis Assessment in Chronic Coronary Artery Disease: Stress Testing With and Without Imaging Perspective