


Abstract
SPECT with 99mTc-labeled agents is better able to detect viability after nitrate administration. Nitrates induce vasodilation and may increase blood flow to severely hypoperfused but viable myocardium, thereby enhancing tracer delivery and improving the detection of viability. Quantitative data on the changes in blood flow are lacking in SPECT but can be provided by PET. The aim of the present study was to use PET to evaluate whether nitrate administration increases blood flow to chronically dysfunctional but viable myocardium. Methods: 13N-Ammonia PET was used to quantitatively assess blood flow, and 18F-FDG PET was used as the gold standard to detect viable myocardium. Twenty-five patients with chronic ischemic left ventricular dysfunction underwent 13N-ammonia PET at rest and after nitrate administration. Results: A significant increase in nitrate-enhanced blood flow was observed in viable segments (from 0.55 ± 0.15 to 0.68 ± 0.24 mL/min/g, P < 0.05). No statistically significant change in blood flow was observed in nonviable segments (0.60 ± 0.20 vs. 0.55 ± 0.18 mL/min/g). A ratio of at least 1.1 for nitrate-enhanced flow to resting flow allowed optimal detection of viable myocardium, yielding a sensitivity of 82% with a specificity of 100%. Conclusion: 13N-Ammonia PET showed a significant increase in nitrate-enhanced blood flow in viable myocardium, whereas blood flow remained unchanged after nitrate administration in nonviable myocardium. Nitrate use during myocardial perfusion imaging will lead to improved assessment of myocardial viability.
Identification of viability in patients with chronic left ventricular (LV) dysfunction is important for therapeutic management; patients with viable myocardium may benefit from revascularization, whereas patients without viable myocardium should be treated conservatively (1). In daily practice, 99mTc-labeled tracers in combination with SPECT are frequently used for the assessment of viability (2). However, tracer delivery is flow dependent and may be suboptimal in severely hypoperfused regions, resulting in an underestimation of viability (3). To avoid this problem, tracer injection and subsequent imaging may be performed after nitrate administration (4). Nitrates induce vasodilation, are conjectured to improve blood flow to severely hypoperfused myocardium, and may enhance tracer delivery and improve detection of viability (5,6). However, data on absolute changes in myocardial blood flow after nitrate administration are limited. PET provides a noninvasive approach that permits quantitative measurements of regional myocardial perfusion and can thus be used to assess changes in blood flow after nitrate administration. Accordingly, the aim of the present study was to evaluate nitrate-induced changes in chronic dysfunctional but viable myocardium. For this purpose, PET with 13N-ammonia was used. For the assessment of viability, PET with 18F-FDG was used.
MATERIALS AND METHODS
Patients
Consecutive patients with chronic regional contractile dysfunction, as identified on gated 99mTc-tetrofosmin SPECT, were prospectively included. Patients with unstable angina, recent myocardial infarction (<3 mo), or heart failure requiring hospitalization were excluded. Twenty-five patients (all men; mean age ± SD, 61 ± 10 y) were enrolled. Their characteristics are summarized in Table 1. All patients had a depressed LV ejection fraction of less than 45%. Adverse reactions to nitrates were not observed. None of the patients experienced a cardiac event during the study period.
Baseline Characteristics of Study Population
Study Protocol
Gated 99mTc-tetrofosmin SPECT was used to identify regions with contractile dysfunction. To categorize the dysfunctional segments as viable or nonviable, 18F-FDG PET was used (segments with >50% 18F-FDG uptake were considered viable). Quantitative blood flow at rest and after nitrate administration was assessed with 13N-ammonia PET. All studies were performed within 2 wk. All patients continued taking their usual medication, with the exception of nitrates, which were discontinued 24 h before the PET studies. The study protocol was approved by the medical ethics committee of the institution, and all patients provided written informed consent.
SPECT
With the patient at rest, 600 MBq of 99mTc-tetrofosmin were injected. SPECT images, including gated images in 16 frames with an RR interval of ±10%, were acquired 1 h after tracer administration using a dual-head γ-camera (E.Cam; Siemens) equipped with low-energy high-resolution collimators. This system has a spatial resolution of 7.4 mm in full width at half maximum. The camera heads were perpendicular (90° opposed). Other acquisition parameters included 32 steps, 20 s per step, a 128 matrix, a zoom of 1.0, and rotation from 45° right anterior oblique to 135° left posterior oblique with the patient supine. Before filtered backprojection reconstruction, emission slices were 2-dimensionally filtered using a Butterworth filter with a cutoff frequency of 0.30 cycles per pixel of Nyquist frequency and order 6.
All data from the 99mTc-tetrofosmin SPECT studies were reoriented into short-axis and horizontal and vertical long-axis sections. A quantitative analysis program in a commercially available gated cardiac software package (4D-MSPECT; University of Michigan Medical Center) was used for assessing LV regional wall motion (7). LV wall motion was classified visually into 1 of 3 categories (0 = normal, 1 = hypokinesia, 2 = akinesia or dyskinesia) using the 9-segment model (4 basal and distal segments [anterior, lateral, septal, and inferior] and 1 apical segment).
PET
18F-FDG, Data Acquisition.
The patients consumed a glucose-enriched breakfast. Ninety minutes before 18F-FDG injection, 500 mg of acipimox (Nedios) was administered orally to lower the circulating free fatty acids (8). To prevent the side effects of acipimox (e.g., skin rash), we administered 250 mg of aspirin orally 5 min before acipimox intake. Guided by the plasma glucose levels, we gave insulin to 4 patients as previously described (9). The PET scanner was an ECAT EXACT HR+ (Siemens/CTI), which acquires 63 planes over a total axial length of 155 mm. 18F-FDG (200 MBq) was injected intravenously, and the PET dynamic acquisition followed. The total 18F-FDG PET acquisition time was 40 min, with the last 20 min acquired in gated mode with 16 frames per cardiac cycle. The length of each gate was based on the current RR interval. The RR interval was allowed to vary within ±10%. Data were corrected for attenuation using the transmission scan and were reconstructed using filtered backprojection (Hann filter, 0.5 pixels per cycle).
18F-FDG, Data Analysis.
A fully automatic, non–operator-dependent program (MATLAB; The MathWorks, Inc.) was used for reorientation of the raw data into 12 short-axis slices. A parametric polar map program was used to reconstruct 18F-FDG polar maps, divide them into 9 segments, and normalize them to 100%. Dysfunctional segments with at least 50% 18F-FDG uptake were classified as viable (10).
13N-Ammonia, Data Acquisition.
After the transmission scan (using 68Ge/68Ga rod sources), 400 MBq of 13N-ammonia were injected intravenously. A 12-lead electrocardiogram was monitored continuously throughout the study. Dynamic data were then acquired over 15 min. After completion of the baseline 13N-ammonia data acquisition, 5 mg of nitroglycerin were administered sublingually, and 10 min afterward a second injection of 400 MBq of 13N-ammonia was administered. Dynamic data were then acquired during another 15 min. Data were corrected for attenuation using the transmission scan and were reconstructed using filtered backprojection (Hann filter, 0.5 pixels per cycle). The data of the second 13N-ammonia scan were corrected for the remaining activity of the first scan by subtracting the remaining activity of the second 13N-ammonia scan.
13N-Ammonia, Data Analysis.
A fit procedure was performed according to the 3-compartment model described by Hutchins et al. (11), and absolute myocardial blood flow was calculated. MATLAB was used for reorientation of the data of the 13N-ammonia studies into 12 short-axis slices. A parametric polar map program was used to reconstruct polar maps for 13N-ammonia baseline flow and 13N-ammonia nitrate-enhanced flow (13N-ammonia-NTG); the polar maps were divided into 9 segments. Segmental values of 13N-ammonia myocardial blood flow were expressed in mL/min/g. In the viable and nonviable segments (according to 18F-FDG PET), segmental blood flow was quantified from the baseline 13N-ammonia data and from the 13N-ammonia-NTG data, providing the change in blood flow after nitrate administration in viable and nonviable segments.
In addition, the ratio of 13N-ammonia-NTG flow to 13N-ammonia baseline flow was calculated. Various parameters derived from 13N-ammonia flow were subsequently tested for the detection of viability, including baseline 13N-ammonia flow, nitrate-enhanced 13N-ammonia flow, and the ratio of 13N-ammonia-NTG to 13N-ammonia baseline. Receiver operating characteristic (ROC) curve analyses were used to define the optimal cutoff values for these parameters to detect viability (using viability on 18F-FDG PET as the gold standard).
Statistical Analysis
Values are presented as mean ± SD. Differences in mean values between 13N-ammonia baseline flow and 13N-ammonia-NTG flow were assessed by the Wilcoxon test for paired data with a nonparametric distribution. The Mann–Whitney test was used to compare differences in mean 13N-ammonia flow between viable and nonviable segments. ROC curve analyses were performed to define the optimal cutoff values for the various parameters to detect viability. The output of ROC curve analysis is an area-under-the curve (AUC) value ranging from 0 to 1. Using this AUC value, performance can be classified as excellent (0.90−1), good (0.80−0.90), fair (0.70−0.80), or poor (0.60−0.70). An AUC value of 0.50−0.60 indicates a test without value. Pairwise-deletion Mann–Whitney statistics were used to compare differences in AUCs (determined by ROC curve analysis) between 13N-ammonia baseline and 13N-ammonia-NTG. For all tests, a P value of less than 0.05 was considered significant.
RESULTS
Data analysis was based on 225 segments in 25 patients (9 segments per patient). Of these 225 segments, 88 (39%) had contractile dysfunction on gated 99mTc-tetrofosmin SPECT and were used for further analysis. Of these 88 segments, 64 (73%) showed hypokinesia and 24 (27%) showed akinesia or dyskinesia.
Effect of 13N-Ammonia-NTG on Resting Myocardial Blood Flow
Mean heart rate and blood pressure during 13N-ammonia baseline imaging were 62.9 ± 8.3 bpm and 92.6 ± 30.8 mm Hg. Mean heart rate and blood pressure during 13N-ammonia-NTG imaging were 61.8 ± 7.8 bpm and 90.8 ± 31.6 mm Hg (not a statistically significant difference from 13N-ammonia baseline).
When all dysfunctional segments were considered, there was a trend toward an overall increase in 13N-ammonia myocardial blood flow after nitrate administration (from 0.57 ± 0.16 mL/min/g at baseline to 0.64 ± 0.23 mL/min/g after nitrate administration, P = 0.06). The mean ratio of 13N-ammonia-NTG to 13N-ammonia baseline in dysfunctional segments was 1.15 ± 0.29. In segments with normal contraction, 13N-ammonia myocardial blood flow increased from 0.63 ± 0.20 to 0.71 ± 0.22 mL/min/g after nitrate administration (P < 0.01). The mean ratio of 13N-ammonia-NTG to 13N-ammonia baseline in segments with normal contraction was 1.16 ± 0.27.
Viable and Nonviable Segments
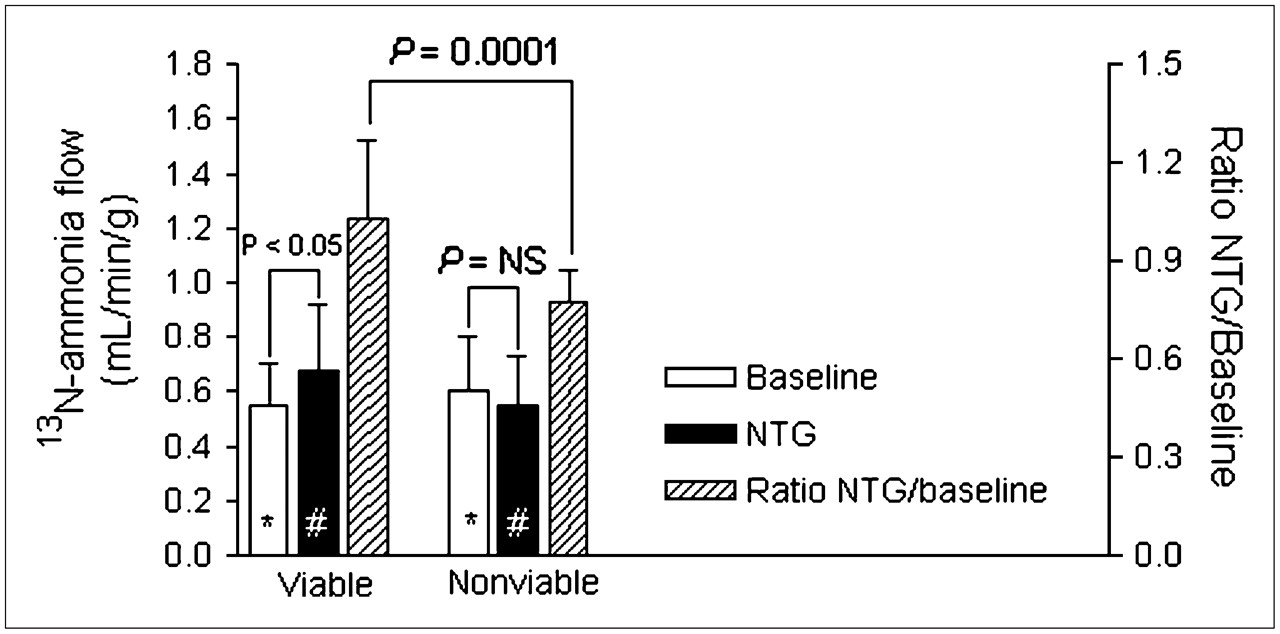
Of the 88 dysfunctional segments, 64 (73%) were viable on 18F-FDG PET. The mean 18F-FDG uptake was 82% ± 24% in viable segments, compared with 42% ± 13% in nonviable segments. The mean baseline 13N-ammonia flow did not significantly differ between viable and nonviable segments (Fig. 1). A significant increase in 13N-ammonia myocardial blood flow after nitrate administration was observed in the viable segments, whereas no increase in flow was observed in the nonviable segments. In particular, the mean increase was from 0.55 ± 0.15 to 0.68 ± 0.24 mL/min/g (P < 0.05). Consequently, the mean ratio of 13N-ammonia-NTG to 13N-ammonia baseline was significantly higher in viable segments than in nonviable segments. The change in blood flow observed in nonviable segments was 0.60 ± 0.20 to 0.55 ± 0.18 mL/min/g.
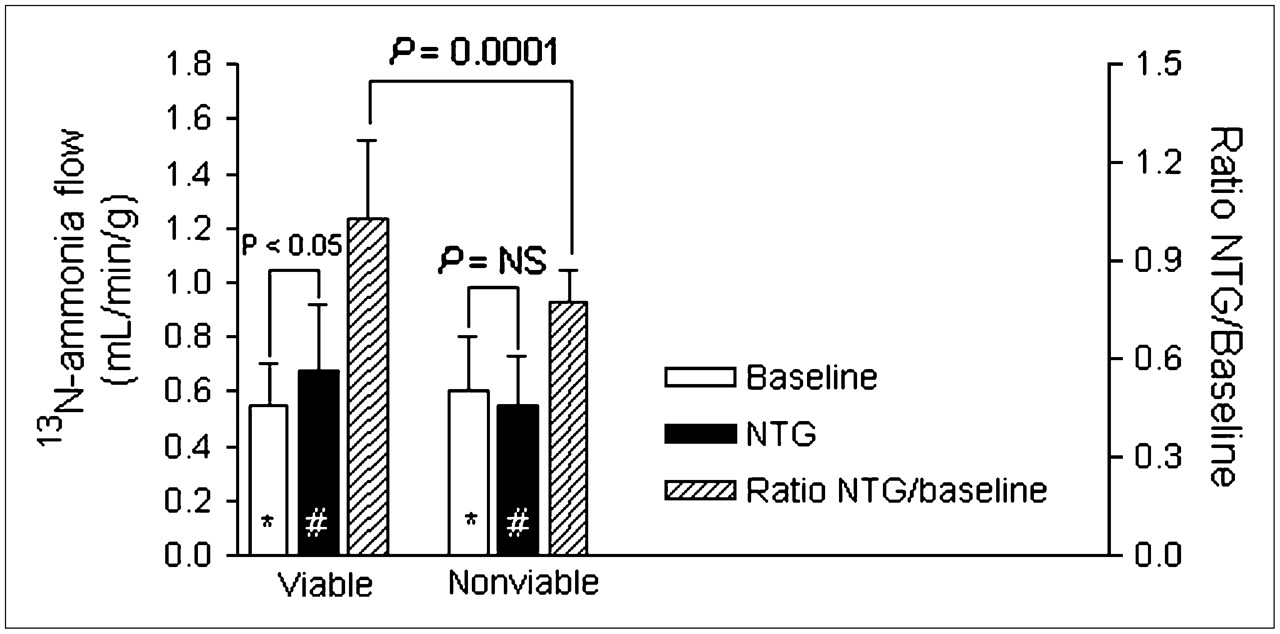
13N-Ammonia flow parameters in 18F-FDG viable and nonviable segments. Baseline = 13N-ammonia baseline flow; NTG = 13N-ammonia-NTG. *Not statistically significant, 13N-ammonia baseline flow in viable segments vs. in nonviable segments. #P = 0.009, 13N-ammonia nitrate-enhanced flow in viable segments vs. in nonviable segments.
Cutoff Level for Detection of Viability
When all dysfunctional segments were considered, ROC curve analysis of 13N-ammonia baseline resulted in an AUC of 0.45 ± 0.07; the optimal cutoff level was 0.50 mL/min/g, yielding a sensitivity of 50% and a specificity of 42%. ROC curve analysis of 13N-ammonia-NTG resulted in an AUC of 0.68 ± 0.065; the optimal cutoff level was 0.53 mL/min/g, providing a sensitivity of 70% and a specificity of 55% (P < 0.01 vs. 13N-ammonia baseline; Fig. 2).
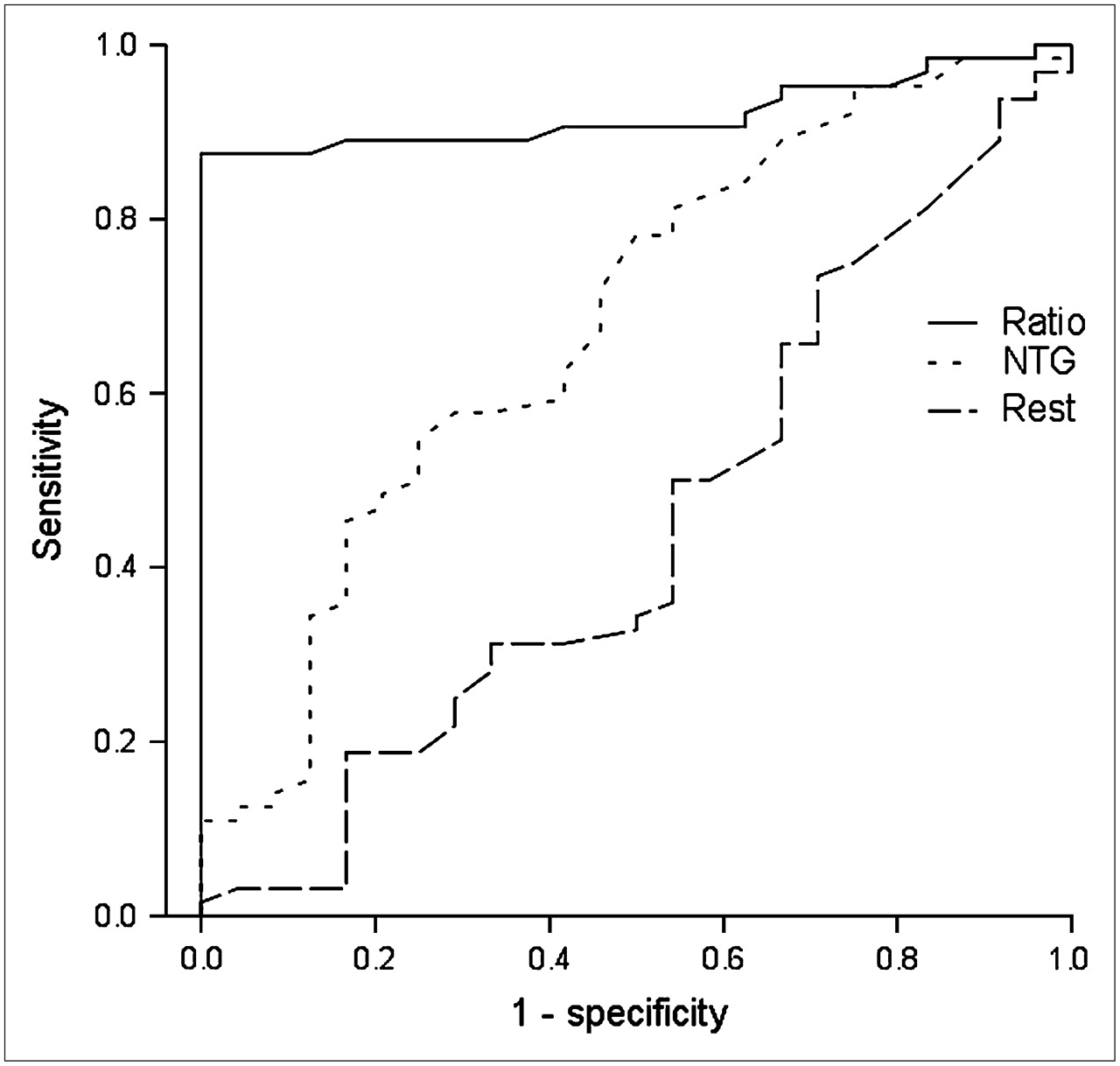
ROC curves of 13N-ammonia baseline, 13N-ammonia-NTG, and ratio of 13N-ammonia-NTG to 13N-ammonia baseline to detect viability on 18F-FDG PET in all dysfunctional segments. Ratio = ratio of 13N-ammonia-NTG to 13N-ammonia baseline; NTG = 13N-ammonia-NTG; rest = 13N-ammonia baseline.
According to ROC curve analysis, a ratio of 1.1 for 13N-ammonia-NTG to 13N-ammonia baseline was the optimal cutoff value for detection of segmental viability, with an AUC of 0.92 ± 0.030. Application of this cutoff value resulted in a sensitivity of 82% and a specificity of 100% (P < 0.005 vs. 13N-ammonia baseline and 13N-ammonia-NTG; Fig. 2).
When only akinetic and dyskinetic segments were considered, ROC curve analysis of 13N-ammonia baseline resulted in an AUC of 0.51 ± 0.12; the optimal cutoff level was 0.47 mL/min/g, yielding a sensitivity of 67% and a specificity of 50%. ROC curve analysis of 13N-ammonia-NTG resulted in an AUC of 0.77 ± 0.10; the optimal cutoff level was 0.50 mL/min/g, providing a sensitivity of 83% and a specificity of 67% (P < 0.01 vs. the 13N-ammonia baseline; Fig. 3). According to ROC curve analysis, a ratio of 1.1 for 13N-ammonia-NTG to 13N-ammonia baseline was the optimal cutoff value for detection of segmental viability, with an AUC of 0.86 ± 0.083. Application of this cutoff value resulted in a sensitivity of 75% and a specificity of 100% (P < 0.02 vs. 13N-ammonia baseline and 13N-ammonia-NTG; Fig. 3).
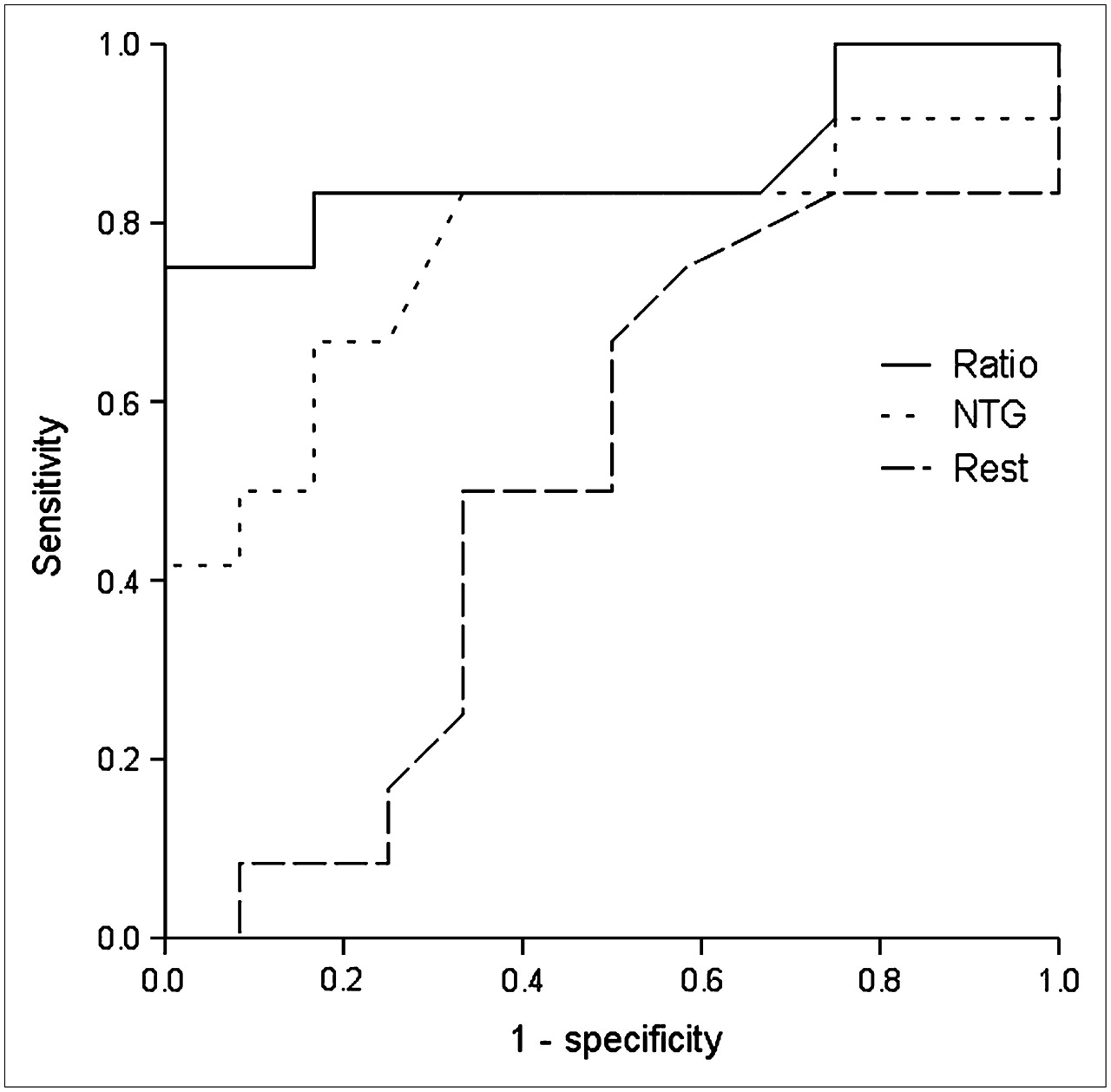
ROC curves of 13N-ammonia baseline, 13N-ammonia-NTG, and ratio of 13N-ammonia-NTG to 13N-ammonia baseline to detect viability on 18F-FDG PET in akinetic or dyskinetic segments. Ratio = ratio of 13N-ammonia-NTG to 13N-ammonia baseline; NTG = 13N-ammonia-NTG; rest = 13N-ammonia baseline.
DISCUSSION
This dynamic 13N-ammonia PET study demonstrated that in patients with chronic ischemic LV dysfunction, the sublingual administration of nitrates significantly increased blood flow in viable myocardium; this increase was not observed in nonviable myocardium. Nitrate use during myocardial perfusion imaging improves the assessment of myocardial viability.
These observations support the routine use of nitrates in combination with SPECT for the assessment of viable myocardium. The observation that nitrates are useful for the detection of viable myocardium is not new. By the 1970s, various studies evaluating improvement in LV function (as a marker of viable myocardium) after nitrate administration had already been undertaken in the cardiac catheterization laboratory. In particular, Mehmel et al. (12) demonstrated, in 12 patients, a significant improvement in LV ejection fraction (from 43% ± 12% to 47% ± 13%, P < 0.05) after nitrate administration. Moreover, Helfant et al. (13) reported an improvement in regional contractile function after revascularization in segments showing a functional improvement after nitrate administration. A histopathologic study subsequently demonstrated that myocardium showing a functional improvement after nitrate administration contained significantly less fibrosis than did myocardium not showing such an improvement (14).
It is hypothesized that viable myocardium is severely hypoperfused, resulting in downregulation of function. After nitrate administration, myocardial blood flow is augmented to these severely hypoperfused regions, resulting in an improvement of contractile function, as demonstrated in the studies just described.
This concept has been extrapolated to the assessment of viability with current nuclear techniques. Sciagra et al. (15–18) have reported extensively on the use of nitrates in combination with 99mTc-sestamibi SPECT. Those authors demonstrated that regions considered nonviable on resting SPECT, with severely decreased tracer uptake, did in fact exhibit a significantly higher tracer uptake (indicating viable myocardium) after nitrate administration. This increased tracer uptake was explained by the nitrate-augmented blood flow to severely hypoperfused but viable regions, permitting increased tracer delivery and uptake. Subsequent studies have shown that nitrate-enhanced SPECT with 99mTc-sestamibi allows the accurate prediction of functional recovery after revascularization. For example, Bisi et al. (19) showed a clear reduction in defect size on 99mTc-sestamibi SPECT after nitrate administration in patients undergoing revascularization; however, the reduction in defect size was observed only in patients showing recovery of function after revascularization. Thus, nitrate administration before SPECT will result in a superior detection of viable myocardium. This finding is also supported by the pooled findings of other studies, available in the literature, on the prediction of functional outcome after revascularization with 99mTc-sestamibi SPECT (20). Pooling of 13 studies (with 308 patients) using 99mTc-sestamibi SPECT without nitrate administration demonstrated a sensitivity of 79% and a specificity of 58%. Pooling of 7 studies (with 180 patients) using nitrate-enhanced 99mTc-sestamibi SPECT revealed a significantly higher sensitivity (86%) and a comparable specificity (83%).
Although the concept that nitrate-enhanced blood flow results in superior detection of viability is attractive, quantitative data on changes in blood flow after nitrate administration are scarce. Two studies have evaluated changes in blood flow after nitrate administration. Fallen et al. (21) performed an elegant 13N-ammonia PET study on patients with ischemic heart disease and demonstrated that nitrate administration increased blood flow to ischemic myocardium by more than 25% (compared with 24% in the current study). The patients, however, had normal LV function, and whether changes in blood flow occurred in chronically dysfunctional myocardium could not be determined. Tadamura et al. (22) studied 23 patients with chronic ischemic LV dysfunction and demonstrated that nitrate administration was associated with increased 201Tl uptake in viable segments, although 15O-water PET demonstrated no changes in blood flow. Coronary vascular resistance, however, showed a significant decrease, which may explain the increase in 201Tl uptake.
The current study was specifically designed to evaluate whether myocardial blood flow increased after nitrate administration in chronically dysfunctional but viable myocardium. The results clearly demonstrated a significant increase in myocardial blood flow after nitrate administration. In addition, ROC curve analysis indicated that the ratio of nitrate-enhanced flow to resting flow better predicted viability in dysfunctional myocardium (also when akinetic and dyskinetic segments were considered separately) than did either resting flow or nitrate-enhanced flow. These findings indicate that it is not so much the absolute level of blood flow, but rather the augmentation of flow after nitrates, that is superior in the prediction of viability. Our results demonstrate a clear increase in blood flow after nitrate administration, whereas this increase was not observed by Tadamura et al. (22). These discrepant findings may be related to differences in study populations, study protocols, flow tracers, or methods of data analysis.
For clinical purposes, nitrate-enhanced SPECT using a 99mTc-labeled agent is adequate for the detection of viable myocardium, and PET to determine absolute flow may not be needed. The current observations, however, provide further evidence supporting the use of nitrate-enhanced SPECT with 99mTc-labeled tracers for the detection of viability.
Some limitations of the present study need attention. First, the patients did not undergo revascularization, and improvement of function could not be evaluated. Second, larger patient populations and, particularly, patients with severely depressed LV ejection fraction need to be studied to confirm the current findings. Third, nitrate was administered sublingually, and whether transdermal or intravenous administration has comparable effects remains to be studied.
CONCLUSION
Nitrate-enhanced 13N-ammonia PET increased myocardial blood flow in viable myocardium, whereas blood flow remained unchanged in nonviable myocardium. The ratio of nitrate-enhanced flow to resting flow was the best predictor of viability, yielding a sensitivity of 82% and a specificity of 100%.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication March 15, 2006.
- Accepted for publication April 21, 2006.





{kind=link}
{kind=link}
{kind=link}