


Abstract
Fine-needle aspiration biopsy (FNAB) is inconclusive in up to 20% of patients with solitary thyroid nodules. In these cases, hemithyroidectomy is necessary, but only 20% of the nodules prove to be thyroid carcinoma. The aim of this study was to explore the potential of 18F-FDG PET to reduce the number of unnecessary hemithyroidectomies in the preoperative assessment of thyroid nodules with inconclusive FNAB results. Methods: Forty-four consecutive patients, scheduled for hemithyroidectomy because of inconclusive FNAB findings, participated in this prospective study. 18F-FDG PET of the thyroid region was performed before hemithyroidectomy, and standardized uptake values were calculated. The final histopathologic diagnosis served as a standard of reference. Results: Histopathologic examination of the surgical specimens revealed 7 well-differentiated thyroid carcinomas in 6 patients, all accumulating 18F-FDG (negative predictive value, 100%). 18F-FDG accumulated in 13 of 38 benign nodules. The pre-PET probability for cancer in this study population was 14% (6/44), and the post-PET probability increased to 32% (6/19). The percentage of unnecessary hemithyroidectomies in a hypothetical algorithm using 18F-FDG PET was only 30% (13/44), compared with 86% (38/44) without 18F-FDG PET. 18F-FDG PET reduced the number of futile hemithyroidectomies by 66% (25/38) (95% confidence interval, 49%–80%; Fisher's exact test, P = 0.0038). Semiquantitative analysis using standardized uptake values did not help to further reduce this number. Conclusion: In addition to data in the literature demonstrating accurate detection of thyroid cancer by 18F-FDG PET, this study showed that 18F-FDG PET should play an important role in the management of patients with inconclusive cytologic diagnosis of a thyroid nodule. 18F-FDG PET reduced the number of futile hemithyroidectomies by 66%. Although PET is a relatively costly procedure, this cost outweighs the costs and risks associated with unnecessary thyroid surgery.
Solitary thyroid nodules are quite common, with a prevalence of 4%–7% in the adult population of the United States (1). The incidence of differentiated thyroid cancer, however, is only 40 cases per million per year (2). The major diagnostic challenge in the work-up of the large number of patients with thyroid nodules is to select for surgery only those patients with malignant nodules.
Clinical findings that should raise a suspicion of malignancy include rapidly growing nodules, firm or hard nodules, regional lymphadenopathy, and local invasion in the neck (3). Radionuclide scanning is not recommended for routine use, because thyroid scintigraphy does not significantly decrease the number of suggestive nodules (3), and most patients would also undergo fine-needle aspiration biopsy (FNAB) in such a diagnostic algorithm (2). Characteristics revealed by ultrasonography, such as hypoechogenicity, microcalcifications, irregular margins, increased nodular flow on Doppler sonography, and, especially, evidence of invasion or regional lymphadenopathy, are associated with an increased risk of cancer. Sonographic findings, however, cannot reliably distinguish between benign and cancerous lesions (3–5). Thyroid function testing may be helpful in differential diagnosis. Nearly all patients with thyroid cancer are euthyroid (1).
FNAB, preferably guided by ultrasonography, has to be regarded as the key investigation in the initial evaluation of thyroid nodules (6). Patient management decisions and choice of therapy will be based mainly on the cytologic diagnosis. FNAB is safe, easily performed, without major complications, and cost-effective. Although the minimal tumor size detectable by ultrasound-guided FNAB is about 5 mm, it has a high negative predictive value of 98% (7). Patients with nonmalignant cytologic types can therefore be followed safely by sonography, as long as the thyroid nodule size remains constant. FNAB, however, does also have several recognized limitations. FNAB shows inconclusive aspirates in up to 20% of cases (8,9). In patients with cytologic findings characteristic of a follicular or Hürthle cell neoplasm or Hashimoto's thyroiditis, hemithyroidectomy is necessary for a reliable histologic diagnosis (2,10). Although routine FNAB clearly increases the relative number of cancers at operation, still 80%–85% of hemithyroidectomized patients eventually turn out to have benign thyroid disease (2,10). A diagnostic test that decreases the number of surgical procedures for benign nodules could have a significant impact on patient management.
In differentiated papillary and follicular thyroid cancer, PET with 18F-FDG has been useful for surveillance and detection of recurrence, especially in thyroid cancer patients with negative findings on 131I whole-body scanning but measurable thyroglobulin. 18F-FDG PET is able to detect metastatic disease in up to 90% of these patients (11). In patients with medullary thyroid cancer and elevated calcitonin levels after thyroidectomy, 18F-FDG PET has a sensitivity of 70%–75% for localizing metastatic disease (11). The current prospective study explored the potential of 18F-FDG PET to reduce the number of unnecessary hemithyroidectomies performed for solitary thyroid nodules that have inconclusive FNAB results and ultimately prove to be benign.
MATERIALS AND METHODS
Patients
Patients scheduled for hemithyroidectomy for a palpable solitary thyroid nodule with inconclusive FNAB findings were eligible for this prospective study. The study was conducted in a general hospital (bed capacity, 450) and a university hospital (bed capacity, 950) in The Netherlands. In our practice, inconclusive cytologic findings are encountered in 20% of patients with a suggestive thyroid nodule. Forty-four consecutive patients with a mean age of 50 y (range, 22–77 y) were enrolled from June 2001 to December 2004 (Table 1). All patients were euthyroid. Exclusion criteria were diabetes mellitus and pregnancy. The study was approved by the Institutional Review Board of the Radboud University Nijmegen Medical Centre, and written informed consent was obtained from each patient.
Characteristics and Cytologic, Histopathologic, and 18F-FDG PET Results for 44 Patients with Thyroid Nodules with Inconclusive FNAB Results
Diagnostic Work-up of Thyroid Nodules
If a suggestive thyroid nodule was observed, the initial diagnostic study was FNAB. A suggestive nodule was defined as a nodule in a patient with a family history of medullary thyroid carcinoma or multiple endocrine neoplasia, a rapidly growing nodule, a firm or hard nodule, a nodule fixed to adjacent structures, or a nodule detected in combination with paralysis of one or both vocal cords or regional lymphadenopathy. A moderately suggestive nodule was defined as a nodule in a patient either younger than 20 y or older than 70 y, a nodule in a male patient or in a patient with a history of head and neck irradiation, a nodule more than 4 cm in diameter, a partially cystic nodule, or a nodule producing symptoms of compression, including dysphagia, dysphonia, hoarseness, dyspnea, or cough. If cytologic examination revealed malignancy, a total thyroidectomy was performed. If the cytologic diagnosis was unequivocally benign, the patient remained under observation. In cases of an inconclusive cytologic finding or if malignancy could not be excluded, the patients underwent hemithyroidectomy to allow a reliable histologic diagnosis. Cytologic findings were considered inconclusive if they were suggestive of a follicular neoplasm or a Hürthle cell (oncocytic) neoplasm, if they showed atypical papillary cells, or if the sample was repeatedly insufficient (nondiagnostic).
Experimental Design
18F-FDG PET was performed only on those patients scheduled for hemithyroidectomy on the basis of inconclusive cytology. The interval between FNAB and 18F-FDG PET was at least 5 wk to avoid 18F-FDG accumulation due to the biopsy trauma.
A dedicated PET scanner (ECAT-EXACT; Siemens/CTI) was used for data acquisition. Before 18F-FDG injection, patients fasted for at least 6 h. Intake of sugar-free liquids was permitted. Immediately before the procedure, patients were given diazepam, 5 mg, for muscle relaxation. One hour after intravenous injection of 200–220 MBq of 18F-FDG (Mallinckrodt Medical), emission and transmission images of the head and neck area were acquired (2 bed positions, 10 min per bed position). The images were corrected for attenuation and reconstructed using the ordered-subsets expectation maximization algorithm.
Evaluation of Data
The images were evaluated independently by 2 experienced observers. These observers were not aware of the location of the nodule or of the final histologic diagnosis. The scans were classified as negative (no 18F-FDG uptake in the thyroid nodule) or as positive (any 18F-FDG uptake in the thyroid nodule above background activity). If 18F-FDG PET revealed the thyroid nodule, standardized uptake values (SUVs) were calculated for semiquantitative analysis of 18F-FDG uptake. If the thyroid nodule was not visible on the 18F-FDG PET images, no quantification was attempted. A volume of interest was drawn around visible nodules using an automatic 50% isocontour (ECAT software tool), which enclosed pixels with 50% or more of the maximum radioactivity in the volume of interest. SUVs were calculated using the concentration of 18F-FDG in the volume of interest as measured by PET, divided by the injected 18F-FDG dose and multiplied by body weight as a normalization factor.
After 18F-FDG PET, all patients underwent hemithyroidectomy and the final histopathologic diagnosis of the nodules was determined. This diagnosis was regarded as the standard of reference and was used for verification of the 18F-FDG PET results.
Statistical Analysis
When designing the study, we included a power analysis to estimate the required size of the patient population. Data from the literature suggest that only 15%−20% of patients with inconclusive FNAB results for palpable thyroid nodules have thyroid cancer (2,10). Thus, 80%−85% of patients are resigned to unnecessary hemithyroidectomy to rule out malignancy. Detection of a 30% reduction in unnecessary hemithyroidectomies as a result of inclusion of 18F-FDG PET in the preoperative diagnostic work-up requires a sample size of 42 patients (α, 0.05; power, 0.80). The results of the study were analyzed using the Fisher exact test. The level of significance was set at 0.05.
RESULTS
FNAB
FNAB yielded cytologic specimens with follicular proliferation in 33 patients, cytologic specimens with numerous Hürthle cells in 4 patients, and a combination of numerous Hürthle cells and follicular cells in 5 patients (Table 1). In 2 patients, 3 repetitive FNABs obtained an insufficient number of cells to allow a correct cytologic interpretation. Thyroid cancer could not be excluded in any of these patients, and they were thus scheduled for hemithyroidectomy.
Histopathologic and 18F-FDG PET Results
Histopathologic examination of the surgical specimens revealed 7 well-differentiated thyroid carcinomas in 6 of the 44 patients: 2 patients with papillary carcinoma, 3 patients with follicular carcinoma, and 1 patient (patient 43, Fig. 1) with 2 primaries in 1 lobe (a palpable large follicular carcinoma and a small papillary carcinoma) (Table 1). All malignant tumors accumulated 18F-FDG and were clearly visible as areas of increased 18F-FDG uptake. Therefore, there were no false-negative results, implying a negative predictive value of 100% (95% confidence interval, 86%–100%). The nodules of 38 of the 44 patients were histologically benign. Histologic examination of these benign nodules revealed nodular hyperplasia in 13, follicular adenoma in 15, Hashimoto's thyroiditis in 7, and a Hürthle cell adenoma in 3. 18F-FDG accumulated in 13 of the 38 histologically benign tumors: 1 of 13 hyperplastic nodules, 5 of 15 follicular adenomas, 4 of 7 cases of Hashimoto's thyroiditis, and all 3 Hürthle cell adenomas (Fig. 2). The remaining 25 patients did not show increased tracer uptake in the thyroid. The number of unnecessary hemithyroidectomies in the diagnostic algorithm in which 18F-FDG PET was implemented was 13 (30%) of 44, compared with 38 (86%) of 44 in the algorithm without 18F-FDG PET. The implication is that 18F-FDG PET can reduce the number of needless hemithyroidectomies by 66% (25/38) (95% confidence interval, 49%–80%; Fisher's exact test, P = 0.0038). The pre-PET probability of cancer in the patients scheduled for hemithyroidectomy was 14% (6/44), and the post-PET probability increased to 32% (6/19). Figure 3 shows the proposed diagnostic work-up including 18F-FDG PET.

In this 38-y-old woman, FNAB showed follicular proliferation. 18F-FDG PET demonstrated 2 lesions in right thyroid lobe. Final histopathologic diagnosis revealed right-sided pT3 follicular thyroid carcinoma and pT1 papillary thyroid carcinoma cranial from this lesion.
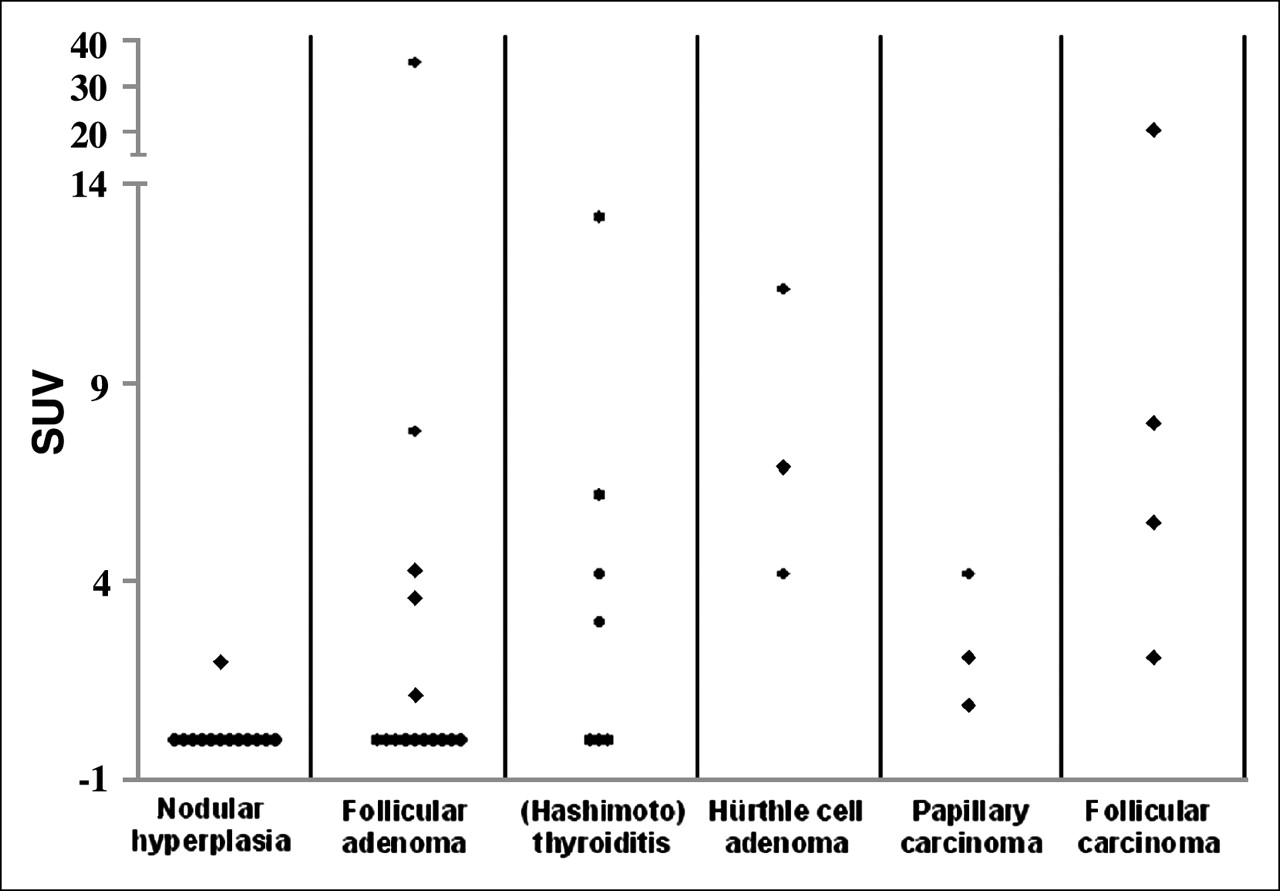
18F-FDG SUV for all 44 patients plotted against final histologic diagnosis. In this plot, SUV of invisible nodules on 18F-FDG PET was set at zero. SUV did not help to separate malignant from benign lesions, as indicated by distinct overlap.

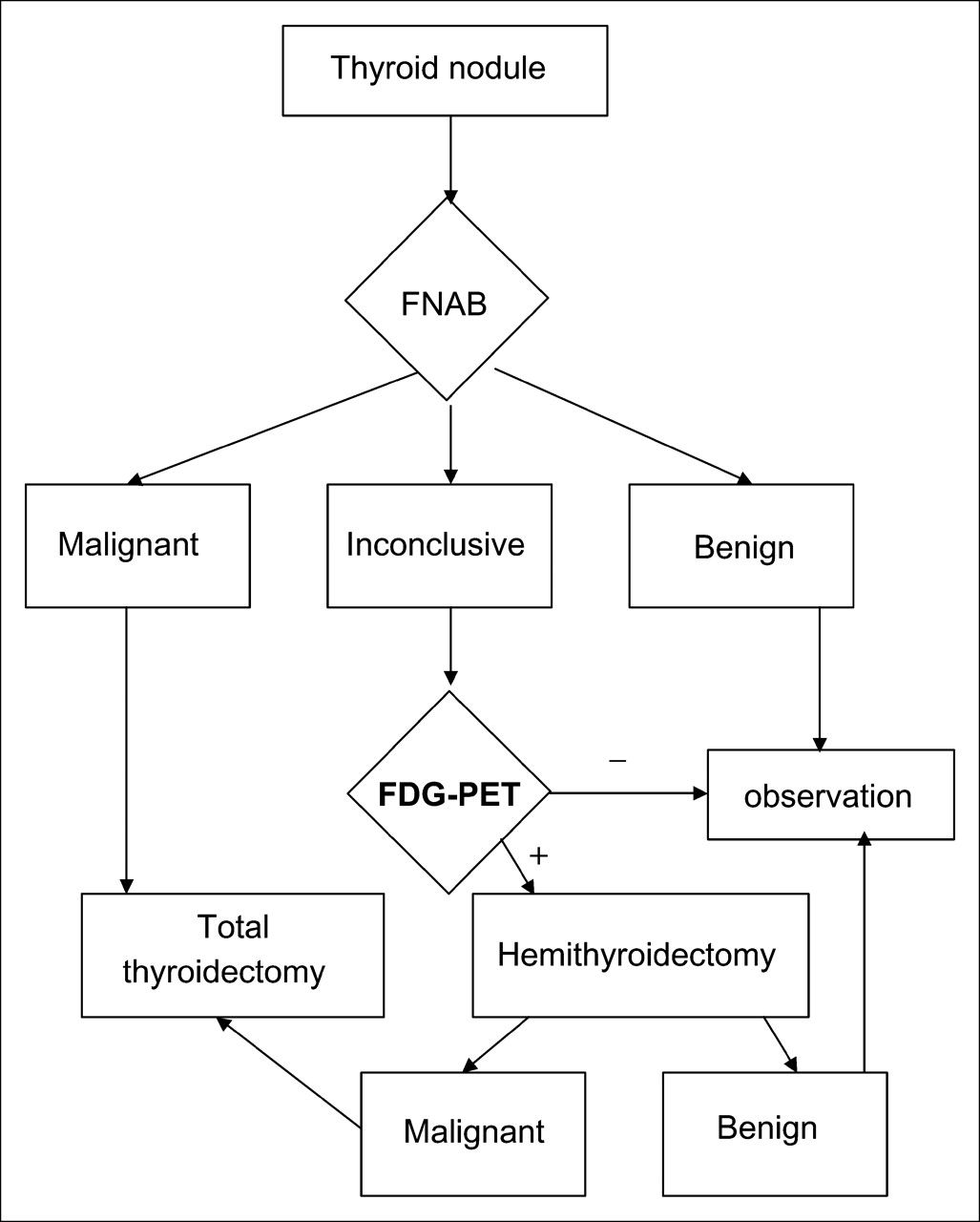
Diagnostic algorithm including 18F-FDG PET. In existing diagnostic algorithm, nodules with inconclusive cytologic diagnosis must be removed, and hemithyroidectomy is necessary to allow reliable histologic diagnosis. In proposed diagnostic algorithm, 18F-FDG PET is implemented as shown.
Semiquantitative Analysis
All carcinomas were clearly visible on 18F-FDG PET images. The mean SUV of the carcinomas was 6.2 ± 6.7 (range, 0.9–20.4; Table 1). The mean SUV of the benign lesions with increased 18F-FDG uptake was similar (7.9 ± 8.9; range, 1.1–35.1). In Figure 2, SUV plots of the various histologic diagnoses are shown. The SUVs of PET-negative nodules were set at zero. This figure demonstrates that SUV did not help to separate malignant lesions from benign lesions, as indicated by a distinct overlap. The mean SUVs of the 18F-FDG PET–positive nodules in the patients with follicular adenoma, Hashimoto's thyroiditis, nodular hyperplasia, and Hürthle cell adenoma were 10.4 ± 14.0, 6.6 ± 4.5, 2.0, and 7.5 ± 3.6, respectively. All patients with Hürthle cell adenoma had increased focal 18F-FDG uptake in the thyroid (Fig. 4). Twelve of 13 lesions with nodular hyperplasia, 10 of 15 with follicular adenoma, and 3 of 7 with Hashimoto's thyroiditis showed no visual 18F-FDG uptake in the thyroid nodules.

This 42-y-old woman (patient 37) had inconclusive findings, with many atypical Hürthle cells, on FNAB. 18F-FDG PET showed intensely increased 18F-FDG uptake in right thyroid lobe. Histologic examination demonstrated 2.7-cm follicular adenoma with focal Hürthle cell changes.
DISCUSSION
The present study showed that the number of futile hemithyroidectomies in an algorithm that includes 18F-FDG PET could be reduced by 66%. 18F-FDG PET is able to increase the probability that cases of cancer will be revealed when the FNAB findings for those cases are inconclusive; the pre-PET probability of cancer in this study population was 14% (6/44), and the post-PET probability increased to 32% (6/19). 18F-FDG PET missed none of the 7 differentiated thyroid carcinomas, implying a negative predictive value of 100%. The findings of 18F-FDG PET were not negative for all benign nodules: 18F-FDG accumulated in 13 of the 38 histologically benign tumors. Nevertheless, our study proved that 18F-FDG PET is helpful in the selection of patients who need surgery. If 18F-FDG PET were implemented in the preoperative work-up for patients with inconclusive cytologic results, the number of futile hemithyroidectomies would decrease substantially. Such a strategy not only would avoid the risks and morbidity associated with thyroid surgery but also would lead to cost savings. The reimbursement for 18F-FDG PET in The Netherlands is approximately €1,200, which compares favorably with the results from a recent cost analysis performed in The Netherlands by Hooft et al. (12). They showed that the costs were driven mainly by the costs of surgery and hospitalization, with mean costs per patient amounting to €3,311 in benign cases, without considering additional-treatment costs, economic costs, or indirect costs.
The high negative predictive value shown by the current prospective study is in line with the findings of various other small, retrospective studies (2,13–15) and studies with varying degrees of selection bias (16–18). These studies included a total of 58 thyroid carcinomas, of which only 1 was missed with 18F-FDG PET—in a study that did not use a modern dedicated PET camera (16). Another nuclear medicine technique, dual-phase 99mTc-sestamibi, did not provide such a high negative predictive value. Thirteen studies (19–24) that reported on this issue included 210 thyroid carcinomas altogether, of which 39 were missed with 99mTc-sestamibi scintigraphy. Like 18F-FDG PET, 99mTc-sestamibi scintigraphy may also show accumulation in follicular adenomas, Hürthle cell adenomas, and Hashimoto's thyroiditis and thus would not be helpful in raising specificity (19–24). Also, further nuclear medicine methods such as 99mTc-tetrofosmin, 201Tl, or 201Tl/99mTc-pertechnetate subtraction scanning have shown similar disappointing results (25).
Furthermore, the current study is unique in that an unselected and uniform population of consecutive patients with inconclusive FNAB findings was prospectively investigated with sufficient power to draw reliable conclusions. Wolf et al. (15) studied patients retrospectively, and Joensuu et al. (16) and Sasaki et al. (18) selected patients with thyroid carcinoma and benign thyroid tumors, respectively. Sasaki et al. studied not only new preoperative cases but also recurrent or metastatic carcinoma. Kresnik et al. (17) studied 43 patients with suggestive cytologic results but selected patients with papillary carcinoma as a positive control group. More important, the study population did not represent the general population, because the study was performed in an area endemic for goiter. The studies of Adler et al. (13), Bloom et al. (2), and Uematsu et al. (14) were too small to achieve sufficient power. In contrast to our findings, the findings of these studies suggested that a higher 18F-FDG uptake in malignant tumors than in benign lesions, as determined by quantitative analysis (i.e., SUV), is able to differentiate successfully between all benign and malignant thyroid nodules. Kresnik et al. and Sasaki et al. also reported many overlapping cases. SUVs depend on acquisition, reconstruction, and region-of-interest parameters. The variability in SUV methodology will hamper direct comparison of results obtained in different studies (26). Furthermore, the partial-volume effect is an additional source of potential error in quantifying 18F-FDG activity in tissue. When the size of the region of interest is smaller than approximately twice the full width at half maximum, 18F-FDG accumulation in the region of interest is underestimated (17,18). For all these reasons, we recommend that SUVs not be relied on in the discrimination between malignant and benign thyroid lesions. Patients with a suggestive thyroid nodule and inconclusive FNAB findings, in combination with any visible 18F-FDG accumulation in the thyroid nodule, should be taken to surgery.
Concerns may arise from the limited spatial resolution of PET. PET will probably never be able to rule out microscopic thyroid carcinoma. However, this is probably not a significant clinical problem, because it is generally supposed that thyroid carcinomas smaller than 1 cm are rarely of clinical significance. This supposition has been confirmed by large autopsy series demonstrating a high prevalence of incidental and unrecognized minimal (occult) thyroid carcinomas (27–29).
Our study may also be of importance for interpretation of increased 18F-FDG uptake in the thyroid region in a patient investigated with 18F-FDG PET for any other indication. Thyroid incidentalomas identified by 18F-FDG PET occur with a frequency of 2.3% (30–32). A study by Cohen et al. showed that, of the 102 incidentalomas found in 4,525 18F-FDG PET examinations, half that underwent biopsy were malignant (30). Therefore, 18F-FDG PET–positive thyroid incidentalomas should not be overlooked and should prompt further investigation to rule out cancer—of course, only when the diagnosis of thyroid cancer would influence patient outcome and management.
CONCLUSION
In addition to data in the literature demonstrating accurate detection of thyroid cancer by 18F-FDG PET, this study showed that 18F-FDG PET should play an important role in the management of patients with inconclusive cytologic diagnosis of a thyroid nodule. 18F-FDG PET reduced the number of futile hemithyroidectomies by 66%. Although PET is a relatively costly procedure, this cost outweighs the costs and risks associated with unnecessary thyroid surgery.
Acknowledgments
This study was funded with internal resources. The funding source was not involved with study design and conduct; the collection, management, analysis, or interpretation of data; the writing of the report; or the decision to submit the paper for publication.
References
- Received for publication December 2, 2005.
- Accepted for publication January 24, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Thyroid nodules with indeterminate cytology: prospective comparison between 18F-FDG-PET/CT, multiparametric neck ultrasonography, 99mTc-MIBI scintigraphy and histology
- IMAGING IN ENDOCRINOLOGY: 2-[18F]-fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography in differentiated thyroid carcinoma: clinical indications and controversies in diagnosis and follow-up
- The role of 18F-fluorodeoxyglucose positron emission tomography in differentiated thyroid cancer before surgery
- The Role of 18F-Fluorodeoxyglucose Positron Emission Tomography in Thyroid Neoplasms
- Hybrid SPECT-CT and PET-CT imaging of differentiated thyroid carcinoma
- Incidental thyroid nodule
- The role of F-18-fluorodeoxyglucose positron emission tomography in the postoperative evaluation of differentiated thyroid cancer
- 18F-FDG PET of Thyroid Nodules with Inconclusive Cytologic Results
- Reply: 18F-FDG PET of Thyroid Nodules with Inconclusive Cytologic Results.