


Abstract
Earlier investigations showed that N-isopropyl-p-123I-iodoamphetamine SPECT (123I-IMP SPECT) is useful for the diagnosis of uveal malignant melanoma, whereas the feasibility and usefulness of 18F-FDG PET in uveal malignant melanoma have not yet been established. We compared the usefulness of 123I-IMP SPECT and 18F-FDG PET for the detection of uveal malignant melanoma on the same subjects. Methods: Nineteen patients (10 men, 9 women) with suspected uveal malignant melanoma were examined by 123I-IMP SPECT. Thirteen of them were also examined by 18F-FDG PET. 123I-IMP SPECT was performed at 15 min or at 3 and 24 h after intravenous administration of 123I-IMP. Results: In 12 of 19 study patients, 123I-IMP SPECT obtained at 24 h after intravenous administration of 123I-IMP delineated an area of increased uptake in the site corresponding to the ocular tumor. All of the ocular tumors in the 12 123I-IMP SPECT–positive patients were confirmed histopathologically and clinically to be uveal malignant melanoma. The other 7 123I-IMP-SPECT–negative patients have been monitored under the diagnosis of choroidal nevus, choroidal hemangioma, hyperplasia of the pigment epithelium of the retina, or idiopathic inflammatory lesions without any complications. In a total of 13 patients examined by 18F-FDG PET, 9 of whom were 123I-IMP SPECT positive and 4 were negative, only 1 patient showed abnormal uptake of 18F-FDG PET in the site corresponding to the ocular tumor. Therefore, 8 of 9 patients with uveal malignant melanoma showed false-negative results in 18F-FDG PET. The 18F-FDG PET–positive patient with uveal malignant melanoma had the largest tumor mass with a short diameter of 12 mm, a long diameter of 17 mm, and a height of 7 mm. In the other 8 18F-FDG PET–negative patients, the tumors had a dimension of 11 × 13 × 7 mm or less. Conclusion: 123I-IMP SPECT is a sensitive and accurate method for the detection of uveal malignant melanoma, whereas the efficacy of 18F-FDG PET for this purpose is low because of a high incidence of false-negative results. 123I-IMP SPECT is far more superior in comparison with 18F-FDG PET in detecting uveal malignant melanoma.
Uveal melanoma, which is the most common primary intraocular malignant neoplasm in adults (1), has been reported to occur in 6–7 cases per million in caucasians (1–3) or 4.3 cases per million in the United States, most of which occurred in the white population (4). In contrast, the annual incidence of uveal melanoma in Japan was 0.25 per million (5).
It was shown that the typical uveal melanoma signal in MRI was found in 69.4% (6). It was also shown that contrast CT could diagnose uveal melanoma in 75% of patients with 2.5- and 3-mm prominence, whereas in the noncontrast CT it was only evident in 34% (7).
A number of earlier reports showed that N-isopropyl-p-123I-iodoamphetamine (123I-IMP) scintigraphy was useful for the detection of primary and metastatic lesions of cutaneous malignant melanoma (8–14). Moreover, 123I-IMP scintigraphy has been shown to be useful also for the detection of uveal malignant melanoma (15–18). These studies, except for 1 study reported in 1988 (15), were the results of imaging using 123I-IMP SPECT (16–18). 123I-IMP is incorporated into melanocytes actively producing melanin.
On the other hand, according to more recent studies, 18F-FDG PET does not seem to be sensitive enough for the diagnosis of uveal malignant melanoma (19–21), despite the fact that it is a sensitive and accurate method for detecting primary and metastastic lesions of cutaneous malignant melanoma (22–28). The reason for this discrepancy in the efficacies of 18F-FDG PET for the detection of cutaneous and uveal malignant melanomas has not yet been elucidated.
We have compared the usefulness of 123I-IMP SPECT and 18F-FDG PET for the detection of uveal malignant melanoma on the same patients to determine the diagnostic value of the latter in this disease.
MATERIALS AND METHODS
Subjects
All procedures followed the clinical study guidelines of Nagoya University Hospital and were approved by the Institutional Review Board. Written consent was obtained after a complete description of the study for all patients and their relatives. Nineteen patients with suspected uveal malignant melanoma (10 men, 9 women; mean age ± SD, 62 ± 10.7 y; age range, 38–76 y) were examined by 123I-IMP SPECT. Thirteen (8 men, 5 women; mean age ± SD, 60 ± 12.1 y; age range, 38–71 y) of them were also examined by 18F-FDG PET. None of them had diabetes mellitus.
In 12 of 19 patients, the ocular tumor was diagnosed histopathologically and clinically as malignant melanoma. Six patients have been monitored under the diagnosis of choroidal nevus, choroidal hemangioma, hyperplasia of the pigment epithelium of the retina, or idiopathic inflammatory lesions without expansion and exacerbation of the lesions. In the other 1 patient, the lesion was very small (<1 mm) and considered as benign, and its diagnosis has been unknown.
In 7 of the 12 patients with uveal malignant melanoma, extirpations of the affected eyes were performed; in 3 patients, laser thermotherapy was performed; and in 1 patient, heavy-particle radiotherapy was performed. In 1 patient (patient 14), laser thermotherapy was primarily performed and then γ-knife radiosurgery was performed for residual melanoma tissues. The patients have been monitored carefully to check for a recurrence of the disease.
SPECT Procedure
123I-IMP (Nihon Medi-Physics, Ltd.; Daiichi Radioisotope Laboratories, Ltd.), 167 MBq (4.5 mCi), was injected intravenously while the patients were in a supine position with eyes closed in a quiet and dimly lit room. SPECT was performed between 5 and 30 min after injection using a triple-head GCA 9300A γ-camera (Toshiba) equipped with low-energy, high-resolution, and fanbeam collimators. The data were acquired in a matrix of 128 × 128 through a 120° rotation at an angle interval of 4°. The projection data were prefiltered through a Butterworth filter and then reconstructed using an ordered-subsets expectation maximization (OSEM) reconstruction with 2 iterations and 10 subsets. No attenuation correction was performed. The in-plane spatial resolution was 8-mm full width at half maximum (FWHM). The final image slices were set up parallel to the orbitomeatal line (OM line) and were obtained at an interval of 6.9 mm through the entire brain. 123I-IMP scintigraphy was performed at 15 min or at 3 and 24 h after intravenous administration of 123I-IMP.
PET Procedure
PET scanning was performed using 18F-FDG. The patients fasted for at least 6 h. Tissue attenuation of annihilation photons was corrected by transmission scans using a rotating 68Ge/68Ga line source. A 10-min transmission scan was performed before injection of 18F-FDG. A 20-min emission scan was started 40 min after injection of 185−204 MBq (5−5.5 mCi) of 18F-FDG. With 1 of 13 patients to be examined by PET, the 15-min emission scan that started 3 h after an injection of 18F-FDG was also performed, because an earlier study showed that delayed 18F-FDG PET was a better and more reliable imaging protocol for tumor detection (29). A Headtome-V PET camera (Shimadzu Co.) was used for the study with a spatial resolution of 4.5-mm (axial) and 3.9-mm (transaxial) FWHM at the center of the fields of view. It provides 47 sections with a center-to-center distance of 3.125 mm. Twenty-three axial images were obtained with a thickness of 6.25 mm parallel to the OM line, starting from just the OM line. Reconstructed images were obtained by an OSEM reconstruction with 2 iterations and 16 subsets.
RESULTS
The summaries of the 19 study patients with suspected uveal malignant melanoma are shown in Tables 1 and 2.
Patient Profile and Uptake in SPECT and PET
Tumor Size, Patient Treatment, and Final Diagnosis
In 12 of 19 patients, 123I-IMP SPECT obtained at 24 h after an intravenous administration of 123I-IMP delineated an area of increased uptake of 123I-IMP in the site corresponding to the ocular tumor. In all of the twelve 123I-IMP-SPECT–positive patients, the ocular tumor was diagnosed histopathologically and clinically as malignant melanoma. Only 2 of these 123I-IMP-SPECT–positive patients showed an increased uptake of 123I-IMP at 3 h after intravenous administration of 123I-IMP. These 2 patients showing the uptake of 123I-IMP at 3 h are patients 10 and 13 in Tables 1 and 2. Tumor size was relatively large in both patients.
Six of the seven 123I-IMP-SPECT–negative patients have been monitored under the diagnoses other than malignant. In the 1 other 123I-IMP-SPECT–negative patient (patient 12), the lesion was very small and its diagnosis has been unknown.
In the 13 patients who underwent 18F-FDG PET, 9 were 123I-IMP positive and 4 negative. In contrast, only 1 patient (patient 10) showed an abnormal uptake of 18F-FDG PET in the site corresponding to the ocular tumor. In patient 13, delayed (3 h) 18F-FDG PET scanning was also performed but both early and delayed 18F-FDG PET images were negative. The images of the ocular tumors by 123I-IMP SPECT, 18F-FDG PET, and other radiologic methods in patients 1 and 13 are shown in Figures 1 and 2.

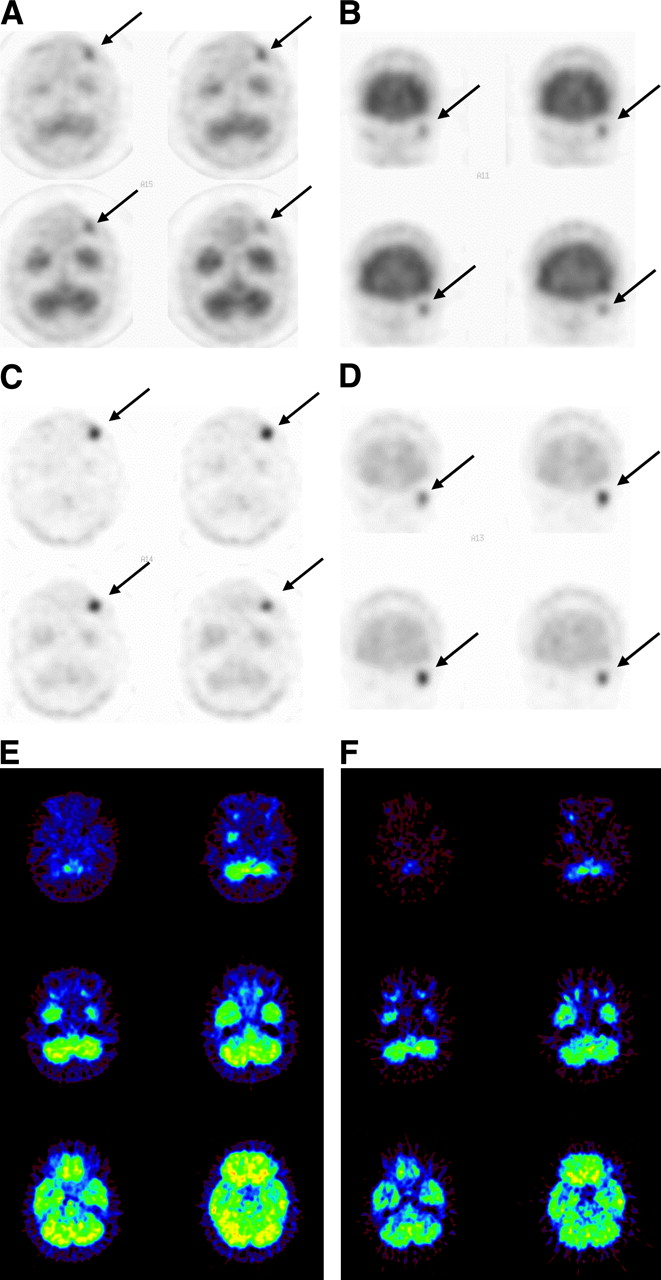
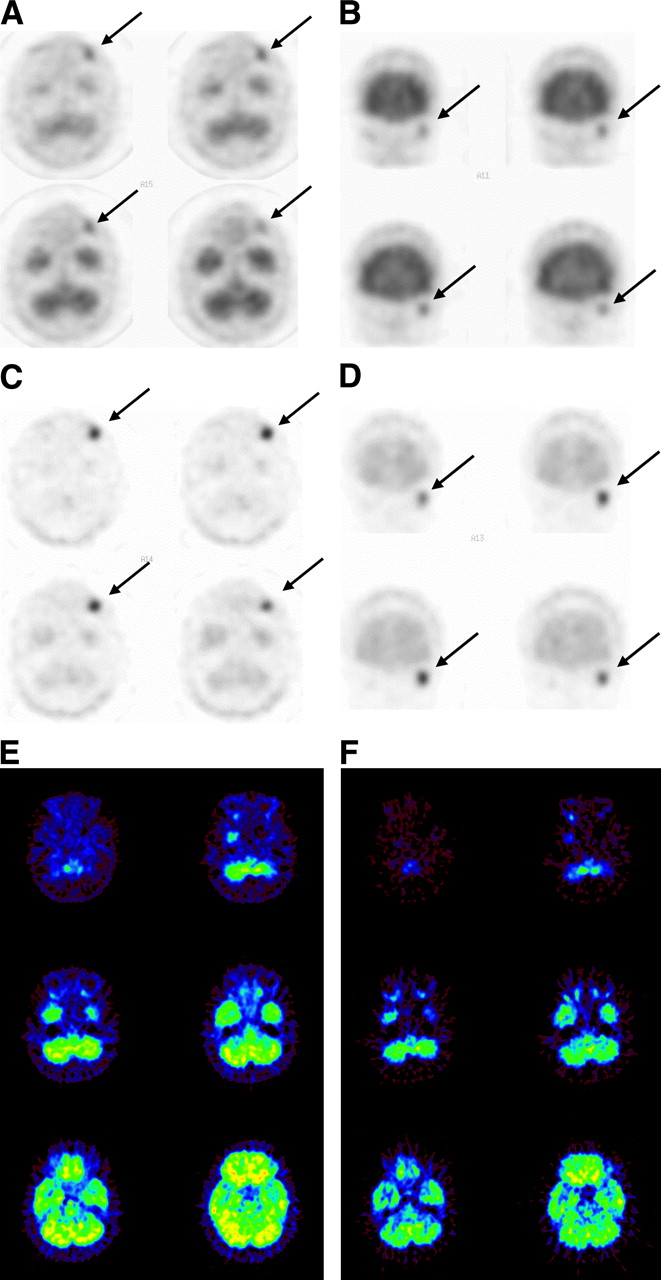
Images of uveal malignant melanoma in patient 1 (60-y-old woman). Three-hour images by 123I-IMP SPECT (axial images (A), coronal images (B)) show no positive area. 123I-IMP SPECT images (axial images (C), coronal images (D)) obtained 24 h after injection show positive area in site corresponding to left ocular tumor. (E) MR images show high-intensity area on T1-weighted images (left) and low-intensity area on T2-weighted images (right) in left eye. Arrows indicate uveal malignant melanoma.
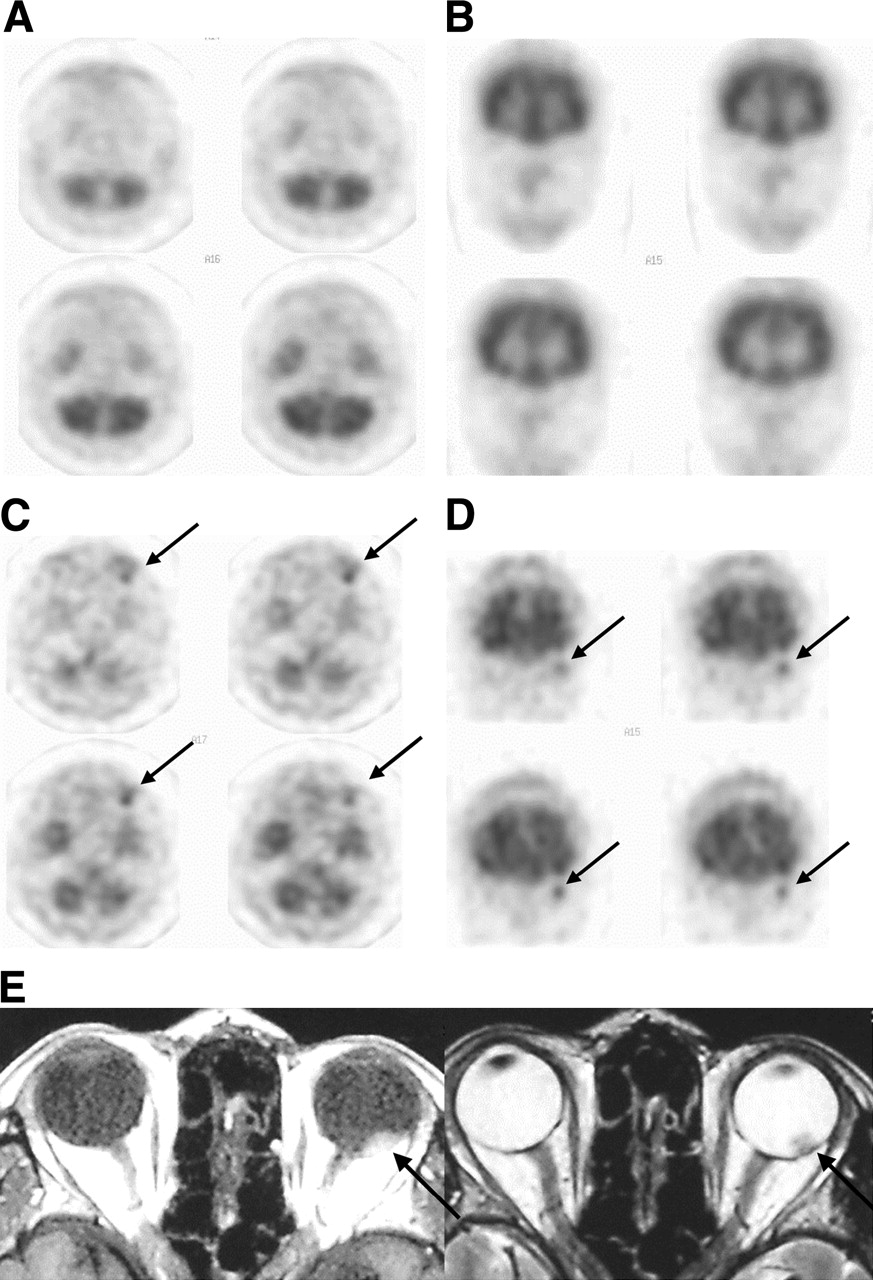
Images of uveal malignant melanoma in patient 13 (62-y-old woman). Three-hour images by 123I-IMP SPECT (axial images (A), coronal images (B)) show positive area in site corresponding to left eye tumor. 123I-IMP SPECT images (axial images (C), coronal images (D)) obtained 24 h after injection show positive area in site corresponding to left eye tumor. Arrows indicate uveal malignant melanoma. (E) 18F-FDG PET images show no positive area (images obtained by scan started 40 min after injection of 18F-FDG). (F) 18F-FDG PET images show no positive area (images obtained by scan started 3 h after injection of 18F-FDG).
The 18F-FDG PET–positive patient (patient 10) was also positive on 123I-IMP SPECT. The tumor size of uveal malignant melanoma in the 18F-FDG PET–positive patient was the largest, with a short diameter of 12 mm, a long diameter of 17 mm, and a height of 7 mm in all 12 patients with uveal malignant melanoma examined in this study. The tumor mass in the other 8 patients who were 123I-IMP SPECT positive and 18F-FDG PET negative had a dimension of 11 × 13 × 7 mm (short diameter × long diameter × height) or less. Except for the tumor mass, no particular clinical and histopathologic characteristics were detected in this 18F-FDG PET–positive patient.
DISCUSSION
Since the late 1980s, 123I-IMP scintigraphy has been reported to provide specific localization of uveal malignant melanoma by using planar imaging (15) or SPECT (16,18). The present study showed that 123I-IMP SPECT was useful for the diagnosis of uveal malignant melanoma. This result agrees well with that of the earlier studies (16,18). Furthermore, the present study revealed that, when examined by 18F-FDG PET, only 1 of 9 cases of uveal malignant melanoma was detected and that the other 8 cases were false-negative. From these results, it was concluded that the sensitivity of 18F-FDG PET for the diagnosis of uveal malignant melanoma is low.
Here, only 2 of the 12 123I-IMP-SPECT–positive patients showed an increased uptake of 123I-IMP at 3 h after intravenous administration of 123I-IMP. Therefore, the accumulation of 123I-IMP in the uveal malignant melanoma tissue must be judged by the late images obtained at 24 h after intravenous administration of 123I-IMP instead of the early images obtained at 3 h.
Since the mid-1990s, several clinical assessments have shown that 18F-FDG PET is a sensitive and accurate modality to detect metastases of cutaneous malignant melanoma within lymph nodes and viscera, with the exception of metastases in the brain (22–28,30). PET has been shown to be particularly effective to detect regional lymph node metastases of cutaneous malignant melanoma, and the smallest nodules detected were 4–5 mm in diameter (26). Besides the brain, 18F-FDG PET was also found to be inferior to CT for diagnosing lung and liver metastases of cutaneous malignant melanoma (31,32). Moreover, Lucignani et al. (19) and Modorati et al. (20) demonstrated that only some (3/12 (19) and 7/20 (20)) of uveal malignant melanomas were visualized by 18F-FDG PET; it was reported that, by 18F-FDG PET, the tumors with a diameter of <7.5 mm were not detected and only 7 of the 12 tumors with a diameter of >7.5 mm were detected and that the 18F-FDG PET uptake was not related to the pathologic features examined (20). Spraul et al. (21) evaluated 18F-FDG PET in the diagnosis of 9 patients with the malignant ocular tumors, consisting of the metastatic lesions from carcinoma of the stomach, breast, or lung (4 patients), malignant melanoma of the choroid (3 patients), malignant melanoma of the ciliary body (1 patient), and squamous cell carcinoma (1 patient), and found that 2 of the 3 cases of malignant melanoma of the choroid were negative and the other 7 cases were positive; they concluded that 18F-FDG PET is not sensitive enough for the diagnosis of malignant melanoma of the choroid (21). The result of the study of Spraul et al. on uveal malignant melanoma, in which 2 of the considered 4 cases were positive, seems to be similar to the results of the studies of Lucignani et al. and Modarati et al. in that ≥50% of the patients with uveal malignant melanoma showed false-negative results on 18F-FDG PET. The smallest tumor size that was detected by 18F-FDG PET in the study of Spraul et al. was a metastatic lesion from carcinoma of the lung with a diameter of 5 mm and a height of 2 mm (21). This value was very similar to the smallest lymph nodes with metastases of cutaneous malignant melanoma detected by PET (4–5 mm in diameter) (26). In the 2 cases of uveal malignant melanoma that were not detected in their study, the tumors had a dimension (diameter × height) of 7.5 × 3.3 mm and 9 × 6.7 mm; these sizes were larger than the limit of the method used (21). Therefore, it was suggested that factors other than the tumor size might contribute to the false-negative results in 18F-FDG PET of uveal malignant melanoma (21).
In the present study, only 1 of 9 patients with uveal malignant melanoma was detected by 18F-FDG PET. The sensitivity of PET in detecting this disease was worse than that reported by the earlier studies (19–21). Thus, the present study supports the earlier conclusion that 18F-FDG PET is not sensitive enough for the diagnosis of uveal malignant melanoma because a high incidence of false-negative results (19–21).
The smallest dimension of uveal malignant melanoma detected by 123I-IMP SPECT was 4 × 4 × 4 mm in the present study (patient 3 in Table 2). This value is very similar to that reported in an earlier study (16) and seems to not differ significantly from the value that was reported to be the smallest tumor size detected by 18F-FDG PET (a metastatic lesion from carcinoma of the lung) by Spraul et al. (21). These findings also support the suggestion that factors other than the tumor size would be involved in the high incidence of false-negative results on 18F-FDG PET of uveal malignant melanoma (21). Because hypoxia was shown to increase cellular uptake of 18F-FDG in malignant cell lines (33), Modorati et al. (20) hypothesized that 18F-FDG uptake by uveal malignant melanoma may be related to the hypoxic cell function of the tumor. Hypoxia may stimulate angiogenesis and tumor cell proliferation. In this study, there were no significant differences in the histopathologic finding of uveal malignant melanoma between the 18F-FDG PET–positive patient and the negative patients. Therefore, at present, we have no evidence that 18F-FDG uptake may be related to the state of hypoxia of uveal malignant melanoma.
In the present study, the tumor size of uveal malignant melanoma in the 18F-FDG PET–positive patient was the largest. Furthermore, with regard to the cases of malignant melanoma of the choroid in the study of Spraul et al. (21), the tumor size in the 18F-FDG PET–positive patient was the largest in all 3 cases. These results suggest that, in the patient with uveal malignant melanoma, a tumor size larger than a certain limit may be necessary together with the other factors to be detected by 18F-FDG PET.
There may be a question of whether the conditions of PET used in our study appear technically suboptimal for obtaining 18F-FDG uptake in uveal malignant melanoma. However, under the same conditions of PET as those used in the present study, we could detect primary and metastatic lesions of cutaneous malignant melanoma as sensitively as that reported in the earlier studies (22–28,30–32) (Katsuhiko Kato et al., 2005, unpublished data). In the study of Spraul et al. on the malignant ocular tumors, all 5 cases other than malignant melanoma (4 metastatic lesions from carcinoma of stomach, breast, or lung and 1 squamous cell carcinoma of orbit) were positive on 18F-FDG PET. Thus, the anatomic position might not be involved in the lower reactivity of uveal malignant melanoma to 18F-FDG PET in comparison with cutaneous malignant melanoma. At the present stage of our studies, we do not have any clues to factors other than the tumor size related to the low sensitivity of 18F-FDG PET in detecting uveal malignant melanoma.
CONCLUSION
From the results of the present study, we conclude that 123I-IMP SPECT is a sensitive and accurate method for detection of uveal malignant melanoma, whereas the efficacy of 18F-FDG PET for this purpose is low because of a high incidence of false-negative results. Therefore, 123I-IMP SPECT is more superior in comparison with 18F-FDG PET in detection of uveal malignant melanoma.
References
- Received for publication September 29, 2005.
- Accepted for publication December 1, 2005.





{kind=link}
{kind=link}