


Abstract
Because tumor targeting with radiolabeled monoclonal antibodies is more efficient in small lesions, radioimmunotherapy is considered most suitable for minimal or microscopic residual disease. The aim of the present studies was to assess the efficacy of adjuvant radiommunotherapy using radiolabeled monoclonal antibodies after cytoreductive surgery in rats with peritoneal carcinomatosis of colonic origin. Methods: We used a tumor model, in which peritoneal carcinomatosis was induced by intraperitoneal inoculation of CC-531 colon carcinoma cells in Wag/Rij rats. The biodistribution of the 125I-/111In-labeled anti-CC-531 MG1 monoclonal antibody after intraperitoneal administration was assessed. Subsequently, the efficacy of 177Lu-MG1 (74 MBq per rat) was compared with that of unlabeled MG1 or phosphate-buffered saline–bovine serum albumin in this model. Finally, rats with resectable intraperitoneal CC-531 tumors were subjected to exploratory laparotomy only, cytoreductive surgery only, exploratory laparotomy + radiommunotherapy (56 MBq 177Lu-MG1 per rat), or cytoreductive surgery + radiommunotherapy. Survival was the primary endpoint. Results: Both 125I- and 111In-labeled MG1 preferentially accumulated in intraperitoneal CC-531 tumors. The uptake of 111In-MG1 in tumor was higher than that of 125I-MG1 (4.1 ± 2.3 %ID/g vs. 1.1 ± 0.5 %ID/g [%ID/g is percentage of injected dose per gram], 72 h after injection; P = 0.053). Radiommunotherapy with 74 MBq 177Lu-MG1 almost completely eradicated tumor growth, whereas unlabeled MG1 had no effect. In the surgery study, both cytoreductive surgery and radiommunotherapy were well tolerated. The median survival of the control rats that underwent exploratory laparotomy only was 41 d. The median survival of the rats that were treated with cytoreductive surgery only, exploratory laparotomy + radiommunotherapy, or cytoreductive surgery + radiommunotherapy was 51 d (P = 0.05 compared with control rats), 61.5 d (P = 0.03), and 88 d (P = 0.0001), respectively, which suggests an additive effect of both treatment modalities. There was a highly significant trend toward improved survival of cytoreductive surgery + radiommunotherapy compared with both monotherapies (P = 0.0004). Conclusion: This study provides proof of principle that radiommunotherapy can be an effective treatment modality when applied as an adjuvant treatment after resection of tumors with a high risk of recurrence, such as after cytoreductive surgery of peritoneal carcinomatosis.
Over the past 2 decades, peritoneal carcinomatosis of colorectal origin has increasingly been recognized as a distinct clinical entity, which should not necessarily be regarded as generalized disease but—similar to liver metastases—may rather be one of the first steps of dissemination (1). For this reason, the efficacy of cytoreductive surgery and intraperitoneal chemotherapy, aimed at locoregional—that is, intraperitoneal—control, has been the subject of investigation in a dozen medical centers worldwide (2). The results published to date indicate that this aggressive approach indeed results in improved survival when compared with strictly palliative chemotherapy and surgery when needed in selected groups of patients (3,4). The completeness of resection as well as the tumor load were consistently shown to be the most important factors predictive of long-term survival. Still, after complete resection of all macrosopic disease and adjuvant intraperitoneal chemotherapy, the reported 5-y survival rate varies from 20% to 54% (3), with the majority of recurrences occurring intraperitoneally (5,6). More effective adjuvant treatment modalities are therefore necessary to improve the results of cytoreductive surgery.
Radioimmunotherapy using radiolabeled monoclonal antibodies (mAbs) directed against tumor-associated antigens offers the opportunity to selectively irradiate tumor cells, while sparing normal tissues. Because tumor targeting with radiolabeled mAbs is more efficient in small-volume disease, radioimmunotherapy is considered most suitable for minimal or microscopic residual disease (7). In this regard, the results of a recently published phase II trial, investigating the efficacy of adjuvant radioimmunotherapy using the 131I-labeled anticarcinoembryonic antigen mAb hMN-14 after salvage resection of liver metastases of colorectal origin, suggested that radioimmunotherapy may indeed improve both the overall median survival and the 5-y survival rate, compared with historical and contemporaneous controls (8).
The MG1 mAb, raised against the syngeneic rat colon carcinoma cell line CC-531, has been shown to localize to CC-531 tumors in Wag/Rij rats (9). We hypothesized that radioimmunotherapy using radiolabeled MG1 might be an effective adjuvant treatment modality after cytoreductive surgery of peritoneal carcinomatosis. To test this hypothesis, first the biodistribution of MG1 labeled with 125I or 111In was determined in Wag/Rij rats with small-volume peritoneal CC-531 carcinomatosis. Subsequently, the efficacy of radioimmunotherapy using 177Lu-labeled MG1 was ascertained. Finally, the efficacy of cytoreductive surgery followed by adjuvant radioimmunotherapy using 177Lu-labeled MG1 was assessed and compared with that of exploratory laparotomy followed by radioimmunotherapy, cytoreductive surgery only, or exploratory laparotomy only.
MATERIALS AND METHODS
Animals
Male Wag/Rij-rats, 10- to 12-wk old with a mean weight of 245 ± 8 g, were obtained from Charles River Laboratories. Rats were acclimated to laboratory conditions for 1 wk before experimental use and housed on sawdust in filter-topped cages (2 rats per cage) with free access to animal chow (Snif Voer) and water. All experiments were approved by the institutional Animal Welfare Committee of the Radboud University Nijmegen.
Cell Line
The syngeneic rat colon carcinoma cell line CC-531, derived from colon tumors of Wag/Rij rats exposed to 1,2-dimethyl-hydrazine, was used (10). CC-531 was cultured and maintained as monolayers on plastic in Dulbecco's modified Eagle medium (DMEM; GIBCO, BRL Life Sciences Technologies) supplemented with 10% fetal calf serum (GIBCO), 2 mmol/L l-glutamine, penicillin (100 units/mL), and streptomycin (100 μg/mL) at 37°C in a humidified atmosphere with 5% CO2. Before inoculation, tumor cells were washed with phosphate-buffered saline (PBS), harvested with 0.25% trypsin (3 min at 37°C), resuspended in PBS, spun down (5 min at 700g), counted, and resuspended once again in PBS to the appropriate concentration.
mAb
The MG1 mAb was purchased from Antibodies for Research Applications BV (www.abforresearch.nL). The MG1 mAb is a murine IgG2a antibody, raised by immunization of mice with CC-531 colon carcinoma cells (9,11). It recognizes an 80-kDa cell-surface antigen and localizes to tumor cells when injected in rats bearing CC-531 tumors with minimal cross-reactivity to other cell types.
Radiolabeling and Quality Control
Antibodies were radioiodinated with 125I (Amersham) using the IODO-GEN (Pierce Chemicals) method, as described (12). Labeling efficiency of the radioiodination reaction was 42%. The specific activity of 125I-MG1 was 85 kBq/μg.
Labeling of the MG1 mAb with 111In (Tyco Mallinckrodt Medical BV) or 177Lu (IDB Holland BV) was performed under strict metal-free conditions. To allow labeling of the antibodies with 111In or 177Lu, the MG1 mAb was conjugated with isothiocyanatobenzyl-diethylenetriaminepentaacetic acid (ITC-DTPA; Macrocyclics), as described (13). The DTPA-MG1 conjugate (DTPA/MG1 ratio, 1.6:1; 1.0 mg/mL) was incubated with 111In or 177Lu in 0.1 mol/L ammonium acetate buffer, pH 5.4, at room temperature (60 min). The specific activity of the 111In-DTPA-MG1 preparation (hereafter referred to as 111In-MG1) used in the biodistribution study was 1.1 MBq/μg. The specific activities of the 177Lu-DTPA-MG1 preparations (hereafter referred to as 177Lu-MG1) used in the radioimmunotherapy monotherapy study and the cytoreductive surgery + radioimmunotherapy study were 0.81 MBq/μg and 0.89 MBq/μg, respectively. The labeling efficiency of both labeling procedures exceeded 98%. Because nonchelated 177Lu might incorporate into the mineral bone, after completion of the labeling procedure 1 mmol/L ethylenediaminetetraacetic acid (EDTA) was added to the injection solutions to scavenge the remaining free 177Lu ions (14).
All reaction mixtures were purified on a PD-10 column, eluted with PBS–0.5% bovine serum albumin (BSA). The radiochemical purity (RCP) was determined using instant thin-layer chromatography on Silicagel strips (Gelman Sciences) using 0.10 mol/L citrate buffer, pH 6.0, as the mobile phase. The RCP of the 125I-, 111In-, and 177Lu-MG1 preparation was 98%, 99%, and 99%, respectively. The immunoreactivity of the radiolabeled MG1 preparations was essentially determined as described by Lindmo et al. (15), with minor modifications as described (13). The immunoreactivity of each of the radiolabeled MG1 preparations was >65%. Radiolabeled antibody preparations were administered within 2 h after the labeling procedures.
Animal Model of Peritoneal Carcinomatosis
The animal model of peritoneal carcinomatosis using CC-531 has been described previously (16). Briefly, peritoneal carcinomatosis was induced by intraperitoneal inoculation of 2.0–5.0 × 106 CC-531 tumor cells suspended in 2 mL of PBS. In this model, the first macroscopic tumor deposits are seen 4–7 d after tumor cell inoculation. Three to 5 wk after tumor induction, bulky peritoneal carcinomatosis with hemorrhagic ascites is present.
Biodistribution of 125I-/111In-Labeled MG1
We previously demonstrated in a nude mouse model of peritoneal carcinomatosis of colonic origin that 131I and 177Lu are the most suitable radionuclides for radioimmunotherapy of small peritoneal metastases (13). To determine the most suitable radionuclide for radioimmunotherapy in the current model, the biodistribution of MG1 labeled with either 125I or 111In, as surrogate radionuclides for 131I and 177Lu, respectively, was determined. Eight days after intraperitoneal inoculation of 5.0 × 106 CC-531 tumor cells, 5 rats received an intraperitoneal injection of 370 kBq 125I-MG1 and 370 kBq 111In-MG1 (total MG1 protein dose, 5 μg per rat), solubilized in 1 mL PBS–0.5% BSA. Three days after injection of the radiolabeled antibodies, the rats were euthanized using O2/CO2 asphyxiation and dissected. At dissection, tumor, blood, bone marrow, liver, spleen, kidney, intestine, lung, muscle, skin, and thymus were sampled and immediately weighed. Activity was measured in a shielded well-type γ-counter (Wizard; Pharmacia-LKB). To correct for physical decay and to calculate uptake of the radiolabeled antibody in each sample as a fraction of the injected dose, aliquots of the injected dose were counted simultaneously. The results are expressed as the percentage of the injected dose per gram tissue (%ID/g).
Efficacy of Radioimmunotherapy Using 177Lu-MG1
Before investigating the efficacy of adjuvant radioimmunotherapy after cytoreductive surgery, first the efficacy of radioimmunotherapy given as monotherapy was assessed. Four days after intraperitoneal inoculation of 2.0 × 106 CC-531 tumor cells, rats were randomly assigned to be treated with 177Lu-MG1 (74 MBq, 91 μg per rat), unlabeled MG1 (91 μg), or the carrier (PBS–0.5% BSA) (8–10 rats per group). We previously demonstrated that the maximal tolerated activity dose (MTD) of 177Lu-labeled mAbs in 20- to 25-g nude mice is 16.7 MBq (13). Radioimmunotherapy at 74 MBq 177Lu-MG1 was therefore considered safe in Wag/Rij rats. In addition, an extra group of 5 rats received tracer doses of 177Lu-MG1 (3.7 MBq, 91 μg per rat) to determine the biodistribution at 72 h after injection. Because 177Lu is a bone-seeking radionuclide, uptake in the femur was determined as well. Thirty days after tumor cell inoculation, rats were euthanized and dissected. At dissection, all tumor nodules were excised and weighed.
Effect of Cytoreductive Surgery With or Without Adjuvant Radioimmunotherapy
Fourteen days after intraperitoneal inoculation of 2.0 × 106 CC-531 tumor cells, 35 rats were randomly assigned to undergo cytoreductive surgery (n = 18) or exploratory laparotomy (n = 17). Subsequently, all rats underwent a midline laparotomy during which the intraperitoneal tumor load was semiquantitatively scored. After completion of the surgical procedures, those rats that had undergone cytoreductive surgery were distributed into 2 groups by an independent nuclear medicine physician after stratification for tumor load: completeness of resection and whether a splenectomy had been performed. Similarly, those rats that had undergone exploratory laparotomy only were divided into 2 groups after stratification for tumor load. Three days after surgery, 1 group of rats that had been treated with cytoreductive surgery and 1 group of rats that had undergone exploratory laparotomy received only an intraperitoneal injection of 56 MBq 177Lu-MG1 (total MG1 protein dose, 63 μg). The remaining rats received intraperitoneal injections of the carrier (PBS–0.5% BSA and 1 mmol/L EDTA). Thus, 4 treatment groups were created: (i) exploratory laparotomy only (n = 9); (ii) exploratory laparotomy + radioimmunotherapy (n = 8); (iii) cytoreductive surgery only (n = 9); (iv) cytoreductive surgery + radioimmunotherapy (n = 9).
Operative Procedures
The surgical procedures were performed under clean conditions. After the onset of general anesthesia (isoflurane/O2/N2O), rats underwent a 7.5-cm midline laparotomy from the xyphoid process to just above the penis. After opening the abdomen, the abdominal cavity was carefully inspected, including the parietal peritoneum at the site of tumor cell inoculation, the greater omentum, the liver hilum, the perisplenic region, the diaphragm, the gonadal fat pads, the kidneys, the mesentery, and Douglas' pouch. Tumor growth at each of these sites was scored 0 (no macroscopic tumor growth), 1 (little tumor growth), 2 (moderate tumor growth), or 3 (abundant tumor growth). The sum of the tumor scores at all sites represented the peritoneal cancer index (PCI).
In those rats assigned to undergo cytoreductive surgery, resection of all macroscopic tumor deposits was then attempted. In the case of disease that was not resectable, tumor nodules were cauterized using an electrocoagulation device. The resected tumor nodules, including the omentectomy specimens, were collected and weighed. When the surgical cytoreduction was considered maximal, the muscular layer of the abdomen was closed by continuous Vicryl 3/0 sutures (Ethicon). The skin was closed by iron wound autoclips.
Follow-up
The primary endpoint was survival. Body weight was measured daily in the first 14 d after treatment and 3 times weekly thereafter as a measure of toxicity. Rats were monitored daily until the humane endpoint had been reached, as determined by a single experienced animal technician, who was unaware of the therapeutic regimen. At the time of the humane endpoint, rats were usually lethargic, showing signs of advanced peritoneal carcinomatosis, such as the presence of ascites or bulky intraperitoneal tumor growth. When the humane endpoint had been reached, rats were euthanized by O2/CO2 asphyxiation and immediately dissected. At dissection, intraperitoneal tumor growth was semiquantitatively scored as described. After calculating a PCI, all macroscopic tumor deposits were excised and weighed. The experiment was terminated at 118 d after tumor cell inoculation, when the remaining rats were euthanized and dissected. In the case of absence of macroscopic tumor growth, relevant organs—including the greater omentum, the mesentery, and the diaphragm—were removed for routine histopathologic hemotoxylin and eosin staining or immunohistochemical staining using the murine MG1 antibody in combination with a horse antimouse IgG peroxidase antibody conjugate (Vector Laboratories Inc.).
Statistical Analysis
Single comparisons were analyzed using the paired t test or the nonparametric Mann–Whitney U test. Multiple comparisons were analyzed using 1-way ANOVA. Bonferroni correction for multiple testing was applied. Survival curves were compared using the log-rank test. All tests were 2-sided; the level of statistical significance was set at P < 0.05.
RESULTS
Biodistribution of 125I-/111In-Labeled MG1
The biodistribution results are summarized in Figure 1. There was preferential uptake of both radiolabeled antibody preparations in the tumor, although uptake of 125I-MG1 in tumor tissue was not significantly higher than the corresponding blood levels (P = 0.093). Uptake of 111In-MG1 in tumor tissue was higher than that of 125I-MG1, although the difference was not statistically significant (4.1 ± 2.3 %ID/g vs. 1.1 ± 0.5 %ID/g; P = 0.053). Ratios of tumor to blood and tumor to bone marrow for 111In-MG1 were significantly higher than those obtained for 125I-MG1 (9.2 ± 5.3 vs. 2.4 ± 1.4 [P = 0.040] and 19.5 ± 8.4 vs. 7.6 ± 4.1 [P = 0.036], respectively). Likewise, uptake of 111In-MG1 in the spleen and liver was higher than that of 125I-MG1, although the difference for the latter organ did not reach statistical significance. On the basis of the favorable biodistribution of 111In-MG1, it was decided to use 177Lu in the radioimmunotherapy studies.
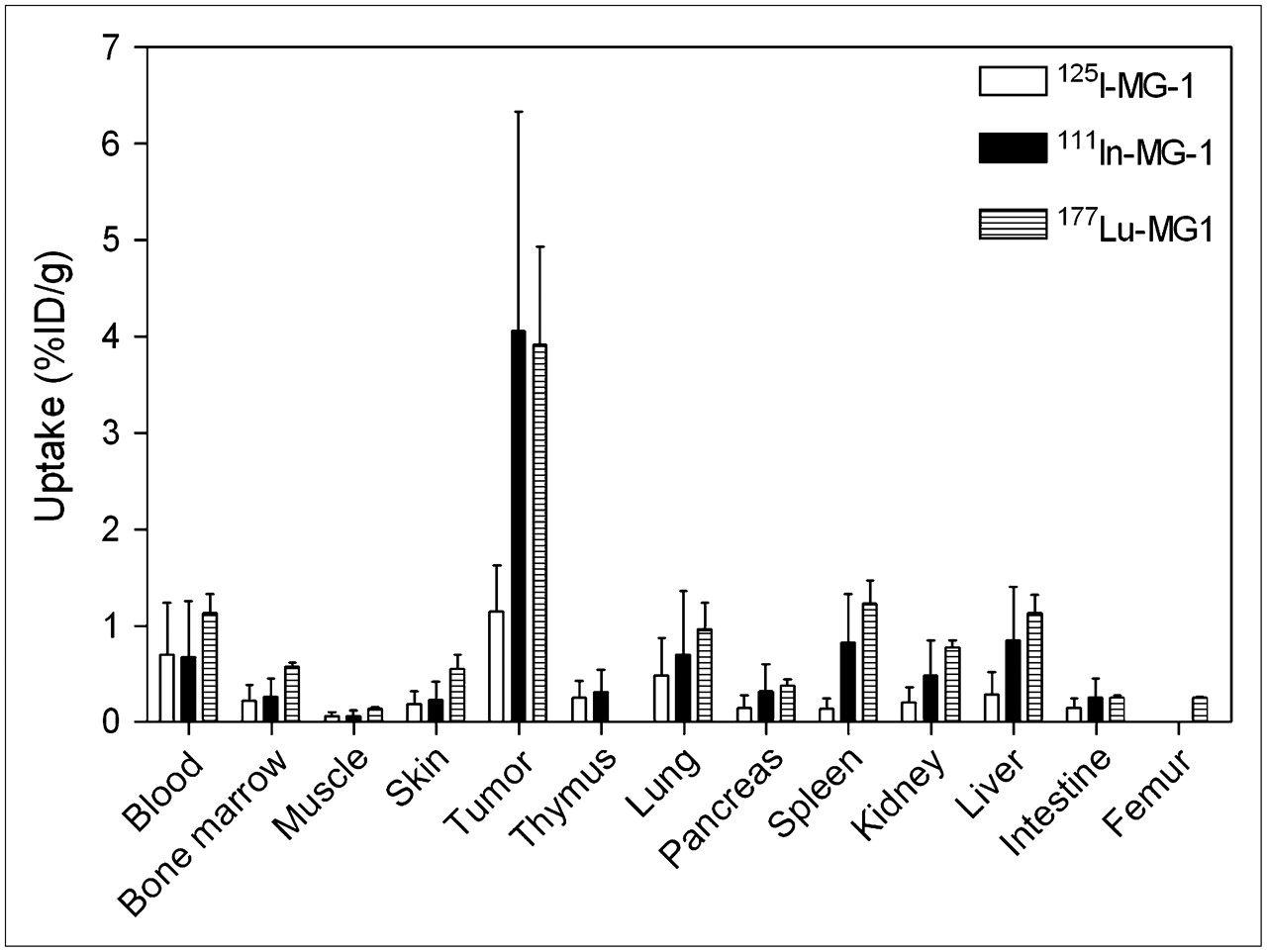
Biodistribution of 125I-MG1, 111In-MG1, or 177Lu-MG1 in Wag/Rij rats with small peritoneal CC-531 metastases. Note that biodistribution of 177Lu-MG1 was determined in a separate experiment.
Efficacy of Radioimmunotherapy Using 177Lu-MG1
The mean body weight of the control rats as well as that of the rats treated with DTPA-MG1 gradually increased during the course of the study. However, the mean body weight of the rats treated with 74 MBq 177Lu-MG1 decreased to a maximum mean body weight loss of 2.6% ± 3.2% on days 5 and 6 after intraperitoneal administration, after which all rats regained body weight again (data not shown).
The biodistribution of 177Lu-MG1 at 72 h after injection was similar to that of 111In-MG1 (Fig. 1). The mean uptake in tumor tissue was 3.9 ± 1.0 %ID/g, whereas the ratios of tumor to blood and tumor to bone marrow were 3.5 ± 0.2 and 7.0 ± 1.2, respectively. Uptake in femur was only 0.25 ± 0.02 %ID/g.
The rats were euthanized 30 d after intraperitoneal tumor cell inoculation. On dissection, the majority of the rats that had received PBS–0.5% BSA and 1 mmol/L EDTA (control rats) or unlabeled DTPA-MG1 had abundant intraperitoneal tumor growth with hemorrhagic ascites. In contrast, the rats that had been treated with 74 MBq 177Lu-MG1 had very little tumor growth. The mean tumor weight of the control rats and of the rats treated with unlabeled ITC-DTPA-MG1 was practically identical, 5.8 ± 3.0 and 5.9 ± 4.3 g, respectively. In contrast, the mean tumor weight of the rats that had been treated with radioimmunotherapy was 0.00 ± 0.00 g (P < 0.01 comparing radioimmunotherapy with PBS–0.5% BSA or unlabeled MG1; Fig. 2).

Tumor weight at dissection of Wag/Rij rats with small peritoneal CC-531 metastases 26 d after treatment with PBS–0.5% BSA (control rats), unlabeled MG1, or 177Lu-MG1. Note that these rats did not undergo surgery.
Effect of Cytoreductive Surgery With or Without Adjuvant Radioimmunotherapy
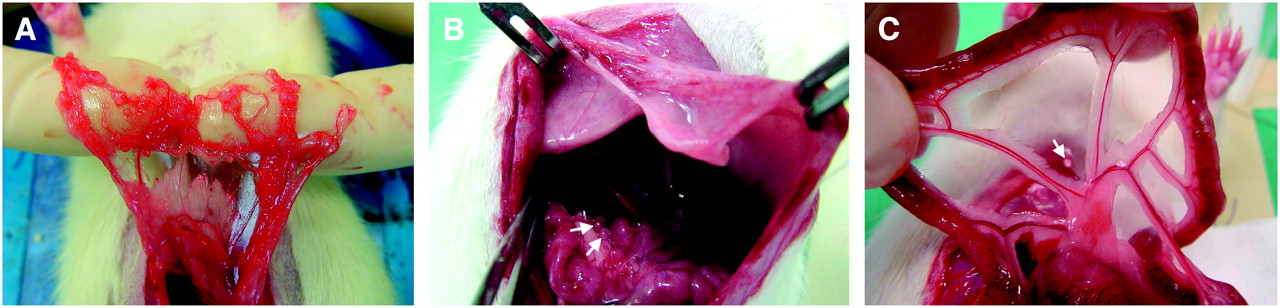
The greater omentum was the most common site of tumor growth (all rats), followed by the liver hilum (34/35 rats), the mesentery (30/35 rats), and the perisplenic region (25/35 rats). The diameter of the tumor nodules was always <5 mm and ranged from 1 to 4 mm. None of the rats had malignant ascites. The median PCI of all rats was 7 (range, 3–10). Three representative examples of macroscopic tumor growth at the greater omentum, the liver hilum, and the mesentery are depicted in Figure 3.
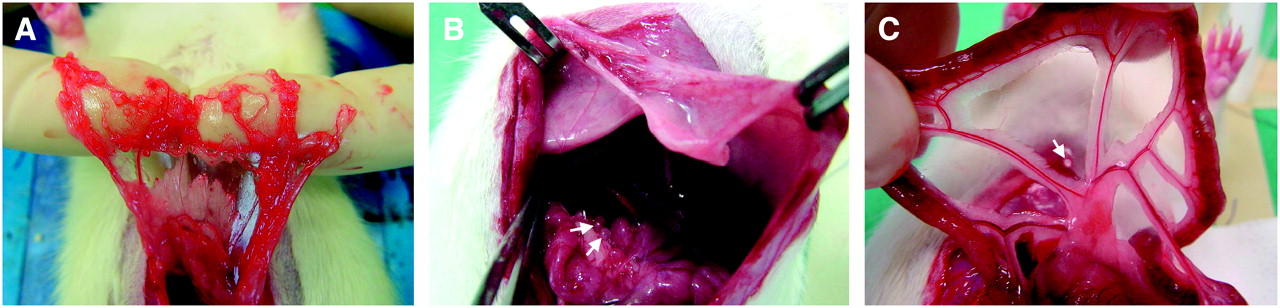
Macroscopic appearance of intraperitoneally growing CC-531 tumors in Wag/Rij rats. (A) Multiple tumor deposits in greater omentum. (B) Two tumor deposits in liver hilum (arrows). (C) One tumor deposit on mesentery (arrow).
An omentectomy was routinely performed in the 18 rats that underwent cytoreductive surgery. Perisplenic tumor growth necessitated splenectomy in 9 of 18 rats that underwent cytoreductive surgery. In 15 of 18 rats undergoing cytoreductive surgery, the resection of all tumor nodules seemed macroscopically complete, whereas in 3 rats macroscopic disease remained in situ. In those 3 rats that had undergone an incomplete cytoreduction, the size of the residual disease was always <1 mm.
The 4 treatment groups were well balanced with regard to the stratification factors mentioned earlier, as well as the body weight, the number of tumor nodules per site (data not shown), and, when applicable, the weight of the resection specimens (Table 1).
Rat, Surgical, and Pathologic Characteristics
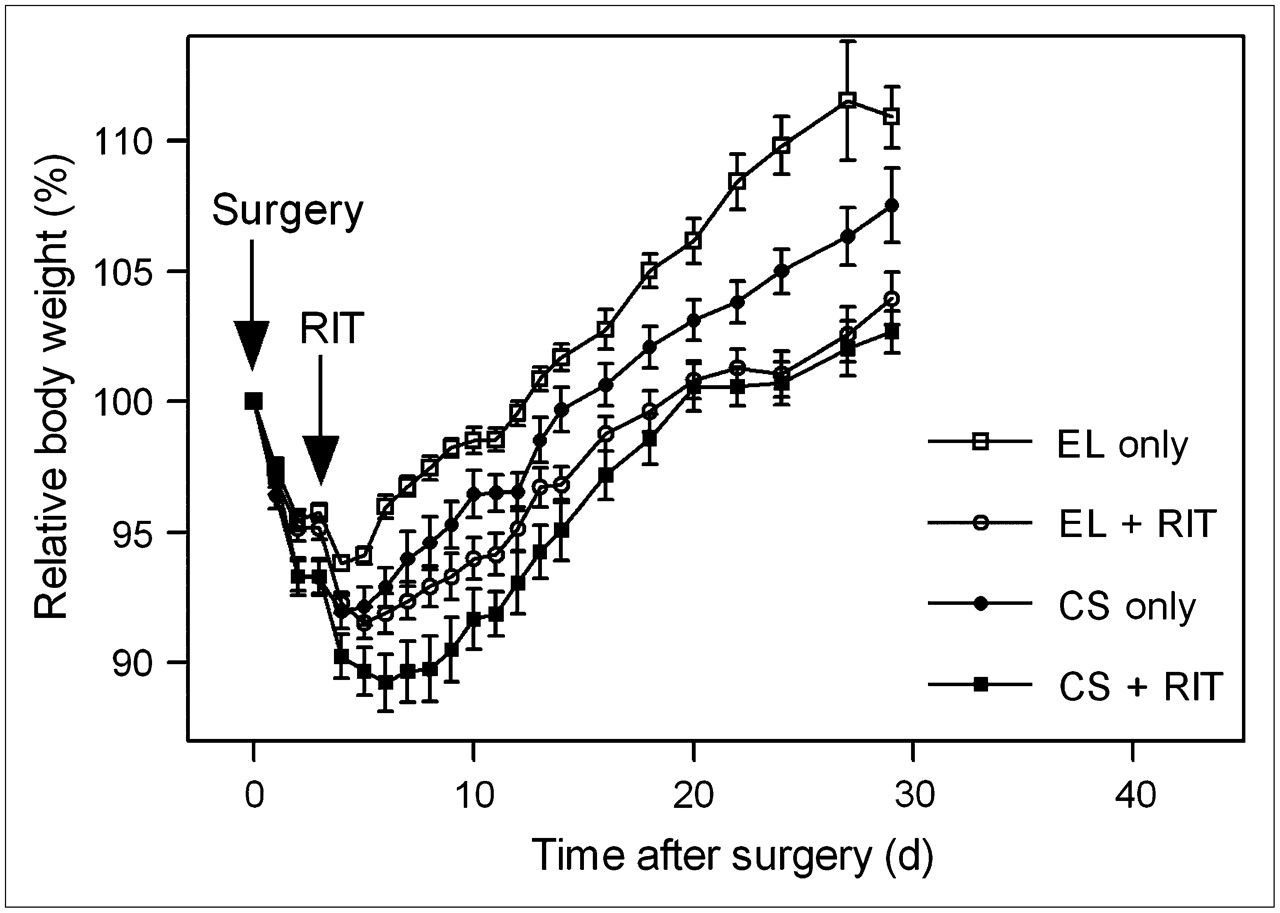
The relative body weight, expressed as the percentage of the body weight on the day of surgery, is depicted in Figure 4. On the third postoperative day, before the administration of radioimmunotherapy, those rats that were treated with cytoreductive surgery had lost more body weight than those that underwent exploratory laparotomy (6.7% ± 1.9% vs. 4.5% ± 1.1%; P = 0.0002). The maximum mean body weight loss of the rats of the exploratory laparotomy–only group was 6.4% ± 0.6% 4 d after the surgery. The maximum body weight loss of the rats of the exploratory laparotomy + radioimmunotherapy group was 8.5% ± 1.7% 5 d after surgery or 2 d after start of the radioimmunotherapy (P = 0.001 compared with the maximum weight loss of the rats of the exploratory laparotomy–only group). The maximum body weight loss of the rats of the cytoreductive surgery–only group was 8.1% ± 1.9% 4 d after surgery (P = 0.015). The maximum mean body weight loss of the rats of the cytoreductive surgery + radioimmunotherapy group was 10.7% ± 3.3% 6 d after surgery or 3 d after start of the radioimmunotherapy (P = 0.0003). After reaching their nadirs, rats regained body weight again at approximately the same rate.
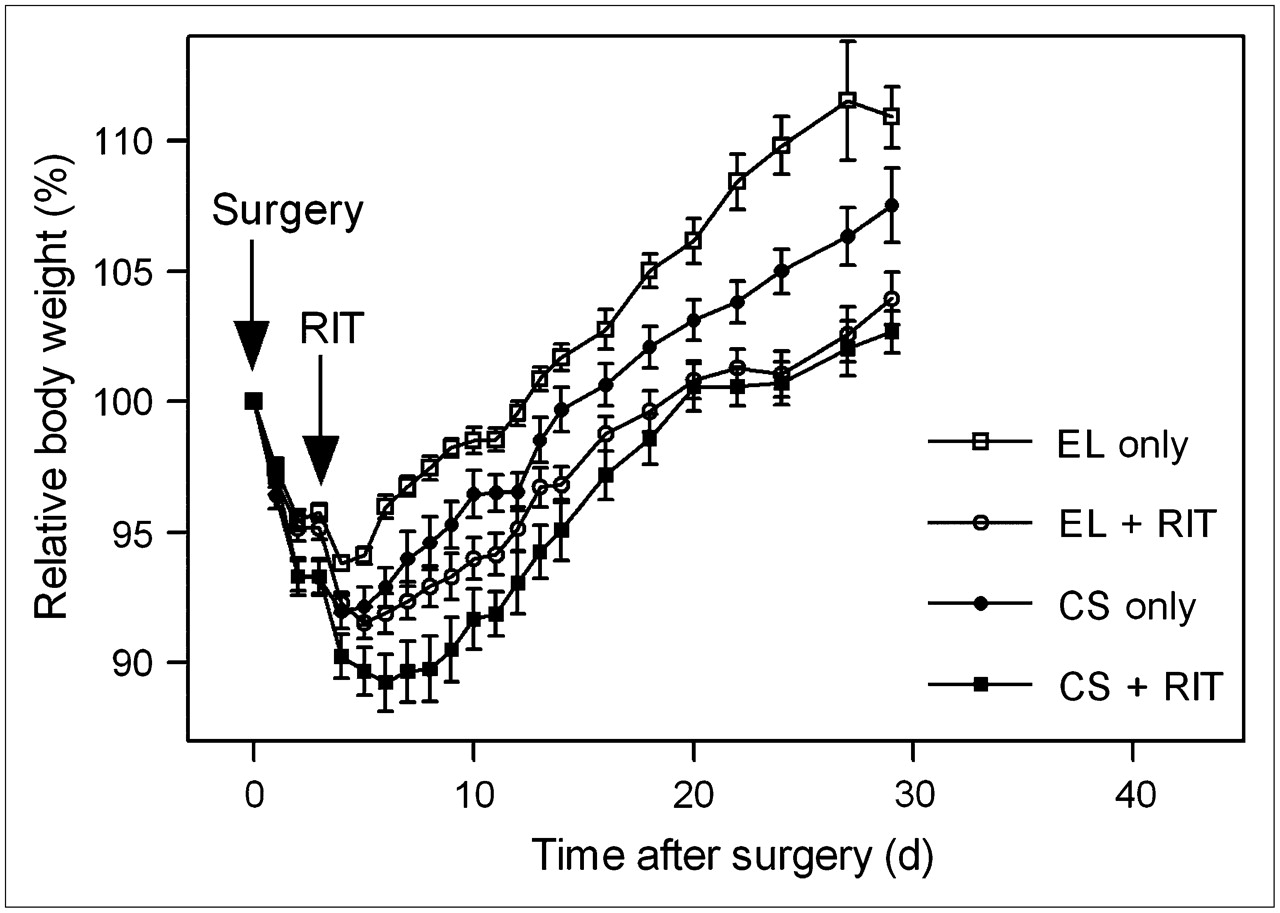
Relative body weight of Wag/Rij rats with small peritoneal CC-531 metastases in first month after exploratory laparotomy (EL) only, EL + radioimmunotherapy (RIT), cytoreductive surgery (CS) only, or CS + RIT. Data are expressed as mean ± SEM.
Thirty-two rats died due to intraperitoneal tumor growth. The survival curves of the various treatment groups are shown in Figure 5. The median survival of the control rats that underwent exploratory laparotomy only was 41 d (range, 37–82 d). The median survival of the rats that had undergone cytoreductive surgery only was 51 d (range, 45–118 d) (P = 0.0544 when compared with the control rats). The median survival of the rats that were treated with exploratory laparotomy followed by intraperitoneal radioimmunotherapy was 61.5 d (range, 47–118 d) (P = 0.0304 when compared with the control rats; P = 0.47 when compared with the cytoreductive surgery–only group). Cytoreductive surgery + radioimmunotherapy resulted in the highest median survival of 88 d (range, 68–118 d) (P = 0.0001 when compared with the control rats; P = 0.0503 when compared with the cytoreductive surgery–only group; P = 0.0822 when compared with the exploratory laparotomy + radioimmunotherapy group). There was a highly significant trend toward improved survival in the cytoreductive surgery + radioimmunotherapy group, both when compared with the cytoreductive surgery–only group as well as with the exploratory laparotomy + radioimmunotherapy group (P = 0.0004 for both trend analyses).
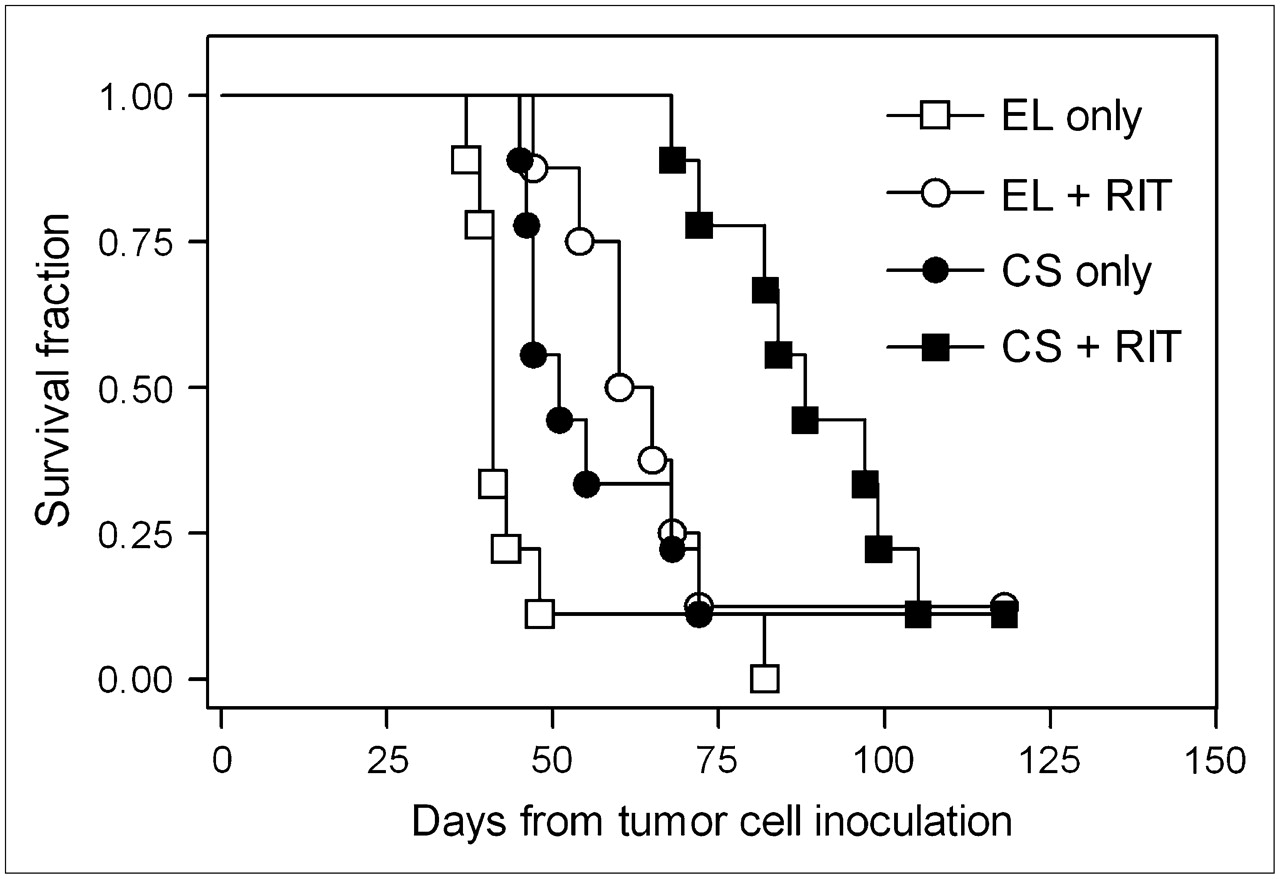
Survival curves for Wag/Rij rats with small peritoneal CC-531 metastases after exploratory laparotomy (EL) only, EL + radioimmunotherapy (RIT), cytoreductive surgery (CS) only, or CS + RIT. There was a highly significant trend toward improved survival for rats treated with CS + RIT compared with both CS only and EL + RIT (P = 0.0004 for both trend analyses).
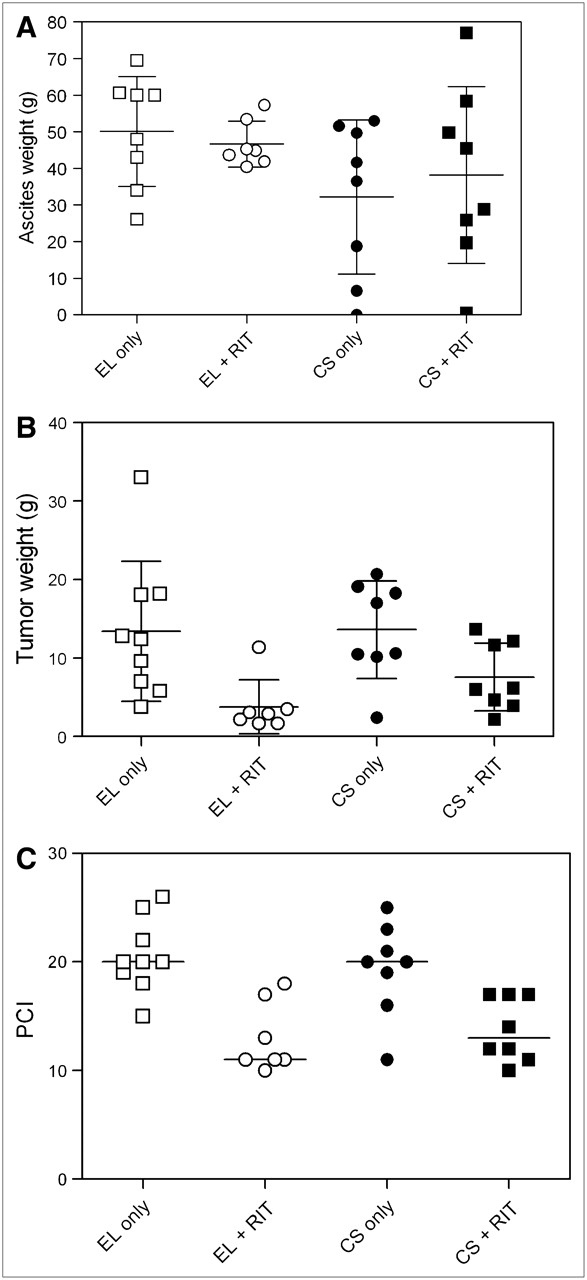
Formation of hemorrhagic ascites was the most common cause of death. Of the 32 rats that died because of intraperitoneal tumor growth, 31 had hemorrhagic ascites. The ascites weight, tumor weight, and PCI found on dissection are depicted in Figures 6A, 6B, and 6C, respectively. The mean ascites weight varied from 32.2 ± 21.0 g in the rats that had undergone cytoreductive surgery only to 50.2 ± 15.0 g in the control group (P = 0.22). The mean tumor weight found on dissection at the time the rats reached their humane endpoints varied from 3.8 ± 3.4 g in the exploratory laparotomy + radioimmunotherapy group to 13.6 ± 6.2 g in the cytoreductive surgery–only group (P = 0.011). The median PCI varied from 11 (range, 10–18) in the exploratory laparotomy + radioimmunotherapy group to 20 (range, 18–26) in the cytoreductive surgery–only group (P = 0.0002). Multiple comparison analyses indicated that the median PCI of the exploratory laparotomy + radioimmunotherapy and cytoreductive surgery + radioimmunotherapy groups was significantly lower when compared with the exploratory laparotomy–only and the cytoreductive surgery–only groups. There was a highly significant correlation between the PCI and the weight of the dissected tumor deposits (Spearman r = 0.8283; P < 0.0001). However, there was no correlation between ascites weight and PCI (Spearman r = 0.1948; P = 0.2670) or tumor weight (Spearman r = −0.0629; P = 0.7239).

(A) Ascites weight found in Wag/Rij rats with small peritoneal CC-531 metastases at time of death after exploratory laparotomy (EL) only, EL + radioimmunotherapy (RIT), cytoreductive surgery (CS) only, or CS + RIT. Differences were not statistically significant (P = 0.2219). (B) Tumor weight found in Wag/Rij rats with small peritoneal CC-531 metastases at time of death after EL only, EL + RIT, CS only, or CS + RIT. Tumor weight of rats treated with EL + RIT was significantly lower compared with that of rats treated with EL only or CS only (P < 0.05). (C) PCI found in Wag/Rij rats with small peritoneal CC-531 metastases at time of death after EL only, EL + RIT, CS only, or CS + RIT. PCI of rats treated with RIT, preceded by either EL or CS, was significantly lower compared with that of rats treated with EL only or CS only (P < 0.05).
At the end of the experiment (118 d after tumor cell inoculation), there were 3 rats (1 treated with exploratory laparotomy + radioimmunotherapy, 1 treated with cytoreductive surgery only, and 1 treated with cytoreductive surgery + radioimmunotherapy) without signs of intraperitoneal tumor growth. On dissection, there was no evidence of disease in any of these rats. Histopathologic examination of relevant organs—including the diaphragm, the mesentery, and, when available, the greater omentum—did not reveal microscopic residual disease in any of these rats.
DISCUSSION
The primary aim of the present experimental studies was to investigate the therapeutic efficacy of radioimmunotherapy when administered postoperatively as an adjuvant treatment after surgical cytoreduction of peritoneal carcinomatosis of colonic origin. Whereas the median survival after cytoreductive surgery only and exploratory laparotomy + radioimmunotherapy was only 10 d (P = 0.05) and 21.5 d (P = 0.03) longer than that of the control rats that had undergone exploratory laparotomy only, the combination of cytoreductive surgery and radioimmunotherapy resulted in an improvement of 43 d (P = 0.0001), which suggests an additive effect of the 2 treatment modalities.
The syngeneic rat colon carcinoma cell line CC-531 was used because of its reproducible in vivo growth pattern in Wag/Rij rats. Hagenaars et al. studied the tumor-targeting potential of the MG1 mAb after intraperitoneal administration in Wag/Rij rats with CC-531 liver metastases and found that the antibody selectively localized to the CC-531 tumors, with some cross-reactivity to thymus, lymph node, salivary glands, and skin (9). However, no data were provided on the absolute or percentage uptake in tumor tissue of MG1. Therefore, before initiating radioimmunotherapy studies, the biodistribution of the MG1 mAb labeled with 125I or 111In—as surrogate radionuclides for 131I and 177Lu, respectively—was studied. Both 125I-MG1 and 111In-MG1 preferentially accumulated in the intraperitoneal CC-531 tumors. The uptake of 111In-MG1 in tumor tissue, however, was higher, which probably is due to differences in cellular routing of the radiolabeled metabolites after intracellular catabolism of the antibodies (17). Therefore, the higher uptake of 111In-ITC-DTPA-MG1 favored the use of 177Lu instead of 131I in radioimmunotherapy studies. Furthermore, the medium-energy β-emission of 177Lu and its concomitant maximum penetration range of 2.5 mm in tissue, in combination with its physical half-life of 6.7 d, make 177Lu an attractive radionuclide for radioimmunotherapy of small-volume disease, as reported in preclinical and clinical studies (13,18).
MG1, as an IgG2a antibody, theoretically could have an antitumor effect itself through complement-mediated tumor cell lysis or complement- or antibody-dependent cellular cytotoxicity. In this regard, Gelderman et al. (19) studied the complement activation potential of the MG1-4 mAb family and found that MG1 did not activate the complement system in vitro. These findings corroborate with the results of the first therapy study reported in this article, in which unlabeled MG1 had no measurable antitumor effect in rats with CC-531 peritoneal metastases. Radioimmunotherapy using 177Lu-MG1 was given at an activity dose of 74 MBq per rat. As the MTD of 177Lu-labeled IgG in 25-g nude mice is 16.7 MBq (13), the MTD of 177Lu-MG1 in 250-g rats could theoretically be as high as 167 MBq. Indeed, radioimmunotherapy using 74 MBq 177Lu-MG1 resulted in minor toxicity, as evidenced by a maximum mean body weight loss of only 2.6% ± 3.2%, which suggests that a higher activity dose could be given safely. Still, radioimmunotherapy using 74 MBq 177Lu-MG1 almost completely ablated intraperitoneal tumor growth, when given as a single treatment in rats that did not undergo surgery.
In the therapy studies, cytoreductive surgery consisted of complete laparotomy and resection of all macroscopic disease, including formal omentectomy, as is practiced in patients undergoing cytoreductive surgery followed by intraperitoneal chemotherapy (4). The modest survival benefit (P = 0.0504) of the rats treated with cytoreductive surgery only may be explained partially by the omentectomy, which was routinely performed in all rats that underwent cytoreductive surgery. In various experimental models, it has been shown that tumor cells preferentially accumulate in the so-called “milky spots” of the omentum in the early stages of intraperitoneal dissemination (16,20). In a rat model, Lawrance et al. (21) showed that omentectomy 3–4 wk before intraperitoneal or intraluminal tumor cell inoculation significantly reduced intraabdominal tumor growth. Weese et al. (22) studied the influence of the omentum on intraperitoneal tumor growth in a rat model of peritoneal carcinomatosis of colonic origin and found that omentectomy reduced the incidence of small bowel obstruction by >50%. Thus, the omentum has been implicated as an initial site of tumor growth, after which secondary seeding occurs at sites of peritoneal trauma.
Although cytoreductive surgery and adjuvant intraperitoneal chemotherapy are increasingly being accepted as one of the treatment options for patients with peritoneal carcinomatosis of colorectal origin, there is little experimental evidence on the efficacy of this treatment. Benoit et al. (23) studied the efficacy of surgical cytoreduction, intraperitoneal chemotherapy using cisplatin/epinephrine, or both treatment modalities in BDIX rats with peritoneal carcinomatosis of colonic origin. Whereas cytoreductive surgery alone did not improve survival, intraperitoneal chemotherapy alone significantly improved survival without curing any of the animals. However, cytoreductive surgery followed by intraperitoneal chemotherapy cured 4 of 5 animals.
Because the uptake of radiolabeled mAbs is inversely correlated with tumor size (24), the efficacy of radioimmunotherapy, theoretically, should be higher in smaller tumor deposits. Therefore, we hypothesized that the combination of cytoreductive surgery followed by radioimmunotherapy would act additively. Indeed, the combination of both treatment modalities resulted in the highest median survival and a highly significant trend toward improved survival, when compared with both cytoreductive surgery only and exploratory laparotomy + radioimmunotherapy. The majority of rats were euthanized because of the development of massive hemorrhagic ascites. Interestingly, whereas the amount of ascites at the time of dissection was similar between the groups, rats treated with radioimmunotherapy, preceded by either exploratory laparotomy or cytoreductive surgery, showed (significantly) less solid tumor growth when compared with those treated with exploratory laparotomy or cytoreductive surgery only. Apparently, radioimmunotherapy effectively inhibited tumor growth but was not able to prevent the formation of ascites.
CONCLUSION
To our knowledge, this is the first experimental study on the efficacy of combined modality treatment including surgery and radioimmunotherapy in an animal model of cancer. Radioimmunotherapy using the 177Lu-MG1 mAb effectively inhibited tumor growth, even at relatively low-activity doses. When given postoperatively after cytoreductive surgery in rats with peritoneal carcinomatosis of colonic origin, radioimmunotherapy was associated with improved survival as compared with both cytoreductive surgery and radioimmunotherapy alone. This study provides proof of principle that radioimmunotherapy can be an effective treatment modality when applied as an adjuvant treatment after resection of tumors with a high risk of recurrence.
Acknowledgments
The authors thank Julliette van Eerd, PhD (Radboud University Nijmegen Medical Center, Department of Nuclear Medicine), for assistance in the radiolabeling procedures; Roger Lomme and Ben de Man (Radboud University Nijmegen Medical Center, Department of Surgery) for technical assistance during the operative procedures; and Henny Eikholt and Bianca Lemmers-de Weem (Radboud University Nijmegen Medical Center, Central Animal Laboratory) for their excellent technical assistance in the animal experiments. Part of this study was supported by grant 920-03-220 from The Netherlands Organization for Health Research and Development.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication March 1, 2006.
- Accepted for publication April 21, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- ImmunoSPECT and ImmunoPET of IGF-1R Expression with the Radiolabeled Antibody R1507 in a Triple-Negative Breast Cancer Model
- Microdistribution of Targeted, Fluorescently Labeled Anti-Carcinoembryonic Antigen Antibody in Metastatic Colorectal Cancer: Implications for Radioimmunotherapy
- Adjuvant and Combined Radioimmunotherapy: Problems and Prospects on the Road to Minerva