


Abstract
A carcinoid crisis is a severe complication of the carcinoid syndrome that can arise in patients with advanced metastatic neuroendocrine tumors. It can be initiated by stress, catecholamines, and tumor manipulation. In this article, we report a case in which an injection with the catecholamine tracer 6-18F-fluorodihydroxyphenylalanine, used for PET, induced a carcinoid crisis. Octreotide can be used for treatment and should be available. Tracer injection should be slow.
The carcinoid syndrome can occur in patients with a metastasized midgut carcinoid. This syndrome is characterized by episodes of flushing, diarrhea, abdominal pain, and wheezing (1–3). A carcinoid crisis is a serious complication of the carcinoid syndrome. A crisis is characterized by a sudden onset of different symptoms at once; these symptoms can consist of prolonged cutaneous flushing, severe dyspnea, peripheral cyanosis, tachycardia, and sometimes hemodynamic instability, which can be fatal (4–6).
In recent years, PET with 6-18F-fluorodihydroxyphenylalanine (18F-DOPA) has emerged as a new and accurate modality for the imaging of neuroendocrine tumors (7,8). 18F-DOPA is an amino acid but is also an important precursor in catecholamine metabolism. In this article, we report a case in which the rapid intravenous administration of a bolus of 18F-DOPA, used for a PET study, initiated a carcinoid crisis.
CASE REPORT
A 61-y-old woman with extensive liver metastases from a carcinoid tumor was referred to our PET center for an 18F-DOPA PET scan. She participated in a diagnostic research project that was approved by the local institutional review board and had given informed consent. One and a half years earlier she had been diagnosed with carcinoid disease and elevated 5-hydroxyindoleacetic acid (5-HIAA) excretion on the basis of a primary tumor in the ileum and extensive liver metastases. To alleviate symptoms of diarrhea she received 20 mg of slow-release octreotide intramuscularly every 4 wk. Despite this treatment, she was still experiencing episodes of diarrhea and flushing at the time of referral for the PET scan. During the last 2 visits to the outpatient clinic, her blood pressure was 190/100 mm Hg. In the preceding month, her urinary 5-HIAA level had risen slightly from 102 to 124 mmol/mmol of creatinine. Since the age of 52 y, she had had type 2 diabetes, for which she received glibenclamide.
In accordance with our scanning protocol, she received 150 mg of carbidopa orally after 6 h of fasting. One hour later, a bolus of 160 MBq of 18F-DOPA with a specific activity of 6 GBq/mmol was administered intravenously in a few seconds. The total injected volume was 8 mL and consisted of 5.63 mg of 18F-DOPA and 6 mL of 0.9% NaCl. Radiosynthesis of 18F-DOPA had been performed according to the method described by De Vries et al. and was no different from previous syntheses (9). At approximately 3 min after injection, she complained about a strange feeling in the abdomen extending to her chest, shortness of breath, and nausea but no itching. These symptoms were followed by severe vomiting. A physical examination revealed facial flushing with facial edema, peripheral cyanosis, and thoracic erythema. Her blood pressure was 185/90 mm Hg, and her heart rate was regular, at 72 beats per minute. An electrocardiogram was normal. Her blood glucose level was 8.6 mmol/L. She was given 2 mg of the antihistamine clemastine (Tavegil; Novartis) intravenously. At approximately 10 min after this injection, her vomiting stopped, and her other complaints slowly diminished in the next 30 min. She believed that she was fit to be scanned, and 1 h after injection of 18F-DOPA, the scan procedure was started (Fig. 1). When the scan was finished, blood and urine samples were collected to evaluate for histamine, catecholamines, and serotonin metabolites. These data could be compared with measurements that had been obtained in the morning, before the PET scan. Finally, she went home in good condition approximately 2 h after the injection.
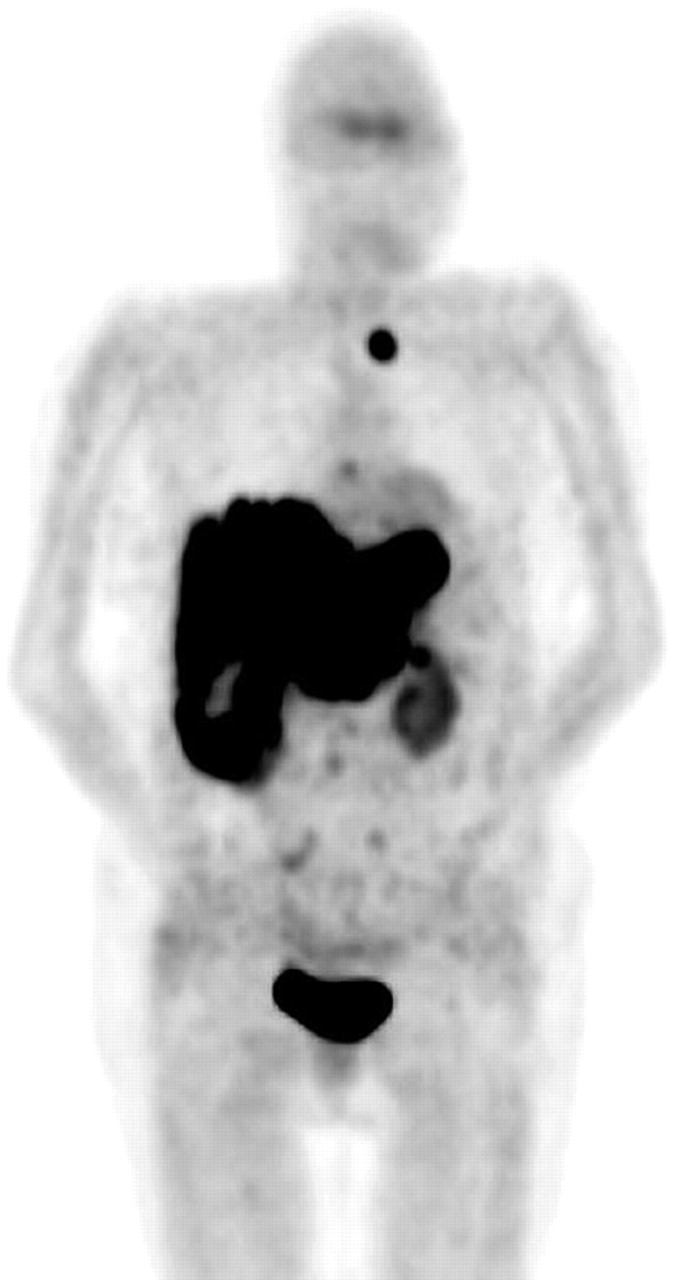
Anterior projection image from 18F-DOPA PET scan showing extensive liver metastases and supraclavicular lesion. Note physiologic uptake in striatum, kidneys, and bladder.
Two weeks later, she told us that she had experienced similar, but less severe, episodes (without vomiting and peripheral cyanosis) spontaneously before. On the basis of these symptoms and the increase in the urinary 5-HIAA level, the slow-release octreotide dose was increased from 20 mg to 30 mg monthly.
DISCUSSION
Initially, we ascribed the symptoms of this patient to an anaphylactic reaction caused by the injection of 18F-DOPA. We treated her for this reaction by administering an antihistamine. However, on the basis of additional clinical and biochemical information, it appears that this incident was a carcinoid crisis induced by the injection of 18F-DOPA.
Laboratory parameters are important for determining the nature of such incidents. During anaphylaxis, mast cells and basophils degranulate on activation by cross-linking of mast cell–bound IgE with antigen or complement components. Products released during this degranulation include histamine, prostaglandins, leukotrienes, platelet-activating factor, and tryptase. Evidence in support of a diagnosis of anaphylaxis includes increased serum tryptase levels and increased levels of urine N-methylhistamine, a histamine metabolite that remains elevated for several hours (10,11). In our patient, tryptase and urine N-methylhistamine levels were within normal ranges (Table 1), a finding that virtually excludes an anaphylactic reaction as the cause for the incident.
Blood and Urine Measurements Before and After Scanning
A carcinoid crisis is the result of a massive release of serotonin and other products, such as histamine, kallikreins (12), or catecholamines (13). In particular, levels of serotonin and its metabolites (5-HIAA) are elevated and remain so for several hours (14–16). In our patient, the urinary 5-HIAA level doubled within a few hours. In addition, the serum tryptophan level declined by 50% (Table 1). From these values, it can be concluded that there was a period of massive serotonin production and release that, together with her symptoms and history, was diagnostic of a carcinoid crisis (17). The low level of tryptophan, the first precursor in the serotonin pathway, confirms the increased activity of this pathway.
Various causes for the carcinoid crisis have been reported. Besides mechanical stimulation of the tumor and triggering by catecholamines (especially noradrenaline), a carcinoid crisis also can be triggered by stress, hypercapnia, hypothermia, hypotension, hypertension, initiation of chemotherapy, or drugs that cause a release of histamine (5,12,15,18–20). In our patient, rapid injection with the catecholamine tracer 18F-DOPA triggered the release of serotonin by the tumor cells, thus initiating the carcinoid crisis.
Possible mechanisms for the initiation of a carcinoid crisis by 18F-DOPA include the local conversion in tumor tissue of 18F-DOPA to noradrenaline, induced by the enzymes aromatic acid decarboxylase and dopamine β-hydroxylase. These enzymes, especially aromatic acid decarboxylase, can be abundantly present in carcinoids and remain active even in the presence of carbidopa (21,22). Noradrenaline then can stimulate the tumor cells to release serotonin. This mechanism seems most likely, because the amount of the injected tracer was relatively high (5.63 mg) as a result of the low specific activity. Another mechanism may be local irritation of the vessel walls of the adrenal gland by 18F-DOPA. The adrenergic system then can release noradrenaline, which in turn can stimulate the tumor cells to release serotonin. Similarly, it has been proposed that the rapid uptake of 123I-metaiodobenzylguanidine in chromaffin granules, either in the normal adrenal gland or in tumor tissue, may cause rapid noradrenaline secretion.
Every neuroendocrine tumor that produces and stores serotonin and catecholamines in secretory granules could react with a massive outpouring of hormones, thus initiating the carcinoid crisis. However, patients most at risk are probably patients with preexisting carcinoid syndrome and the existence of extensive liver metastases or of metastases in another part of the body where the venous blood flow directly enters the systemic circulation. There are currently no risk factors that can indicate which of these patients will develop a carcinoid crisis (1).
Differentiating a carcinoid crisis from a severe episode of the carcinoid syndrome can be difficult, and there is a gradual transition. However, the hallmark of a carcinoid crisis is the sudden (violent) onset of different symptoms at once. Our patient developed symptoms that were much more severe and diverse shortly after the injection of 18F-DOPA than the symptoms that she usually experienced during an episode of her carcinoid syndrome. Also, her biochemical findings suggested that she had gone through an episode with a massive release of serotonin. Therefore, it seems more likely that our patient experienced a carcinoid crisis instead of a severe episode of her carcinoid syndrome.
Considering the severity of a carcinoid crisis, preventive measures should be taken, and nuclear medicine workers must be aware of this risk and its treatment. These caveats have become more relevant, because the application of 18F-DOPA PET seems to have become increasingly valuable for patient care. A preventive measure could be to administer 18F-DOPA slowly instead of as a bolus. By avoiding rapidly building peak first-pass concentrations, slow injection most likely can prevent a rapid secretion of noradrenaline by tumor cells. This strategy is similar to the advice given for the administration of 123I-metaiodobenzylguanidine. Treatment of a carcinoid crisis should consist of blocking the release of the mediators from tumor tissue by administering somatostatin analogs, such as octreotide (20,23). In the acute situation, 100–500 μg of octreotide can be safely administered intravenously (6). Ketanserin has been used successfully in patients with a carcinoid crisis to block the actions of mediators. It is a selective antagonist of the 5-hydroxytryptamine receptor 2, the α1-adrenoreceptor, and the H1-histamine receptor and decreases the central sympathetic outflow (23). Ketanserin can be given as a 10-mg intravenous bolus injection. Catecholamines should never be used for the treatment of hypotension, as they may stimulate tumor cells to release even more serotonin.
CONCLUSION
We present a case of a patient who had a carcinoid tumor and extensive liver metastases and who developed a carcinoid crisis after injection with 18F-DOPA. As a carcinoid crisis can be fatal, PET centers using 18F-DOPA for the imaging of patients with biochemically active and metastasized carcinoid disease should be aware of this rare syndrome. The tracer must be administered slowly, and intravenous somatostatin analogs and perhaps also ketanserin should be available to treat this condition.
Acknowledgments
This work was supported by grant 2003-2936 from the Dutch Cancer Society.
Footnotes
As an exception to the JNM policy of not publishing case reports, the editors deemed the information presented in this study to be of importance for clinicians and investigators using 18F-DOPA for clinical studies.
Received Jan. 19, 2005; revision accepted Mar. 23, 2005.
For correspondence or reprints contact: Pieter L. Jager, MD, PhD, Department of Nuclear Medicine and PET Center, University Medical Center Groningen, P.O. Box 30.001, 9700 RB Groningen, The Netherlands.
E-mail: p.l.jager{at}nucl.azg.nl
REFERENCES
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- In Vivo Biodistribution of No-Carrier-Added 6-18F-Fluoro-3,4-Dihydroxy-L-Phenylalanine (18F-DOPA), Produced by a New Nucleophilic Substitution Approach, Compared with Carrier-Added 18F-DOPA, Prepared by Conventional Electrophilic Substitution
- 6-L-18F-Fluorodihydroxyphenylalanine PET in Neuroendocrine Tumors: Basic Aspects and Emerging Clinical Applications
- The Effects of Carbidopa on Uptake of 6-18F-Fluoro-L-DOPA in PET of Pheochromocytoma and Extraadrenal Abdominal Paraganglioma
- Further delineation of the continuous human neoplastic enterochromaffin cell line, KRJ-I, and the inhibitory effects of lanreotide and rapamycin
- Safety of 18F-DOPA Injection for PET of Carcinoid Tumor