


Abstract
We used gated SPECT to evaluate the impact of abciximab on the efficacy of myocardial reperfusion in patients with acute myocardial infarction undergoing infarct-related artery stenting. Methods: The Abciximab and Carbostent Evaluation (ACE) trial randomized 400 infarct patients to stenting alone or stenting plus abciximab. One-month 99mTc-sestamibi gated SPECT was planned in a subgroup of consecutive patients to evaluate infarct size, infarct severity, left ventricular volumes, and ejection fraction. Results: The final study population included 182 patients (99 randomized to abciximab and 83 to stenting alone). Gated SPECT revealed smaller infarcts in the abciximab group than in the stenting-alone group (14.3% ± 11.7% vs. 18.1% ± 13%, P < 0.02), and lower infarct severity (minimum-to-maximum count ratio = 0.47 ± 0.17 vs. 0.41 ± 0.15, P < 0.02), resulting in a smaller left ventricular end-diastolic volume index (57.8 ± 20.0 vs. 64.6 ± 20.8 mL/m2, P = 0.03) and left ventricular end-systolic volume index (31.7 ± 17.4 vs. 37.5 ± 18.6 mL/m2, P = 0.05) in the abciximab group. One-month left ventricular ejection fraction was significantly higher in patients randomized to abciximab (47.4% ± 11.3% vs. 43.9% ± 11.7%, P = 0.05). Conclusion: The use of abciximab therapy as an adjunct to infarct-related artery stenting leads to a reduction in infarct size and severity, resulting in smaller 1-mo left ventricular volumes and better left ventricular function. Gated SPECT appears to be an ideal tool for outcome assessment in infarct patients undergoing different treatment strategies.
Several studies comparing primary coronary angioplasty with primary infarct artery stenting for acute myocardial infarction have shown that primary stenting improves the procedural success rate and clinical outcome (1–6). The impact of abciximab therapy as an adjunct to stenting on the efficacy of myocardial reperfusion and myocardial salvage has not yet been defined, and completed randomized trials comparing stenting alone with stenting plus abciximab have not assessed the effect of abciximab treatment on the final infarct size (6–9). The Abciximab and Carbostent Evaluation (ACE) trial randomized 400 patients with acute myocardial infarction to infarct artery stenting alone or stenting plus abciximab (10). The ACE scintigraphic study sought to determine the effect of abciximab treatment on myocardial salvage by assessing infarct size and severity, together with left ventricular function, by 1-mo 99mTc-sestamibi gated SPECT in a subgroup of the ACE trial cohort.
MATERIALS AND METHODS
Study Protocol and Patient Population
Since 1995, primary percutaneous transluminal coronary angioplasty has been the systematic treatment at our institution for all patients with acute myocardial infarction admitted within 6 h of symptom onset or within 24 h in cases of ongoing ischemia, without any restriction on age, sex, or clinical status at presentation. The details of the ACE trial, which was based on this premise, have already been published (10). In brief, the enrollment criteria were as follows: chest pain persisting more than 30 min and associated with ST-segment elevation of at least 0.1 mV in 2 or more contiguous electrocardiographic leads, and admission within 6 h of symptom onset or between 6 and 24 h if continuing ischemia was evident. The exclusion criteria were previous administration of fibrinolytic or abciximab therapy, a history of bleeding diathesis or allergy to the study drug, major surgery within 15 d, active bleeding, participation in another study, and inability to obtain informed consent. All patients with a vessel reference diameter of at least 2.5 mm were eligible for stenting and randomization.
After coronary angiography, which was performed as previously described, patients were randomly assigned to stenting alone or stenting plus abciximab. Patients randomized to abciximab received the drug immediately before the procedure as a bolus of 0.25 mg/kg of body weight followed by a 12-h infusion at a rate of 0.125 μg/kg/min. Heparin was given as an initial bolus of 70 U/kg, and additional boluses were administered during the procedure to achieve an activated clotting time of 200–300 s in patients assigned to abciximab or at least 300 s in patients assigned to stenting alone. In the group assigned to stenting alone, crossover to abciximab was strongly discouraged. Immediately after the procedure, patients received 500 mg of ticlopidine or 300 mg of clopidogrel. Patients were routinely treated with aspirin (325 mg/d indefinitely) and with ticlopidine (500 mg/d for 1 mo) or clopidogrel (75 mg/d for 1 mo).
Coronary angiography was analyzed with consideration of the Thrombolysis In Myocardial Infarction (TIMI) grade flow, corrected TIMI frame count, diameter of the reference infarct artery, and minimum lumen diameter. These quantitative angiographic parameters were assessed as previously described (10–13).
During the acute phase after admission, 12-lead electrocardiography was repeatedly performed to assess the ST segment, and early resolution in ST-segment elevation was defined as a decrease by at least 50% in ST-segment elevation at 30 min after infarct artery recanalization (14). Creatine kinase was systematically measured on admission, every 3 h for the subsequent 24 h, and then every 12 h for 2 d.
Resting 99mTc-sestamibi SPECT had been planned 1 mo after index infarction for the determination of infarct size in a prespecified subgroup of the first 250 consecutive patients enrolled in the centers with nuclear medicine facilities: 130 patients were randomized to stenting plus abciximab and 120 to stenting alone. Of them, 8 died during hospitalization (2 of the abciximab and 6 of the stenting-alone group), and 12 (6 of each randomization group) dropped out of the study before the 1-mo follow-up. Of the remaining 230 patients who underwent SPECT at 1 mo, 15 (7 of the abciximab group) were enrolled in a center without the capability of acquiring SPECT with electrocardiographic gating and 9 (5 of the abciximab group) could not studied because of technical problems or severe arrhythmia preventing gating. Finally, 24 patients (11 of the abciximab group) had had a previous myocardial infarction precluding evaluation of the index infarct size. Thus, the final study population with complete gated SPECT data included 182 patients (99 randomized to abciximab and 83 to stenting alone).
Gated SPECT
Gated SPECT acquisition began 60 min after 99mTc-sestamibi injection (740 MBq), using a double-head camera equipped with high-resolution collimators, a 180° rotation arc, 34 projections, 60 s per projection, 8 frames per heart cycle, and 64 × 64 matrices. The studies were reconstructed using filtered backprojection without attenuation or scatter correction and realigned along the heart axis. Perfusion defects were quantified as percentage of left ventricular wall, with the defect threshold set at 60% of peak uptake (15). Infarct severity was defined as the lowest ratio of minimal to maximal counts in the short-axis slices evaluated for infarct size (16, 17). Left ventricular end-diastolic volume and end-systolic volume and ejection fraction were measured by an automated and validated method (18). Volumetric data were corrected for body surface area and expressed as indexes.
Statistical Analysis
Results are expressed as mean value ± SD. Groups were compared with the Student t test for unpaired samples. Proportions were compared using the χ2 test. A P value of less than 0.05 was considered statistically significant.
RESULTS
General Findings
Table 1 summarizes the baseline characteristics of the patients. The baseline characteristics of the scintigraphic study patients were similar to those of the general study patient cohort (10). The 2 groups of patients of the scintigraphic study were similar in all baseline characteristics, and there was a trend toward a higher incidence of elderly patients in the abciximab group.
Baseline Characteristics of Patients
Table 2 summarizes the details and the results of the percutaneous procedure. All patients randomized to abciximab did receive abciximab treatment, and crossover to abciximab occurred in 8% of patients of the stenting-alone group because of procedural complications or suboptimal angioplasty results.
Procedural Details and Results
Myocardial Perfusion
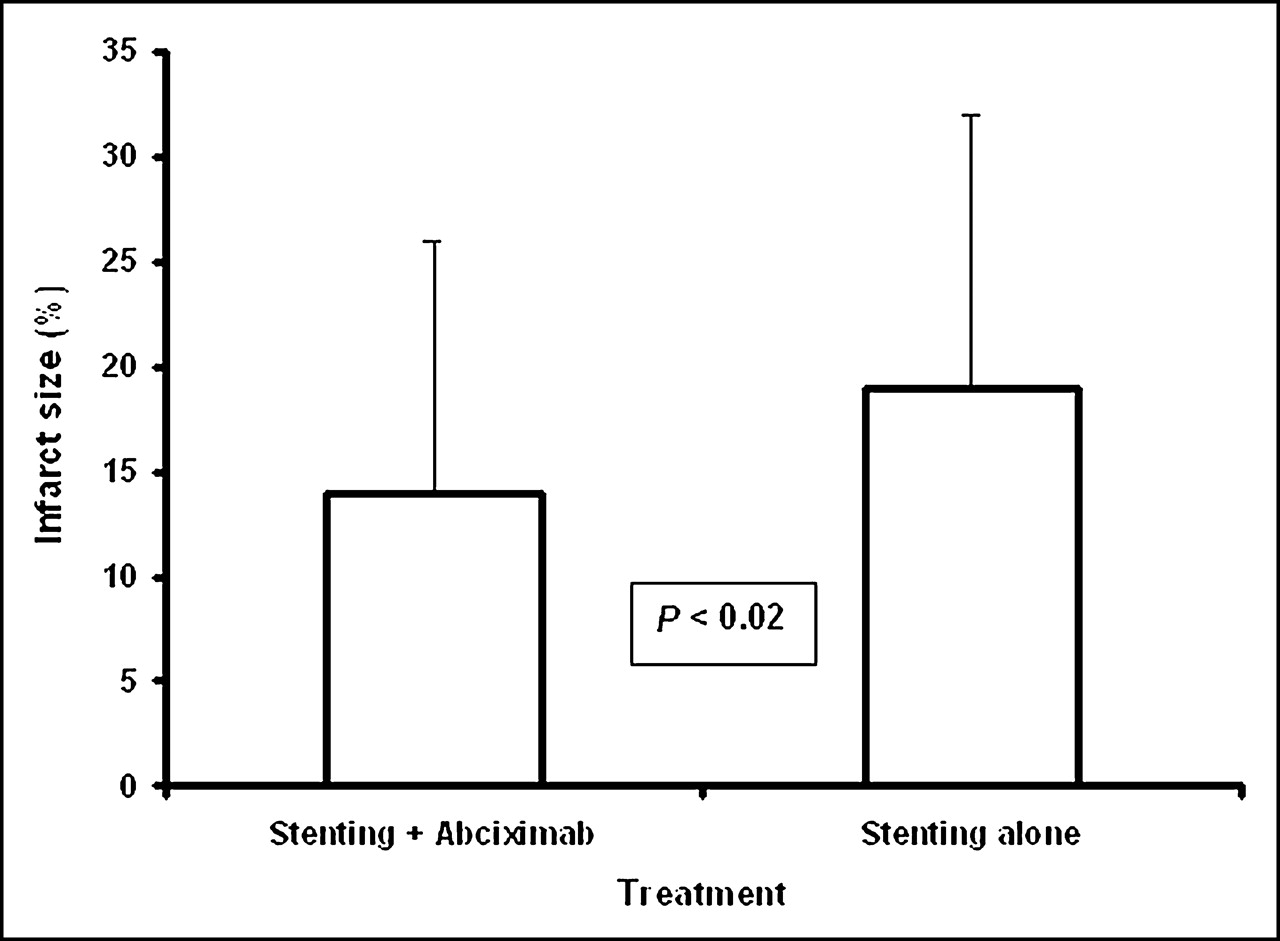
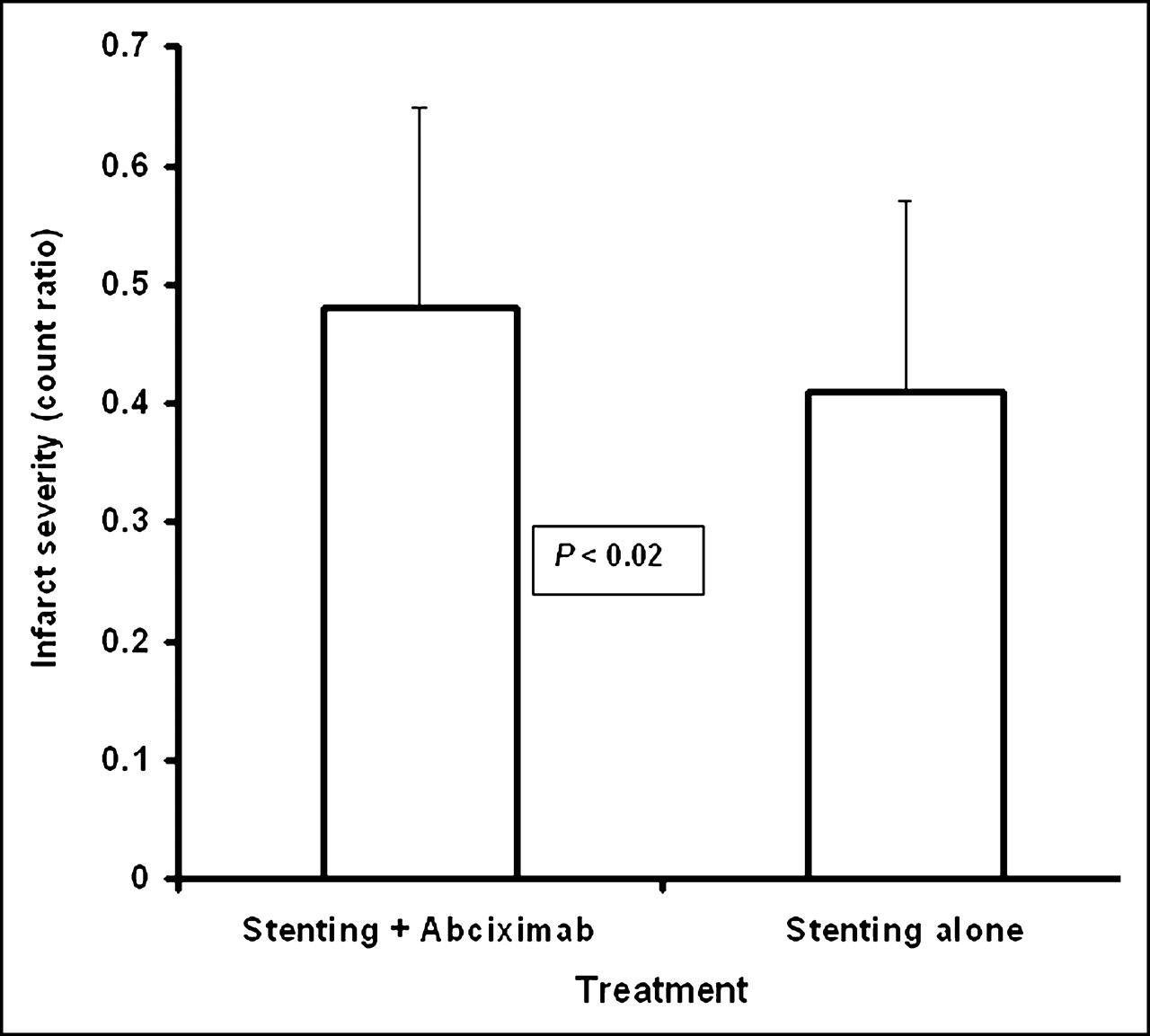
One-month gated SPECT revealed significantly smaller infarcts in the abciximab group than in the stenting-alone group: 14.3% ± 11.7% versus 18.1% ± 13%, P < 0.02 (Fig. 1). The infarcts in the abciximab group were also less severe, with a significantly higher count ratio: 0.47 ± 0.17 versus 0.41 ± 0.15, P < 0.02 (Fig. 2).

Bar graph showing difference in infarct size between patients treated with stenting plus abciximab and those treated with stenting alone.

Bar graph showing difference in infarct severity (ratio of minimum over maximum counts within infarct) between patients treated with stenting plus abciximab and those treated with stenting alone.
Left Ventricular Functional Data
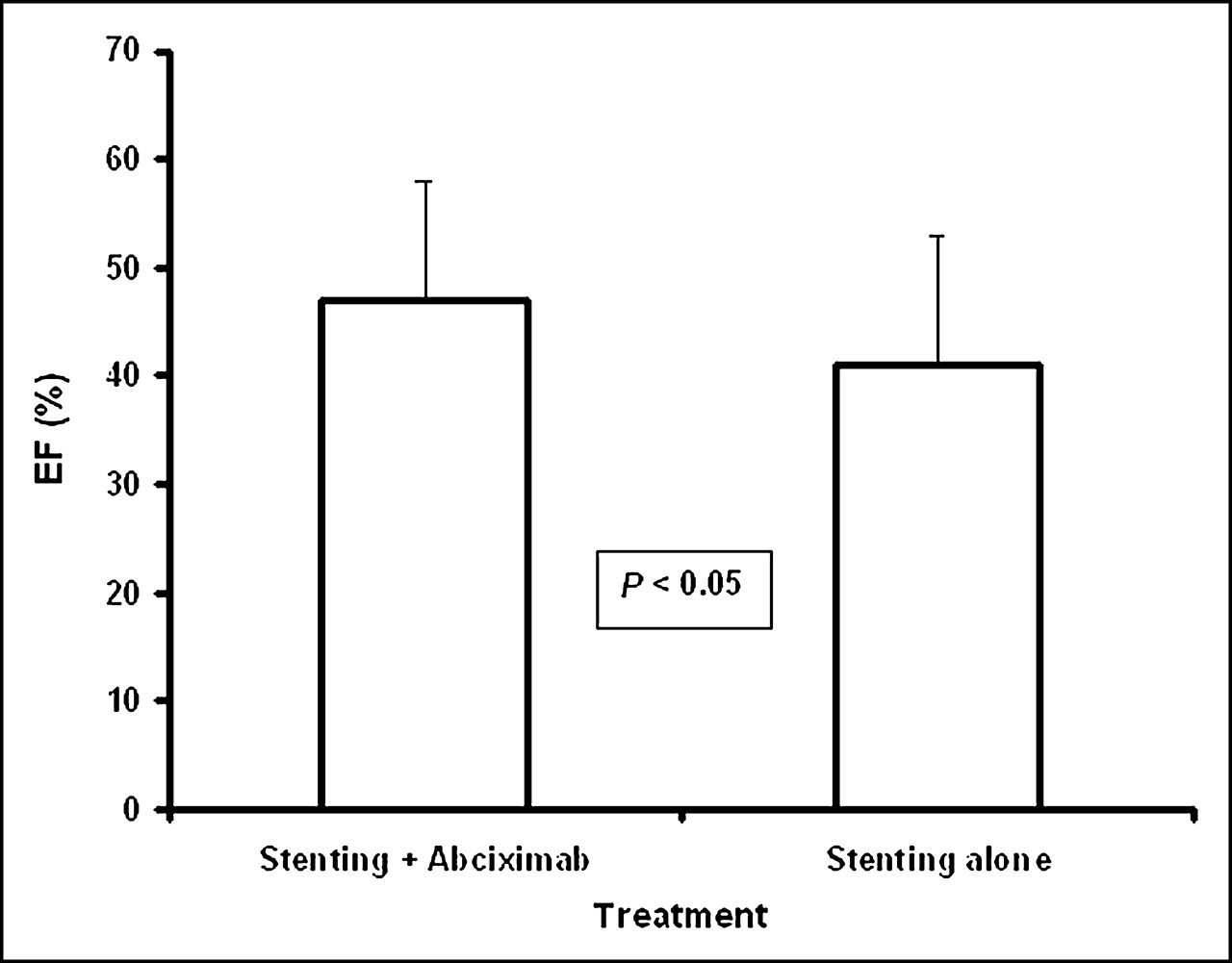
Both left ventricular volumes were significantly smaller in the abciximab group than in the stenting-alone group: the end-diastolic volume index was 57.8 ± 20.0 versus 64.6 ± 20.8 mL/m2, P = 0.03, and the end-systolic volume index was 31.7 ± 17.4 versus 37.5 ± 18.6 mL/m2, P = 0.05 (Fig. 3). Consequently, the left ventricular ejection fraction was significantly higher in the abciximab group than in the stenting-alone group: 47.4% ± 11.3% versus 43.9% ± 11.7%, P = 0.05 (Fig. 4).

Bar graph showing difference in left ventricular volume indexes between patients treated with stenting plus abciximab and those treated with stenting alone. End-diastolic volume = white bars; end-systolic volume = black bars.
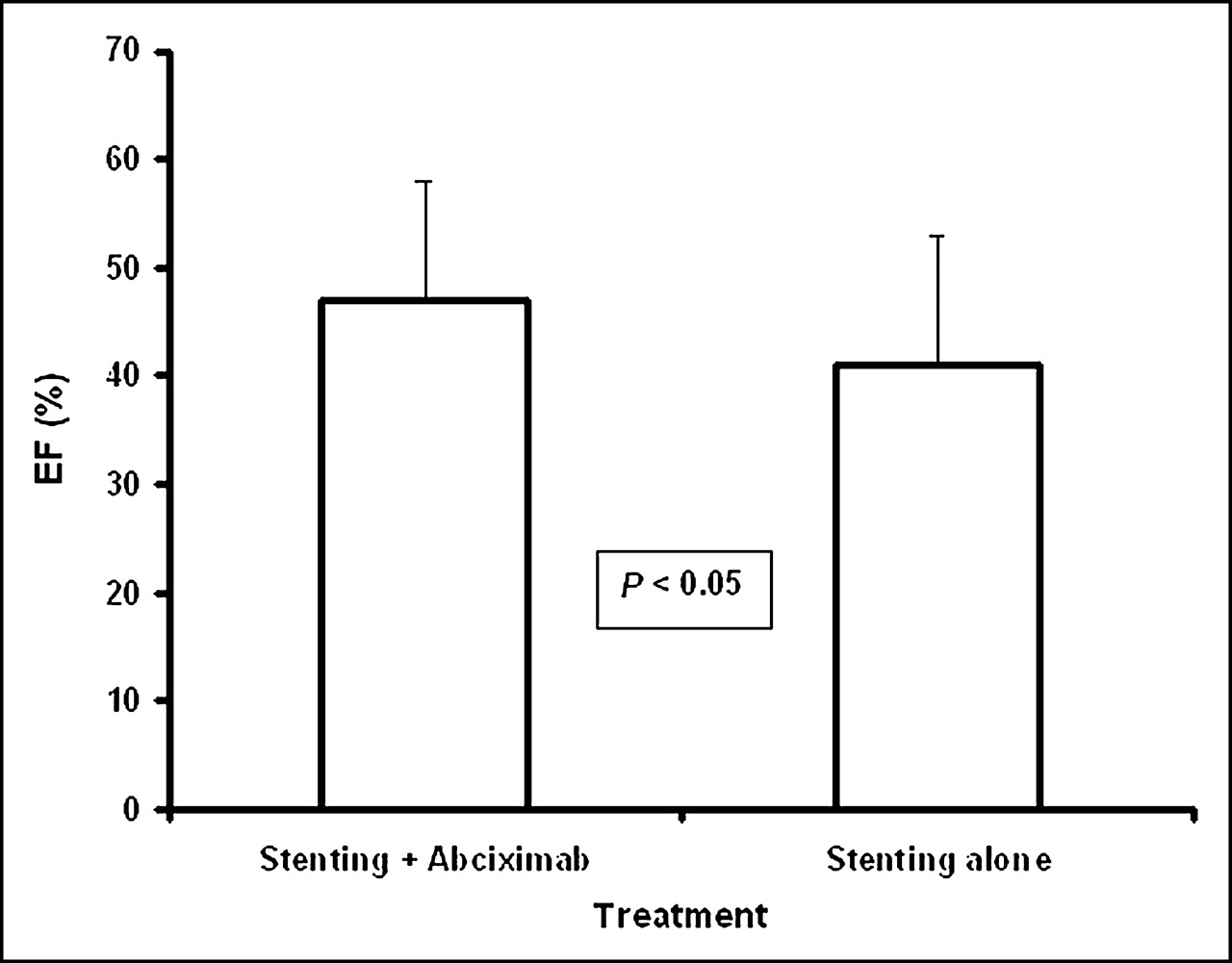
Bar graph showing difference in left ventricular ejection fraction between patients treated with stenting plus abciximab and those treated with stenting alone. EF = ejection fraction.
DISCUSSION
The ACE Trial
The ACE trial has shown that abciximab provides a better clinical outcome than does stenting alone in patients who have acute myocardial infarction with ST-segment elevation. In the general patient cohort, the use of abciximab reduced the rate of the 1-mo composite of death, reinfarction, target vessel revascularization, and stroke. At 6 mo, the reduction in mortality increased, resulting in a significant reduction in the composite of death and reinfarction (10). At 1 y, the survival and event-free survival rates were higher in patients randomized to abciximab (19).
The results of the scintigraphic study suggest that the link between abciximab treatment and improvement in short- and long-term clinical outcome might be, at least in part, a more effective reperfusion resulting in increased myocardial salvage. Patients with a first acute myocardial infarction randomized to abciximab treatment had a final smaller infarct size and lower infarct severity. Furthermore, according to the functional data derived from the gated SPECT evaluation, left ventricular volume indexes were significantly smaller and the ejection fraction significantly higher in the abciximab group than in the stenting-alone group. These results are consistent with those of the ADMIRAL trial (9). The relationship of the more favorable outcome to more effective reperfusion at the tissue level in abciximab-treated patients was confirmed by their higher rate of early ST-segment resolution, which is a robust marker of the effectiveness of reperfusion and relates directly to the extent of myocardial salvage (20). Moreover, this parameter is known to correlate inversely with infarct size (14,21). The faster creatine kinase release from the infarcted tissue in the abciximab group supports, as well, the hypothesis of a more effective reperfusion in these patients (22).
Previous Trials
Three trials comparing abciximab plus stenting with stenting alone did not assess directly the effectiveness of myocardial reperfusion and salvage (6,8,9). The results of these studies were negative, or showed that the benefit of abciximab was mainly due to the protection against early failure of infarct-related artery recanalization. In contrast, a randomized trial from the Munich investigator group demonstrated that patients randomized to abciximab had more improved microcirculatory function, assessed by coronary Doppler velocity measurements, and a higher angiographic left ventricular ejection fraction than did patients randomized to placebo (7). This study showed that abciximab better protects the coronary microcirculation, which in turn is the prerequisite for increased myocardial salvage and left ventricular functional recovery.
The Effects of Abciximab on Reperfusion
It has been hypothesized that abciximab, beyond the antithrombotic effects on platelet aggregates, may interact with receptors other than the glycoprotein IIb/IIIa receptor and inhibit the complex inflammatory cascade that contributes to the obstruction and disruption of the microvessel network after reperfusion (23,24). These inhibitory effects yield a more complete myocardial reperfusion and myocardial salvage, with the potential for increased survival. Previous studies, using ST-segment resolution or coronary flow velocity measurements as markers of reperfusion, could reveal only indirectly the higher efficacy of reperfusion provided by abciximab (7,25). The ACE scintigraphic study, by finding smaller and less severe infarcts in abciximab-treated patients, suggests that the “peripheral” effect of the drug might be a major determinant of the improved outcome as revealed by randomized and nonrandomized studies (8,9,19,26–28). This peripheral effect may remain clinically masked in patients with small infarcts (6). Conversely, the effect of abciximab may be clearly expanded in patients with a large area at risk.
Methodologic Issues
From the methodologic point of view, the most interesting feature of the present study was the use of gated SPECT to assess patient outcome and to compare different treatment strategies in acute myocardial infarction. Ideally, the acquisition of 2 perfusion studies, one showing the perfusion pattern before intervention and the other the treatment result, would be preferable (20,29,30). However, previous studies convincingly demonstrated that the scintigraphic estimate of infarct size could be a valuable surrogate endpoint for studies on treatment effectiveness in acute myocardial infarction (31). Also, infarct severity is important in predicting patient outcome in acute myocardial infarction (32). Most of this importance is related to the connection of infarct severity with infarct viability and to the prediction of left ventricular remodeling (33), underlining the major role of parameters characterizing left ventricular functional status in establishing prognosis (34). Therefore, the possibility of comprehensively characterizing both myocardial perfusion and left ventricular function using a single examination is a major strength of perfusion-gated SPECT in the current diagnostic arena. To our knowledge, this was one of the first studies in which gated SPECT could demonstrate not only less severe myocardial damage but also a significantly better functional outcome in patients with acute myocardial infarction treated by 2 different therapeutic strategies. Unfortunately, we were unable to assemble, in this scintigraphic substudy, a patient population large enough to permit a reasonable analysis of the relationship between gated SPECT data and prognosis, as was recently done for salvage index (30). Nevertheless, it is worth mentioning that the 1-y overall mortality in our patient population was 2% (4 deaths), with 1 patient in the abciximab group (group mortality, 1%) and 3 in the stenting-alone group (group mortality, 4%).
Study Limitations
We already mentioned the lack of perfusion data before intervention. Patients who underwent 99mTc-sestamibi gated SPECT were not randomized separately from the entire trial population. This limitation has, in theory, the potential for biasing the scintigraphic study cohort. However, the scintigraphic study population arose from consecutive patients randomized in the trial centers with nuclear medicine facilities. A large part of the numeric difference between the 2 groups could be explained by the initial planned randomization scheme (130 patients treated with abciximab vs. 120 treated with stenting alone) and, most important, by the higher number of in-hospital deaths in the stenting-alone group (6 vs. 2). Moreover, the 2 groups of patients with a first acute myocardial infarction were similar, and the scintigraphic patient cohort was comparable in all baseline characteristics to the overall study population.
CONCLUSION
The data of the present study support the general conclusion of the ACE trial, indicating a better outcome for patients with acute myocardial infarction treated with primary stenting plus abciximab than for those treated with stenting alone (10,19). In particular, the perfusion indicators of myocardial damage, such as infarct size and infarct severity, were significantly better in the abciximab group than in the stenting-alone group. Furthermore, taking advantage of the gated SPECT acquisition, we could demonstrate that in the abciximab group the left ventricular functional parameters, such as volumes and ejection fraction, were significantly better as well.
Acknowledgments
This study was supported by Sorin Biomedica and the ARCARD ONLUS Foundation.
Footnotes
Received Oct. 20, 2004; revision accepted Dec. 22, 2004.
For correspondence or reprints contact: Roberto Sciagrà, MD, Nuclear Medicine Unit, Department of Clinical Physiopathology, University of Florence, Viale Morgagni 85, 50134 Florence, Italy.
E-mail: r.sciagra{at}dfc.unifi.it
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.