


Abstract
Radioimmunotherapy (RIT) for pediatric tumors remains in its infancy despite its potential as an attractive therapeutic modality. Most childhood tumors are radiation sensitive, but the side effects of external beam radiation are well recognized. Despite achieving complete remissions with sophisticated combination therapies, treatment failure primarily results from the inability to eradicate minimal residual disease, which is typically distant and occult. RIT can conceivably target such disease and improve cancer treatment. Because intensive chemotherapy regimens used in most childhood cancers are highly immunosuppressive, repeated administration of radiolabeled monoclonal antibodies is possible without the immediate induction of human antimouse or human antichimeric antibody responses. Despite the differences in biology between childhood and adult hematologic malignancies, they share several tumor antigens for which RIT agents are now available. However, safety and efficacy profiles in children remain to be defined. On the other hand, the antigen repertoire of pediatric solid tumors differs substantially from that in adults, partly because of differing lineages: pediatric solid tumors are typically of embryonal origin, whereas adult tumors are usually carcinomas of epithelial origin. Hence, RIT agents licensed for adult tumors are generally not applicable to pediatric solid tumors. Tumor-selective radioimmunoconjugates specific for embryonal tumors of childhood are currently being actively investigated. Without substantial policy changes in drug development for orphan indications, however, these agents are not likely to be widely available in the near future.
Although survival in children with cancer has improved significantly over the last 4–5 decades, children with metastatic solid tumors and some children with hematologic malignancies continue to have poor prognoses despite treatment with multimodality therapy, including surgery, external beam radiation, and high-dose chemotherapy. Radioimmunotherapy (RIT) may be an effective adjunctive modality, particularly against minimal residual disease. Most pediatric cancers are radiation sensitive and are good candidates for RIT. RIT may potentially reduce organ toxicities associated with external beam radiation. These toxicities (e.g., growth impairment and asymmetry, learning difficulties, and other neurologic effects) are of particular significance in children. Moreover, because most children with cancer are treated with immunosuppressive, high-dose chemotherapy, passive immunotherapy with monoclonal antibodies (mAbs) is feasible without the rapid induction of human antimouse antibody (HAMA) or human antichimeric antibody responses. Despite these potential advantages, few antibodies are currently available for RIT in children with cancer. Reasons for this include: the different antigen repertoire of childhood neoplasms, particularly solid tumors, when compared with common adult tumors; delay in the implementation of phase I and II studies of available RIT agents in children; and the “orphan” status of pediatric cancers for which approaches and objectives of RIT may differ significantly from those for adult tumors.
PEDIATRIC TUMOR ANTIGENS FOR RADIOIMMUNOTHERAPY
Pediatric hematologic malignancies and brain tumors share antigens that have been targeted by RIT in adults. These are listed in Tables 1–3. Children with brain tumors have been treated on some RIT trials designed primarily for adults (4). However, reports documenting RIT targeting of hematological malignancies did not include pediatric patients (5–15). Two antigens expressed on a majority of childhood acute lymphoblastic leukemia (ALL), the pre-B antigen CD19 and the common ALL antigen CD10, have been targeted by 131I-HD37 and 131I-WCMH15.14, respectively (16,17).
Antigens on Pediatric Hematologic Malignancies Targeted by Radioimmunotherapy
On the other hand, most pediatric solid tumors do not express antigens that have been targeted by RIT in adults with solid tumors (Tables 2,3). The disialoganglioside GD2, an acidic glycosphingolipid found on the outer surface membrane of several pediatric solid tumors including neuroblastoma (NB), brain tumors, osteosarcoma, and desmoplastic small round cell tumor (DSRCT), is a pediatric solid tumor antigen that has been the most extensively studied for RIT (18,19). As an antigen for targeting by mAbs, it has several advantages: it is homogeneously expressed on cell membrane with high antigen density, particularly on NB (107 binding sites/cell); cross-reactivity with normal tissues is restricted to tissues of the central nervous system and some peripheral nerves; levels of circulating antigen in patients are generally not high enough to interfere with binding; and loss of GD2 from cell surface after antibody binding is rare (20,21). Of the several antibodies produced against GD2, 3 have been used clinically for radioimmunotargeting. 131I-3F8, a murine IgG3 targeted specifically to NB in preclinical experiments, produced a substantial dose-dependent shrinkage of NB xenografts (22). The murine IgG2a mAb 14G2a has demonstrated antitumor effects in murine NB xenograft models. 131I-14G2a and its chimeric counterpart 99mTc-ch14.18 have each been used for radioimmunotargeting of NB (23,24).
Antigens on Pediatric Extracranial Solid Tumors Targeted by Radioimmunotherapy
Antigens on Pediatric Brain Tumors Targeted by Radioimmunotherapy
Several other solid tumor antigens have been used for radioimmunotargeting. L1-cell adhesion module (L1-CAM) is a 200-kD isoform of L1-cell adhesion molecule expressed on NB and on renal carcinoma with normal tissue expression restricted to brain tissue and kidney (25). α-fetoprotein (AFP), a 70-kD glycoprotein, is expressed on hepatoblastoma, hepatocellular carcinoma, and germ cell tumors. Rhabdomyosarcomas (RMSs) express myosin on cell membrane protein, although it is also distributed on normal skeletal muscle. TP-1/TP-3 osteosarcoma-associated antigen, a cell-surface monomeric polypeptide with a molecular weight of 80 kD, is expressed on osteosarcoma and some soft tissue sarcomas, with normal tissue expression restricted to the adrenal medulla, proximal kidney tubules, endothelial cells, and actively proliferating osteoblastic cells (26). A recently described cell-surface glycoprotein with a molecular weight of 58 kD and recognized by the murine MoAb 8H9 is found on a broad range of pediatric solid tumors, including NB, osteosarcoma, Ewing’s sarcoma, DSRCT, RMS, Wilms’ tumor, and brain tumors, as well as some adult tumors, such as carcinomas and melanomas. Its expression in normal human tissues is highly restricted. Both among tumor types and within tumors, the antigen appears to be homogeneously expressed with cell surface localization. 131I-8H9 specifically targets RMS xenografts in mice (27–29).
RADIOIMMUNODETECTION OF PEDIATRIC TUMORS
Imaging of tumors with radiolabeled mAbs seeks to enhance the sensitivity and specificity of disease detection. More important, it provides vital pharmacokinetic information as well as dosimetry measurements, not easily available by conventional radiologic imaging modalities. The use of SPECT and PET has added greatly to precision in quantifying radioactivity targeted by radiolabeled antibodies in vivo. Nevertheless, few antibodies are currently available for radioimmunodetection (RID) in pediatric patients.
Neuroblastoma
Biodistribution of 131I-3F8 showed excellent tumor targeting in patients with NB. 131I-3F8 localized to NB at primary and metastatic sites in lymph nodes, bone marrow, and bone in 42 patients. When compared with 131I-metaiodobenzylguanidine (131I-MIBG) imaging or MR images, anti-GD2 (131I-3F8) was more sensitive and more specific in detecting sites of metastatic disease (Fig. 1). Eighteen of 20 patients with soft tissue disease identified on CT/MR imaging had positive 131I-3F8 scans. On surgical resection, one of the 2 negative tumors was determined to be ganglioneuroblastoma and the other had only microscopic foci of residual NB (30). 131I-3F8 had a relatively high tumor uptake of 0.08%–0.1% injected dose per gram (31). Similarly, the anti-GD2 antibodies 131I-14G2a (23) and 99mTc-ch14.18 have yielded positive scans in patients with NB. The latter has been reported to have higher sensitivity and specificity than 131I-MIBG in the detection of NB relapses in 18 patients studied. Metastases were detected earlier with 99mTc-ch14.18 and tumor uptake persisted for a shorter duration after anti-NB chemotherapy was initiated when compared with 131I-MIBG, indicating possible disease response (24). chCE7, a chimeric antibody that recognizes an L1-isoform, also has been used in RID in patients with NB. In a group of 7 patients with relapsed NB who were sequentially imaged with 131I-MIBG and anti-L1 (131I-chCE7), the latter targeted most tumor sites, although some discordance with results from conventional imaging modalities was observed (25).

Gamma-camera scan of a child with recurrent stage 4 neuroblastoma, imaged 48 h after injection of 131I-3F8 and showing diffuse metastases in skull and axial and appendicular skeleton. Also notable is the absence of nonspecific uptake in liver or spleen. Figures show uptake of 131I-3F8 in (A) left lateral skull; (B) anterior skull; (C) anterior torso; (D) right lateral skull; (E) lower extremities; and (F) posterior torso.
Rhabdomyosarcoma and Soft Tissue Sarcoma
111In-labeled antimyosin F(ab) fragments (111In-R11D10) have been used for the detection of myocarditis in adults and children. Because myosin is a cytoplasmic molecule, a breach in muscle sarcolemma (as in inflamed or necrotic muscle cells) is required for 111In-R11D10 F(ab) binding. In RMS, antimyosin antibodies have been found to permeate tumor cells by an undetermined mechanism. Three studies have used 111In-R11D10 F(ab) for RID of RMS. In one study of 8 patients with RMS, scans were true-positive in 4 patients, false-negative in 2 patients, and true-negative in 2 patients (32). In a subsequent study, 7 of 9 children with evaluable RMS had positive antibody scans, although scans were false-positive in one patient in the absence of evaluable disease (33). In a third study, 27 patients (21 of whom were younger than 14 y) with histologically proven RMS were imaged after injection with 111In-labeled antimyosin F(ab) fragments. Sensitivity and specificity, when compared with standard imaging modalities, were 82% and 73%, respectively (34). Antimyosin binding to other solid tumors, such as leiomyosarcoma and rhabdoid tumor, has also been reported, although detection of these tumors was less accurate (32–34).
Osteosarcoma
RID of osteosarcoma has been attempted using 131I-TP-1 F(ab)′2 fragments. In 5 patients with osteosarcoma imaged after injection with 131I-TP-1 F(ab)′2 fragments, tumor detection was possible in 3 patients: one with primary tumor in femur and the other 2 with pulmonary metastases. Four patients had tumors removed after injection of antibody. Tumor-to-blood ratios ranged from 1.2 to 4.2, compared with a range of 0.1 to 0.8 for normal tissues (26).
Other Pediatric Solid Tumors
The anti-α-fetoprotein (anti-AFP) antibody IMMU-30 labeled with 99mTc has been used to detect AFP-secreting testicular and mediastinal nongerminomatous germ cell tumors in adults and children. AFP scanning in this population of 45 patients had a sensitivity of 89% and specificity of 58% when compared with conventional imaging modalities and serum AFP measurement (35). Anti-AFP (99mTc-IMMU-30) has also detected hepatic lesions correlating with MR image findings in a child with hepatoblastoma with possible extrahepatic lesions who was being evaluated for liver transplant (36). The murine IgG1 131I-8H9, which recognizes a glycoprotein antigen expressed on a broad range of pediatric solid tumors, has shown promise in preclinical studies (27). Administered intravenously, it is currently being investigated in a phase 1 study at Memorial Sloan–Kettering Cancer Center as an imaging agent in children with relapsed or refractory solid tumors before consideration for possible future use in RIT. In a separate study, intrathecal 131I-8H9 is being evaluated for its immunodetection of solid tumors metastasizing to the leptomeninges.
RADIOIMMUNOTHERAPY OF PEDIATRIC TUMORS
The radiation sensitivity of most pediatric tumors is a strong rationale for exploring RIT as a potential adjunct to standard multimodality therapies. However, experience to date in the use of RIT in pediatric cancer is limited. The largest number of children undergoing RIT have been patients with NB treated with anti-GD2 (131I-3F8).
Neuroblastoma
NB is the most common extracranial solid tumor in pediatric patients. Stage 4 NB has a poor prognosis, despite being chemosensitive and radiosensitive. Large primary tumors, widespread metastases, and early development of chemoresistance have posed management challenges. GD2 is an optimal tumor target on NB for RIT for several reasons. It is homogeneously expressed among and within tumors, localized on the cell surface, and not easily modulated. Three other important attributes of GD2 are the large number of binding sites it provides for anti-GD2 mAbs, absence on blood and bone marrow cells, and restricted distribution on peripheral neural tissues. Although GD2 is present on neurons, the blood–brain barrier effectively prevents the mAb from crossing over to cause neurotoxicity. The lack of GD2 loss after antibody binding or treatment and the lack of interference of antibody localization by shed GD2 are also critical factors for tumor targeting (20,21). Both 99mTc-ch14.18 and 131I-3F8 have been successfully used for RID (24,30). 3F8 has been used in patients since 1986, and the therapeutic efficacy and safety of unlabeled 3F8 as well as of 131I-3F8 have been carefully studied (37,38). Given the radiation sensitivity of NB cells with limited repair mechanisms and the accessibility of NB cells in the marrow compartment to mAb, RIT targeted at GD2 has a compelling rationale.
The radiation toxicities of 131I-3F8 were defined in a phase 1 dose escalation study performed in 24 patients (aged 0.3–24.2 y at diagnosis) at Memorial Sloan–Kettering Cancer Center. Twenty-three patients had refractory stage 4 NB, and one had unresectable stage 3 disease with ascites. All completed treatment with intravenous 131I-3F8 at one of 7 dose levels: 6, 8, 12, 16, 20, 24, or 28 mCi/kg. All patients developed grade 4 myelosuppression requiring autologous bone marrow rescue (22 patients) or treatment with granulocyte macrophage colony stimulating factor (1 patient). One patient died of progressive disease before marrow reinfusion. Effects of acute toxicities included pain during infusion, fever, and mild diarrhea. No late extramedullary toxicities were reported, except for biochemical hypothyroidism, which was encountered despite thyroid protection with oral potassium iodide, liothyronine sodium, or both. Six patients survived more than 20 mo after antibody treatment. Of the 10 patients evaluable for response, 2 had complete response of bone marrow disease and 2 had partial response of soft tissue disease (Fig. 2). Average tumor dose was calculated to be 150 rad/mCi/kg, and cumulative blood radiation dose averaged 2,000 cGy at a dose of 740–888 MBq/kg. Total body dose was estimated to be 500–700 cGy, substantially less than the total body irradiation dose in myeloablative regimens that have been used before autologous transplant for NB (39,40). Based on the lack of extramedullary toxicities encountered in the phase 1 study, 131I-3F8 at a dose of 740 MBq/kg was added to a multimodality program (N7) for all high-risk NB patients. Forty-two newly diagnosed patients were enrolled, and 35 completed treatment with 131I-3F8. All patients engrafted after bone marrow rescue. Among the first 20 patients treated with 131I-3F8, median time to achieve absolute neutrophil count >500/μL was 16 d and to achieve platelet count >20,000/μL was 41 d. As in the phase 1 study, toxicities encountered included myelosuppression, fever, and hypothyroidism, with no extramedullary toxicity. However, one patient died of complications from infection. With continued follow-up (6–10 y from diagnosis), overall survival for NB patients newly diagnosed at >18 mo of age is approximately 40% (41). Absorbed dose was calculated using the DOSCAL program developed at Memorial Sloan–Kettering Cancer Center that implements S-factor. Based on tracer dosimetry, average doses for liver, spleen, red marrow, lung, and tumor were 0.06, 0.07, 0.06, 0.05, and 0.37 cGy/MBq, respectively (40). No unexpected late effects were reported among children treated on this regimen. In this group of patients who received high-dose chemotherapy before 131I-3F8, only 2 of 35 patients (6%) developed HAMA responses. These were transient, resolving spontaneously within 1–3 mo, permitting subsequent administration of unlabeled anti-GD2 (3F8). This was among the first studies in children to use myeloablative doses of 131I-labeled mAbs.
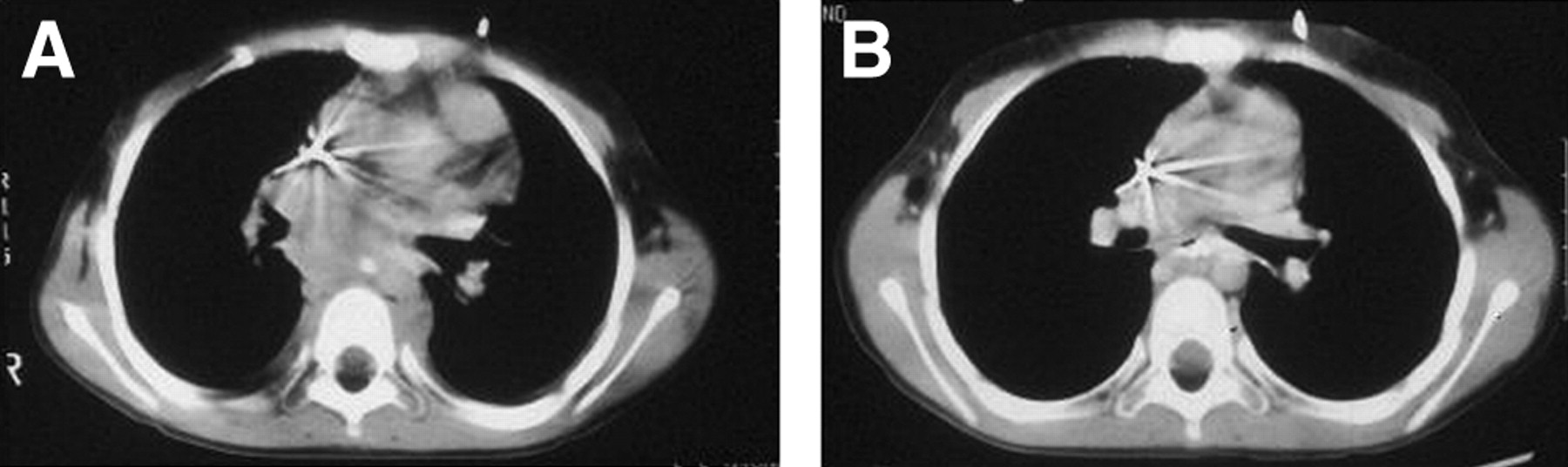
CT image of a child with recurrent MYNC-amplified neuroblastoma. Paraspinal soft tissue mass before (A) and after (B) 131I-3F8 therapy.
Brain Tumors
RIT trials in brain tumors have primarily focused on adults with poor-prognosis diseases such as high-grade gliomas. Because many of these tumors also occur in the pediatric patients, a few children have received treatment on these protocols. However, exact data on toxicity or efficacy of these agents specifically in children are unavailable. Eight pediatric patients with gliomas were treated with intrathecal 131I-81C6, an antitenascin radioimmunoconjugate, in a dose-escalation phase 1 study (4,42). The maximum tolerated dose was not reached in this study, and no objective responses were observed. In subsequent phase 1 and 2 studies investigating the intracavitary use of this agent, children younger than 18 y were not enrolled (43). Two pediatric patients, one with glioblastoma multiforme and one with anaplastic astrocytoma, have been treated with intravenous 125I-425, an antiepidermal growth factor receptor antibody (44), and one pediatric patient has been treated with intratumoral 90Y-ERIC-1, an anti-neural cell adhesion molecule antibody (anti-NCAM) (45). However, toxicities experienced by these patients were not described.
Leptomeningeal Metastases
Current therapies for leptomeningeal metastases are, for the most part, ineffective. One exception is in childhood central nervous system leukemia, where intrathecal chemotherapy combined with craniospinal irradiation result in relatively high salvage rates, particularly if relapse occurs >18 mo after initial diagnosis. However, for solid tumor or brain tumor metastases, the outlook remains bleak. 131I-labeled anti-NCAM antibody UJ13, and anti-L1 antibodies UJ181.4 and M340 have been used to treat patients with relapsed medulloblastoma/primitive neuroectodermal tumor and pineoblastoma (46,47). Of 13 pediatric patients treated, 6 had complete or partial responses, although all responses were transient, with patients surviving 1–39 mo after treatment (46,47). Based on pharmacokinetic and toxicology studies in nonhuman primates and efficacy demonstrated in preclinical rat models of leptomeningeal NB, a phase 1 study using intraventricularly administered escalating doses of anti-GD2 (131I-3F8) in patients with leptomeningeal disease is ongoing at Memorial Sloan–Kettering Cancer Center (48,49). The first 8 patients (7 children) with GD2-positive leptomeningeal disease were injected with 37–74 MBq 131I-3F8 through an implanted Ommaya reservoir. Side effects included self-limited fever, headache, and vomiting, but no significant myelosuppression. Focal 131I-3F8 uptake along the craniospinal axis consistent with tumor was seen in 7 patients. Calculated radiation dose to cerebrospinal fluid was 0.4–1.5 cGy/MBq and to blood was <0.05 cGy/MBq. HAMA was not observed in any patient (50). From these studies, it appears that compartmental RIT to target leptomeningeal disease is feasible.
Leukemia
The feasibility of using RIT in children with relapsed ALL has been tested in 7 children (aged 3–16 y) with second or subsequent leptomeningeal relapse by intrathecal injection of anti-CD19 (131I-HD37) or anti-CD10 (131I-WCMH15.14) (16,17). Unlike reported experience with intraventricular administration of 131I-3F8, patients developed myelosuppression. Six of 7 patients demonstrated transient complete response with disappearance of cerebrospinal fluid lymphoblasts. No reports have been published on the use of RIT specifically in children, although a phase 1–2 trial at Memorial Sloan–Kettering Cancer Center examining the safety and efficacy of anti-CD33 (213Bi-HuM195) in patients with CD33-positive advanced myeloid malignancy is currently open to children. Moreover, the anti-CD33-calicheamicin immunoconjugate gemtuzumab ozogamicin has shown efficacy in children with relapsed acute myeloid leukemia (51). Another strategy targets the panhematopoietic CD45 antigen using anti-CD45 (131I-BC8) for the purpose of myeloablation instead of total body irradiation (12). A trial studying anti-CD45 (131I-BC8) containing a myeloablative conditioning regimen is currently open for pediatric patients at the Fred Hutchinson Cancer Research Center (Seattle, WA).
Non-Hodgkin’s Lymphoma
Although several radiolabeled antibodies are now available for RIT of adult non-Hodgkin’s lymphoma (NHL), no published reports have documented their use in children. The Children’s Oncology Group is currently recruiting children with relapsed CD20-positive B-NHL for a phase 1 study of 90Y-ibritumomab tiuxetan.
ONGOING TRIALS OF RADIOIMMUNOTHERAPY FOR PEDIATRIC TUMORS
There is an obvious need for more pediatric patients to be enrolled in RIT studies as well as for the development of studies designed specifically for children. In addition to the previously mentioned trials studying anti-CD33 (213Bi-HuM195) and anti-CD45 (131I-BC8) in acute leukemia, anti-CD20 (90Y-ibritumomab tiuxetan) in NHL, and 131I-8H9 for RID of pediatric solid tumors, 131I-3F8 has been incorporated into a therapeutic protocol for standard-risk medulloblastoma, in an effort to provide prophylaxis for the cranial spinal axis while reducing the dose and associated late effects of external beam radiation. A phase 1 study using intraventricular 131I-8H9 to provide targeted RIT to 8H9-positive solid tumors and brain tumors with leptomeningeal spread is also under way at Memorial Sloan–Kettering Cancer Center.
FUTURE OF RADIOIMMUNOTHERAPY FOR PEDIATRIC TUMORS
The FDA approval of 131I-tositumomab and 90Y-ibritumomab tiuxetan for adults with relapsed CD20-positive lymphoma has opened the door for investigative studies in children. However, given the differences in the biologic behavior of these agents in childhood B-NHL, careful efficacy and safety studies of these radiolabeled mAbs in phase 1–2 trials are necessary and have been initiated by the Children’s Oncology Group. The rapid development of other radiolabeled mAbs for hematologic malignancies in adults also has exciting implications for future therapy of pediatric leukemia and lymphoma. Approaches to developing new specific radioimmunoconjugates in pediatrics are essential to extend RIT to childhood solid tumors. Efforts at improving targeting while reducing toxicity are being investigated. Specifically for pediatric tumors, preclinical studies have demonstrated that anti-GD2 fusion protein single-chain Fv-streptavidin used in a pretargeting strategy with 111In or 90Y-DOTA-biotin can significantly augment tumor-to-nontumor ratios in NB xenograft models (52). The highly favorable microdosimetry of α-emitters, especially for minimal residual disease, is also being explored in these antibody systems, for both intravenous and intrathecal applications.
Acknowledgments
Preparation of this report was supported in part by the Leukemia Lymphoma Society, Hope Street Kids, and the Robert Steel Foundation.
Footnotes
Received May 4, 2004; revision accepted Aug. 13, 2004.
For correspondence or reprints contact: Shakeel Modak, MD, Department of Pediatrics, Memorial Sloan–Kettering Cancer Center, 1275 York Avenue, New York, NY 10021.
E-mail: modaks{at}mskcc.org
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.