


Abstract
The tracer 6-O-(2-18F-fluoroethyl)-6-O-desmethyldiprenorphine (18F-FDPN) provides enhanced flexibility to PET studies of the opioidergic system because the label has a longer half-life than the label of 11C-diprenorphine. Here we evaluated the ideal length of PET studies with 18F-FDPN. Methods: 18F-FDPN binding kinetics were quantified with protocols of different lengths by use of a 1-tissue or a 2-tissue compartment model for different volumes of interest. Furthermore, the effects of scanning duration were assessed by parametric analyses. Results: A 90-min protocol resulted in less than 10% bias in distribution volume (DV) relative to the full-length protocol. Correlation analyses of the DV estimates for the full-length protocol and the shortened protocols showed good replication of DV estimates for regions with both low and high levels of binding at schedules of up to 90 min. Conclusion: Data sampling in dynamic 18F-FDPN PET acquisitions should not be shorter than 90 min to maintain reliable estimates of DV.
The PET tracer 11C-diprenorphine is a nonspecific opioid receptor ligand suitable for in vivo assessment of the opioid receptor system (1–4). Compared with 11C-diprenorphine (half-life, 20.3 min), the 18F-labeled analog 6-O-(2-18F-fluoroethyl)-6-O-desmethyldiprenorphine (18F-FDPN; half-life, 109.7 min) developed at our institution (5) provides important methodologic advantages because of the longer half-life of the label. 18F-FDPN is applicable to alternative experimental designs, including single-bolus “ligand displacement” protocols. Compared with approaches involving 2 scans or bolus plus constant infusion, single-bolus investigations (6–8) allow measurement of endogenous opioid release on experimental challenge in 1 imaging session (9). Furthermore, 18F-FDPN can now be used at centers without an on-site cyclotron.
Recently, the kinetics of this compound were evaluated by use of various invasive modeling approaches (10). The analysis showed that a 2-tissue (2T) compartment model best characterizes the data obtained after a bolus injection of 18F-FDPN (120-min scanning protocol). Estimates of the distribution volume (DV) were robust across models, and compartment-model results showed a good correlation with results of the basis function method, thereby supporting the application of this method to pixel-based analyses. The applicability of the binding potential was questioned because of minimal binding in the (occipital) reference region (10,11).
The aim of this work was to determine the ideal length of an 18F-FDPN PET protocol after a bolus injection. Long protocols can provide increased parameter precision but are also subject to motion artifacts at late time points. On the other hand, shortened protocols may lead to biased parameters and increased uncertainty in parameter values but are tolerated better. An optimal scan length is a compromise between these 2 extremes, resulting in the shortest possible protocol that still accurately portrays 18F-FDPN binding.
MATERIALS AND METHODS
Experimental Protocol
Eight healthy male volunteers (age range, 33–40 y; mean age ± SD, 36.8 ± 2.9 y) were included. The research studies were approved by the ethics committee of medicine of Technische Universität München and the radiation protection authorities.
PET scans were acquired by use of an ECAT EXACT HR+ scanner (Siemens/CTI) in the 3-dimensional mode. A neck shield (NeuroShield; Scanwell Systems) was used to reduce random counting rates. Head fixation was accomplished with a polyurethane head mold, and obvious head movements were corrected manually by use of reference skin markers. The attenuation was corrected by transmission scanning. The data were reconstructed by filtered backprojection with a ramp filter (cutoff 0.3 cycle per projection element) into 63 image planes (128 ×128 pixel image matrix).
18F-FDPN was synthesized as published previously (5) and was obtained at a specific activity of >37 TBq/mmol. Each volunteer underwent a single 120-min scan in which 18F-FDPN was administered as a single bolus intravenous injection of 95.44 ± 9.58 MBq. On the basis of rodent brain uptake studies corrected for the weight differences between species and μ, δ, and κ expression in the brain (5), this dose corresponds to less than 0.2% occupancy of the opioid receptors present in the brain. Images were acquired over 120 min with the following frame durations (total of 46 frames): 12 frames of 10 s each, 3 frames of 20 s each, 7 frames of 1 min each, 4 frames of 2.5 min each, and 20 frames of 5 min each. Arterial blood samples were acquired throughout the scanning period as fast as possible for the first 2 min and then at increasingly spaced intervals (20 s–5 min). Arterial blood samples for metabolite quantification were taken at 5, 15, 30, 45, 60, 90, and 120 min. The amount of intact tracer as a function of time was determined as published previously (5) and was used to calculate the metabolite-corrected arterial input function (10).
Analysis and Statistical Evaluation
We quantified 18F-FDPN binding kinetics with protocols of different lengths for different volumes of interest (VOIs). Each subject’s dynamic PET dataset was realigned to a scan with a high signal-to-noise ratio by use of a 4th degree B-spline interpolation and resliced. Next, the dynamic volumes were normalized to a ligand-specific template (12). These preprocessing steps were performed by use of SPM2 software (Wellcome Department of Cognitive Neurology, London, U.K.). Regional VOIs defined by the MARSBAR toolbox (marsbar.sourceforge.net) included the amygdala, caudate, putamen, thalamus, cingulate, frontal, and occipital VOIs. The VOI extraction and kinetic analyses were performed by use of the PMOD Medical Imaging Program, version 2.5 (PMOD Group, Zurich, Switzerland), with the “VOI” and “KINETIC” tools, respectively. To evaluate the quantification of 18F-FDPN binding kinetics with protocols of different lengths, a 1-tissue (1T) or 2T compartment model was fit to the VOI data (13,14) with a measurement error variance defined to be equal to the average VOI concentration divided by the frame length (15,16). Parametric analyses also were performed at each protocol length by use of basis pursuit denoising (17,18).
The DV values for protocols of different lengths were assessed in terms of percent difference (Eq. 1), where DVexp is the DV determined from the shortened protocol and DVtrue is the DV estimated from the full-length protocol (120 min):
 Eq. 1
Eq. 1
Parametric maps of DV values were compared for the shortened protocols and the full-length protocol by use of a paired t test with the F test as output.
RESULTS
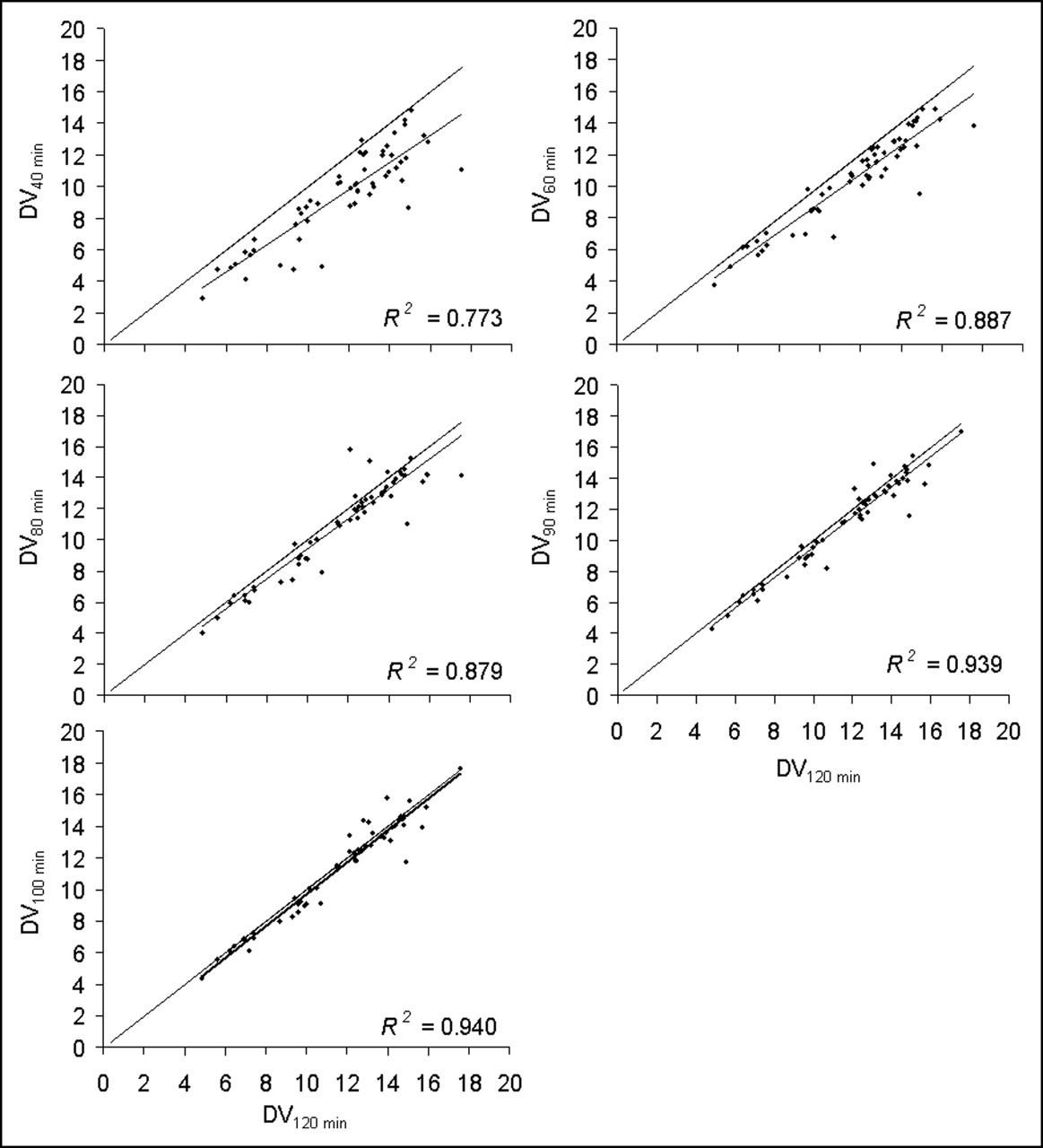
The VOI analysis resulted in less than 10% mean bias in DV values for protocols more than 90 min long (Fig. 1). The regional differences in DV illustrate that even an 80-min protocol resulted in less than 10% mean bias in all but very small regions, such as the amygdala. At 60 min, the small regions showed enhanced bias of up to 19%. The small regions showed greater variability in DV bias than did the larger regions. The variability in DV bias was consistent through 90 min but increased with shorter protocols. Correlation analyses of the DV estimates for the full-length acquisition protocol and the shortened acquisition protocols (Fig. 2) indicated that there was good replication of DV values for regions with both low and high levels of binding at shortened schedules of 100 and 90 min. At 80 min, the correlation was characterized by more variability and a trend toward more deviation in regions with high levels of binding than in regions with low levels of binding (Fig. 2). This trend was further augmented in the 60- and 40-min protocols, resulting in a substantial underestimation of DV values.

Mean absolute percent difference in DV values (VOI data). All values were compared against values from full-length (120-min) protocol. Regional VOIs included amygdala (♦), caudate (▪), cingulate (▴), frontal (•), occipital (□), putamen (⋄), and thalamus (○) VOIs.
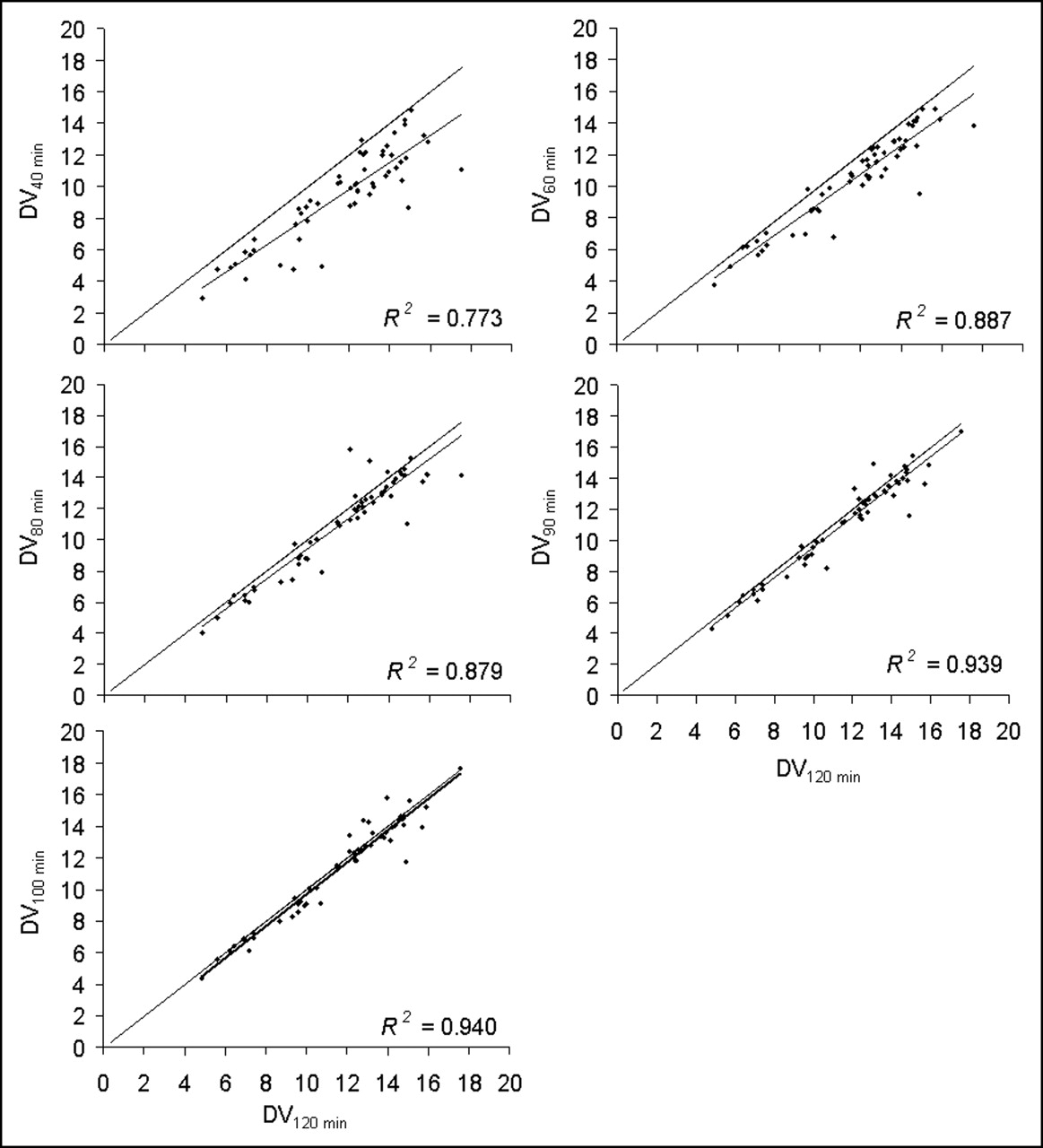
Correlations with dataset obtained with full-length (120-min) protocol. Long line is unity line (line where x equals y). Short line illustrates regression between DV values determined with shortened protocols and full-length (120-min) protocol.
Figure 3 shows the statistical evaluation at the voxel level for continuously shortened acquisition protocols (paired t test with F test as output; P < 0.001; extent threshold, 20 mm). The statistical comparisons with the 120-min protocol showed that various brain regions had statistically significant signal changes, with a clear trend toward increased differences with further shortening of the protocol. Only the 100-min protocol showed no significant statistical difference from the 120-min protocol. In the 90- and 80-min protocols, the differences were randomly distributed, with statistically significant differences predominantly in white matter, which is not expected to have 18F-FDPN binding.
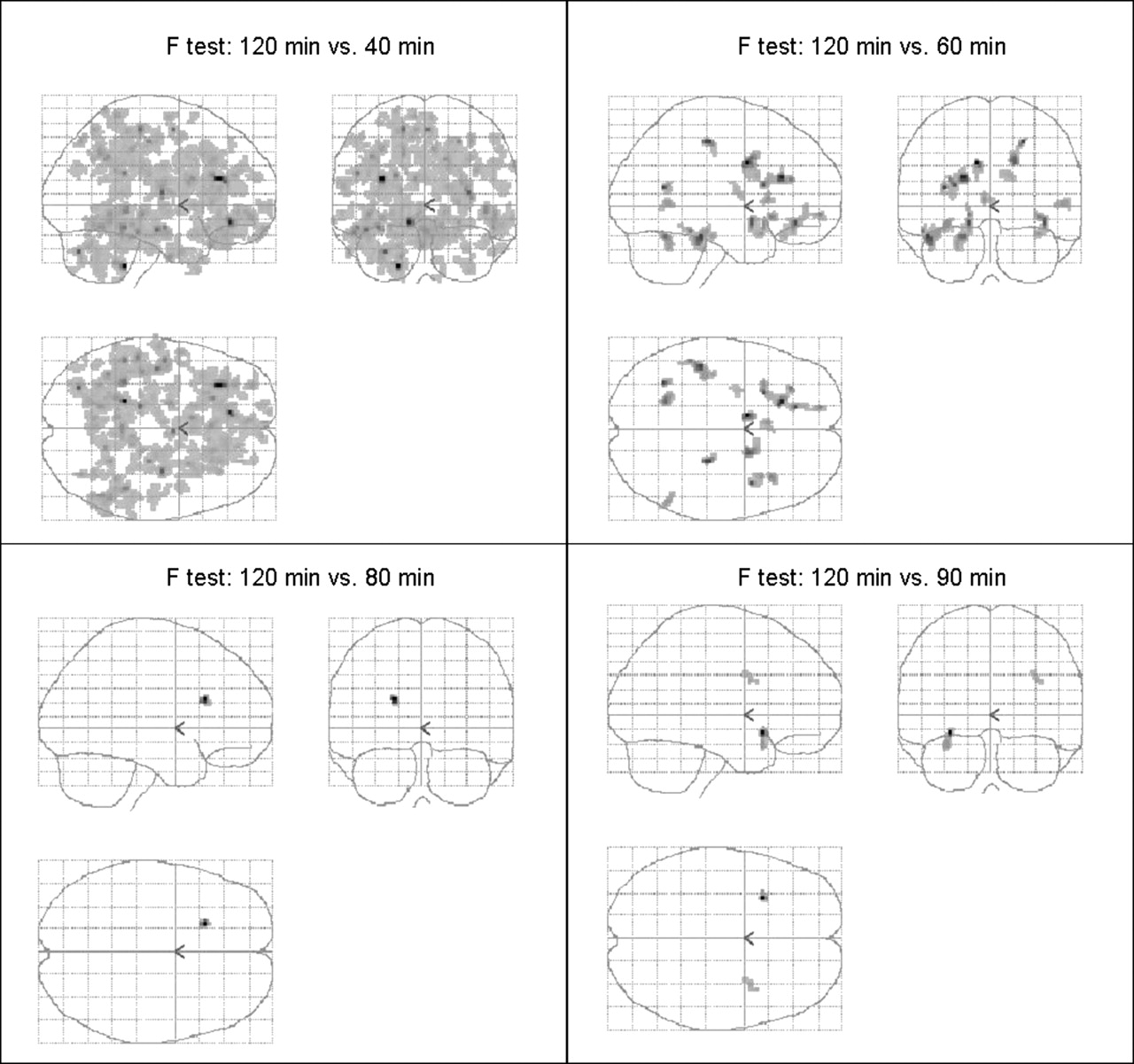
Areas of statistically different DV values in parametric analyses. All comparisons were made between shortened protocols and full-length (120-min) protocol. See text for details of comparisons. DV values across brain regions determined with 100 min of data (not shown) were not statistically different from those determined with 120 min of data.
As the protocol became shorter, it was necessary to reduce the model structure from a 2T model to a 1T model. Over 90% of the regions could be fit with a 2T model for protocols more than 80 min long. This value decreased to 80% with a protocol of 60 min, and 50% of all regions required a model reduction to adequately fit the data with a 40-min protocol.
DISCUSSION
PET with 18F-FDPN necessitates dynamic acquisitions with invasive blood and metabolite sampling because of the absence of a valid opioid receptor–free reference region (10,11). Our analysis of DV values attained by simulating acquisition times of variable lengths showed that a dynamic sampling period of 90 min yielded a robust estimation of DV values in all investigated brain regions (i.e., <10% deviation from data obtained with a 120-min acquisition). As shown in Figure 1, acquisition times of up to 60 min allowed the determination of DV values with approximately 10% bias in most brain regions. Although this approach is valuable when larger VOIs are investigated, our data suggest a considerable amount of uncertainty when DV values are estimated for very small brain regions, such as the amygdala or the ventral tegmental area, which are key areas in pain research of the opioidergic system. Theoretically, this estimation error may be improved by high-spatial-resolution scanners and online motion correction devices. As demonstrated by both VOI and voxel-based analyses (Figs. 1–3) of our data, protocols less than 60 min long should be avoided. We observed a generally negative bias with shorter sampling protocols (Fig. 2), illustrating the importance of the later data points for the estimation of DV values.
It was expected that a voxel-based analysis would be more sensitive to shortened protocols because of the increased noise at the individual voxel. It was encouraging to find that no significant differences from the dataset obtained with the full-length protocol were observed for the 100-min protocol and that those observed with the 90- and 80-min protocols were predominantly in white matter regions. These results support the use of parametric evaluations with these protocol lengths. Parametric analysis of protocols less than 80 min long may result in erroneous estimates of DV values in regions of potential interest. In these cases, it may be advisable to use a VOI analysis, which compromises some spatial information for improved signal-to-noise ratios in the data.
We reported a need to reduce the model structure from a 2T model to a 1T model as the protocol length was shortened. We therefore decided not to compare individual model parameter values but rather values for DV, which is a commonly calculated macroparameter that can be estimated from both model structures and thus can provide a metric for comparisons across all protocols. The reduction from a 2T model to a 1T model is warranted when there is inadequate information in the data to describe the second compartment. If the application of a 2T model is attempted when it is not supported by the data, unpredictable and erroneous DV values will be estimated. In these cases, it is better to use a 1T model in which the free and bound compartments are combined into a single compartment. Alternatively, the use of a 1T model when the data will support a 2T model will result in an underestimation of DV values because the data will not have been correctly quantified as a result of incorrect model assumptions. Although an underestimation of DV values also will occur with shorter sampling protocols, this result may not be attributable to the use of a 1T model (which may be appropriate given the data) but rather to a lack of information in the dataset. The rich dataset used in this study also could have been used to evaluate noninvasive methods from a modeling point of view. However, the importance of such an investigation warrants a dedicated and thorough study.
On the basis of this VOI and parametric evaluation, we propose an acquisition time of 90 min for dynamic 18F-FDPN PET studies. Compared with a 120-min acquisition (19,20), this shorter acquisition means a substantial improvement for human applications and should affect compliance and extent of movement artifacts. If, however, further shortening of the sampling time is required, such as in single-bolus challenge studies measuring DV before and after challenge in 1 scan, the investigator should be aware that the DV estimation will deteriorate in small regions. Therefore, a trade-off between accuracy and methodologic constraints must be considered in different studies.
CONCLUSION
The evaluation of 18F-FDPN distribution volumes with protocols of different lengths showed that a 90-min protocol resulted in less than 10% mean bias relative to the full-length protocol in all regions analyzed.
Acknowledgments
This study was supported by KKF grant 8764153.
Footnotes
Received Jun. 10, 2005; revision accepted Sep. 14, 2005.
For correspondence contact: Henning Boecker, MD, Nuklearmedizinische Klinik und Poliklinik, Klinikum Rechts der Isar, TU München, Ismaningerstrasse 22, D-81675 München, Germany.
E-mail: h.boecker{at}lrz.tu-muenchen.de
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.