


Abstract
99mTc-Labeled antimicrobial peptide ubiquicidin, 99mTc-UBI (29-41) in a freeze-dried kit, was evaluated as a bacterial infection–seeking agent in Staphlococcus aureus– and Escherichia coli–induced infections. Methods: Thirty-three rabbits were classified in 3 groups. Biodistribution of 99mTc-UBI (29-41) was studied in 3 animals (group I). Uptake of peptide was determined by counting radioactivity in anatomically fitted regions drawn over the liver, kidneys, urinary bladder, and whole body and expressed as the percentage uptake per organ. Experimental thigh muscle infection was induced by injecting 2 × 108 colony-forming units of live S. aureus or E. coli bacteria into the right thigh muscle in 20 rabbits (group II). Turpentine oil and formalin-killed S. aureus were used for inducing sterile thigh muscle inflammation in 10 rabbits (group III). On scintigrams, anatomically adjusted regions of interest were drawn over infected/inflamed (target) and noninfected/noninflamed (nontarget) thigh, and accumulation of 99mTc-UBI (29-41) at sites of infection/inflammation was expressed as a target-to-nontarget (T/NT) ratio. Results: A biodistribution study of 99mTc-UBI (29-41) revealed rapid removal of tracer from the circulation via the kidneys (10.6% ± 2.1% at 5 min and 5.9% ± 0.8% at 60 min) with accumulation of the major part in the urinary bladder within the first hour after injection (66.6% ± 7.2%). A significantly higher (P < 0.05) accumulation of 99mTc-UBI (29-41) was seen at sites of S. aureus–infected animals (T/NT ratio, 2.2 ± 0.5) compared with that of E. coli–infected animals (T/NT ratio, 1.7 ± 0.4). The maximum tracer accumulation was observed at 60 min after injection followed by a gradual decline. No significant accumulation was noticed in thighs of rabbits injected with either turpentine oil or killed S. aureus with markedly lower T/NT ratios (P < 0.05) compared with that of S. aureus– and E. coli–infected thighs. Conclusion: A 99mTc-UBI (29-41) freeze-dried kit can be used for differentiating infections with S. aureus and E. coli with significantly higher scintigraphic intensity (P < 0.05) compared with that of sterile inflammatory sites. The optimum time for infection imaging is 60 min after injection. Relatively low (T/NT) ratios were observed in E. coli infections compared with those of the S. aureus group, which may be due to a low virulence of the former; however, other possible reasons may include low affinity of this peptide for E. coli microbial membranes.
The medical community often faces the dilemma of discrimination between infection and inflammation. To achieve prophylactic cover, many consultants prescribe antibiotics blindly. There is a dire need for a specific technique to solve this problem. Currently available modalities such as CT and MRI give minute anatomic details but rely more on morphologic changes and are less accurate in early stages of infection. Scintigraphic detection of infection and inflammation allows determination of both the location and the number of infection and inflammatory foci throughout the body. Since scintigraphic images are based on functional tissue changes, these foci can be localized in their early phases, when anatomic changes are not yet apparent (1). However, there are many limitations in developing specific pharmaceuticals for clear differentiation between infection and inflammation. 67Ga-Citrate, being the most primitive radiotracer for this purpose, has a high sensitivity for both acute and chronic infections and noninfectious inflammation (2). There are disadvantages attributed to it, including its long physical half-life and high-energy γ-radiation. Many pharmaceuticals labeled with different radioisotopes have been used previously, but an ideal agent has not yet been found. Polyclonal and monoclonal immunoglobulins (3,4), liposomes labeled with 99mTc-hexamethylpropyleneamine oxime (99mTc-HMPAO) (5), and the avidin–biotin system (6) are nonspecific tracers with certain disadvantages. Antigranulocyte antibodies and antibody fragments, chemotactic peptides, cytokines, interleukins, and platelet factor-4 also have certain limitations. Cytokines and chemotactic peptides affect the immune system (7). Autologous leukocytes labeled with 111In are still considered the gold standard but require a sterile environment. Leukocytes labeled with 99mTc-HMPAO have the advantages of a low radiation burden to the patient and an ideal γ-energy; however, this agent is less stable than 111In-labeled leukocytes (8). Ciprofloxacin labeled with 99mTc has shown a high sensitivity and specificity for infection imaging (9). This antibiotic binds to the DNA gyrase enzyme of bacteria and has shown good accuracy in hip prosthesis infections (10). However, antibiotics face the problem of antibiotic-resistant bacteria, which is attributed to ciprofloxacin as well (11–14). Antimicrobial peptides, produced by phagocytes, epithelial cells, endothelial cells, and many other cell types, are an important component of innate immunity against infection by a variety of pathogens (15). These peptides show antibacterial, antiviral, and antifungal activities in vitro. Bacterial infections with Staphlococcus aureus and Klebsiella pneumoniae have been visualized in mice by 99mTc-labeled human neutrophil peptide-1 (16). The basis of the antimicrobial activity of these peptides is the interaction of the cationic domains with the negatively charged surface of the microorganisms. The antimicrobial peptide ubiquicidin UBI (29-41) (TGRAKRRMQYNRR; 1,693 Da) was originally isolated from mouse macrophage cells. This peptide is identical or highly homologous to S30, a protein that was purified from the small ribosomal subunit fraction of rat liver and shown to be present in various human and murine tissues (17). Later, an identical UBI was isolated from human airway epithelial cells. This peptide was labeled with 99mTc, which targeted bacterial cells but not sterile inflammatory processes in experimental animals (18). In later experiments, it also showed accumulation with high accuracy in fungal infections. This tracer was also used for detection of S. aureus infections in mice and K. pneumoniae in rabbits. As controls, inflammation was produced by lipopolysaccharides (LPS) and heat-killed microorganisms (19). Interactions of cationic peptides with bacterial envelopes involve insertion of the peptide into microbial membranes (20) and possibly a sequence-dependent interaction of the antimicrobial peptides with microorganisms (21).
In this study, we have used a 99mTc-labeled UBI (29-41) freeze-dried kit for detection of infection sites in rabbits injected with live S. aureus and Escherichia coli bacteria. As a control, inflammation was induced by formalin-killed bacteria and turpentine oil. Another difference from previous studies (18,19,22) is the use of a freeze-dried kit containing a greater quantity of UBI (29-41) with some modifications, such as preservatives and an enhanced constituted volume of the kit for easy injections to animals. Sodium borohydrate was used as the source of borohydrate ions instead of potassium borohydrate. A pyrophosphate lyophilized kit was used as the source of stannous ions instead of stannous pyrophosphate. The amount of peptide was regulated to obtain a reliable labeling efficiency with the lyophilized kit.
MATERIALS AND METHODS
Healthy, immunocompetent rabbits were obtained from a farmhouse. Ethical approval for the experiments and injection of 2 × 108 colony-forming units (cfu) of live bacteria was given by the Animal Ethics Committee of the Agriculture University, Faisalabad. Thirty-three animals, each weighing 1.2–1.6 kg (average, 1.4 kg), were divided into 3 groups: (a) Group I consisted of 3 rabbits to study the biodistribution of 99mTc-UBI (29-41). (b) Group II comprised 20 rabbits in which thigh muscle infection was induced experimentally; the rabbits were further categorized into 2 groups (IIa and IIb). In group IIa (n = 10) and group IIb (n = 10), infection was induced by using live S. aureus bacteria (American Type Culture Collection [ATCC] 25923) and live E. coli bacteria, respectively. (a) Group III comprised 10 rabbits in which sterile inflammation of the thigh muscle was induced. The rabbits were further categorized as animals having a thigh inflammation induced by killed S. aureus (group IIIa; n = 5) and those having a turpentine oil–induced thigh inflammation (group IIIb; n = 5), respectively.
Bacterial Strains
S. aureus ATCC 25923 is the most widely used quality control organism in clinical microbiology laboratories. Being a standard reference strain, its use was similar to that of previous studies. The E. coli bacterial strain was locally isolated and its pathogenicity was confirmed by an ileal loop ligation method in rabbits. This isolate, when biotyped, gave the 7-digit biochemical profile of 5154552.
Induction of Experimental Infection in Rabbits
Saline (0.3 mL) containing 2 × 108 cfu of viable S. aureus ATCC 25923 (group IIa) or E. coli (group IIb) was injected into the right thigh muscle followed by scintigraphy after 48 h, when significant swelling was visible at the injection site.
Induction of Inflammation in Rabbits
Sterile inflammation was induced by injecting saline (0.3 mL) containing 2 × 108 cfu of formalin-killed S. aureus (group IIIa) or turpentine oil (group IIIb) into the right thigh muscle of each animal. Imaging was performed after 48 h, when significant swelling was observed at the injection site.
99mTc-UBI Scintigraphy
Radiopharmaceutical.
99mTc-Pertechnetate was used to label antimicrobial peptide UBI (29-41), which was supplied by the Pakistan Institute of Nuclear Science and Technology (PINSTECH), Islamabad, in a freeze-dried kit formulation.
Kit Constituents.
Each vial of UBI (29-41) contained the following constituents or properties and was sealed under vacuum instead of nitrogen: (a) peptide, 400 μg dissolved in 10 μL 0.01 mol/L acetic acid; (b) stannous ions, 5.0 μL from the standard pyrophosphate kit; (c) borohydrate, 8.0 μL from the standard solution of 0.7 mg/mL sodium borohydrate in 0.1N NaOH; (d) activity, 0.5 mL (200 MBq/mL) 99mTc-pertechnetate fresh elute from the generator; (e) pH of the contents maintained at 6–7; and (f) storage at −5°C in the refrigerator.
Kit Preparation.
One-half milliliter of freshly eluted sodium pertechnetate (200 MBq/mL) was added to the vial with an insulin syringe. After incubation for 10–15 min, 0.9% saline was added to the vial to bring the constituted volume up to 2.0 mL. Two-tenth milliliter (10 MBq) of 99mTc-labeled peptide was withdrawn into the sterile syringe for injection to the animal. The kit was stored at room temperature and used within 6 h of reconstitution.
Kit Quality Control.
Free activity in the reconstituted kit was determined by using Whatman no. 3 filter paper as the stationary phase and acetone as the mobile phase. Hydrolyzed activity was determined by using instant thin-layer chromatography (ITLC-SG; Gelman Sciences) as the stationary phase and 85% ethanol at pH 3. Quality control on the high-performance liquid chromatography system was determined by using a gradient program as given in the Leiden University Protocol (Leiden, The Netherlands) with minor adjustments. The elution time for free technetium was 3.60 min and for the peptide was 12–16 min with peak splitting. The stability of labeled UBI was checked in the presence of various concentrations of cysteine in vitro, which showed an insignificant effect on the labeled compound.
Acquisition Protocol.
An E-Cam γ-camera (Siemens) equipped with a low-energy, all-purpose collimator was used for the acquisition. Data processing was done on the ICON 8.5 Macintosh system interfaced with the γ-camera.
Each animal was placed on a flat hard surface with both hind legs spread out and all 4 legs fixed with surgical tape. Diazepam (5.0 mg) was injected into the left thigh muscle. Saline (0.2 mL) containing 10 MBq (40 μg) of 99mTc-labeled peptide was then injected intravenously into the marginal ear vein. Immediately after injection, dynamic acquisition with both thighs in focus was done for 60 min (60 frames of 1 min each), followed by static images at 2, 3, and 4 h after injection (each for 3 min). For the biodistribution study of the radiopharmaceutical, whole-body acquisition was done at 5, 30, 60, and 120 min after injection.
Biodistribution of 99mTc-UBI (29-41) in Rabbits.
Total body counts were determined by drawing a region of interest (ROI) over the image of the entire animal. To determine the uptake (counts) of tracer in different organs, ROIs were drawn over the liver, both kidneys, and the urinary bladder in the images taken at 5, 30, 60, and 120 min. None of these animals passed urine during the time of study. The percentage uptake of injected activity by these organs at various time intervals was calculated as: percentage uptake by organ = (organ counts at a specific time/total body counts at that time) × 100.
Quantitative Analysis.
To determine the tracer accumulation in the infected/inflamed thigh, reference images (5, 30, and 60 min and 2, 3, and 4 h) were selected. On all reference images, an anatomically adjusted ROI was drawn over the right thigh region (target) and a mirror image region was created over the contralateral normal thigh area (nontarget). Accumulation of tracer at the site of infection or inflammation was expressed as the ratio of counts in the target muscle to the counts in the nontarget muscle (T/NT ratio).
Confirmation of Infection
Rabbits in the infection group showed focal thigh muscle swelling after injection of live S. aureus or E. coli and focal increased tracer accumulation, and infection was confirmed by culture of a fine-needle aspirate. The area was shaved with a razor and sterilized with pyodine solution. A sterile 5-mL disposable syringe with a 23-gauge needle was inserted deep into the swollen area and a sample was taken with a to-and-fro movement of the needle within the swelling. The aspirate was spread over blood agar and McConkey’s agar plates and incubated at 37°C for 24–48 h. After incubation, agar plates were observed for any growth of microorganisms. In the case of growth, a sample was taken, fixed on a slide, stained for gram-positive or gram-negative bacteria, and observed under a microscope for identification of microorganisms. The same process was repeated for rabbits in the inflammation group, in which formalin-killed S. aureus were used.
RESULTS
Paper Chromatography
Free technetium activity remained <1% and the overall labeling efficiency of the labeled peptide was found to be >95% in each case. These values remained unchanged up to 6 h after reconstitution of the kit.
Biodistribution of 99mTc-UBI (29-41)
The biodistribution of 99mTc-UBI (29-41) in various organs of the rabbit was determined scintigraphically. Kidneys displayed gradual excretion of the radiotracer, with mean percentage uptake values of 10.6% ± 2.1% and 4.2% ± 0.3% at 5 and 120 min after injection, respectively. The liver also showed a gradual decline in uptake values with the passage of time, with mean percentage uptake values of 6.6% ± 1.6% and 2.5% ± 0.8% at 5 and 120 min after injection, respectively. A rapid accumulation of radioactivity was visualized in the urinary bladder, with almost 80% of the injected tracer present at 120 min after injection.
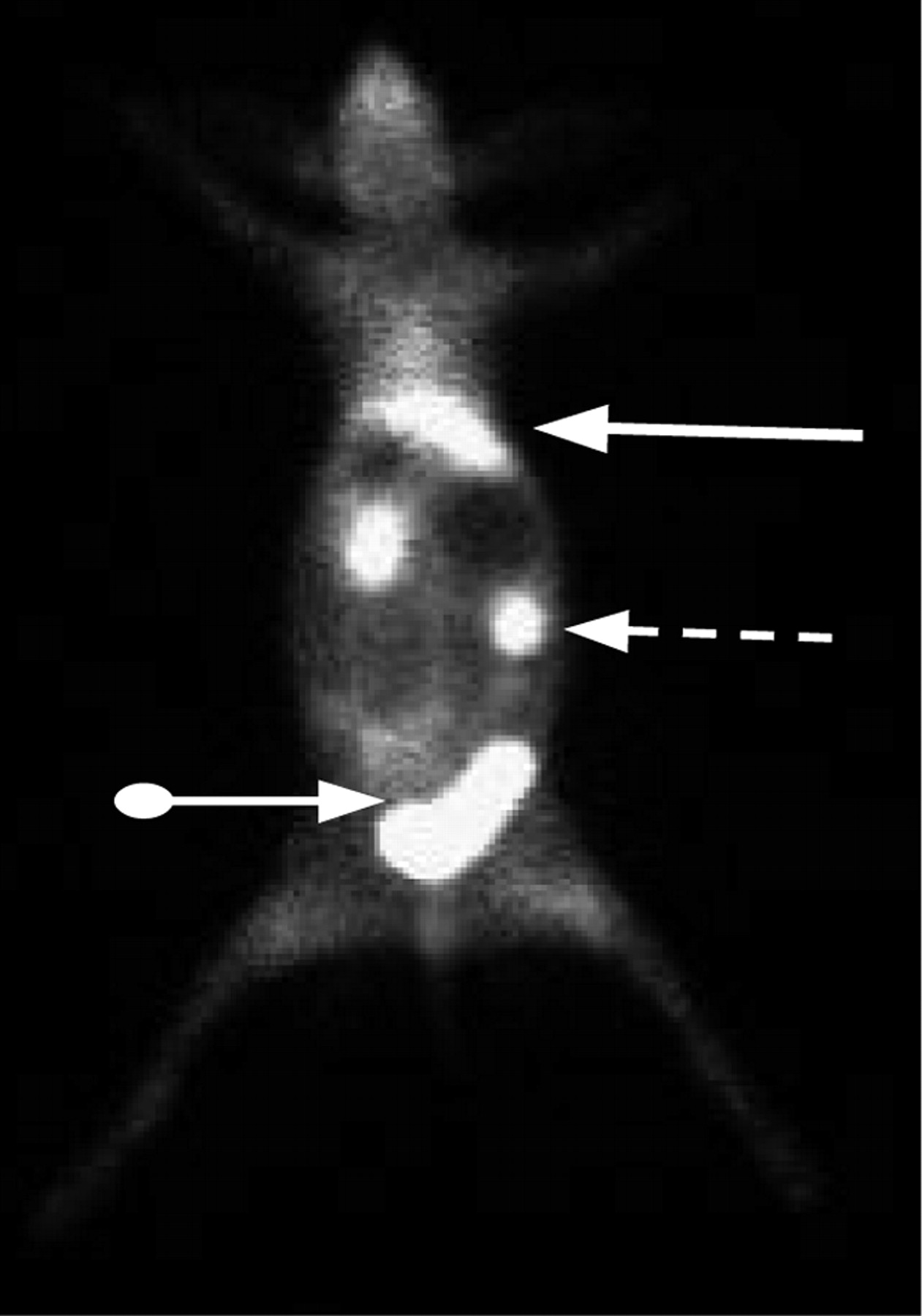
Values of 3 animals (3 data points; mean ± SD) are given in Table 1 and are graphically shown in Figure 1. Figure 2 shows the normal biodistribution of 99mTc-UBI (29-41) in a rabbit at 30 min after injection. The liver, both kidneys, and the urinary bladder are well outlined. The thyroid is not visualized, indicating good labeling efficiency of the kit.
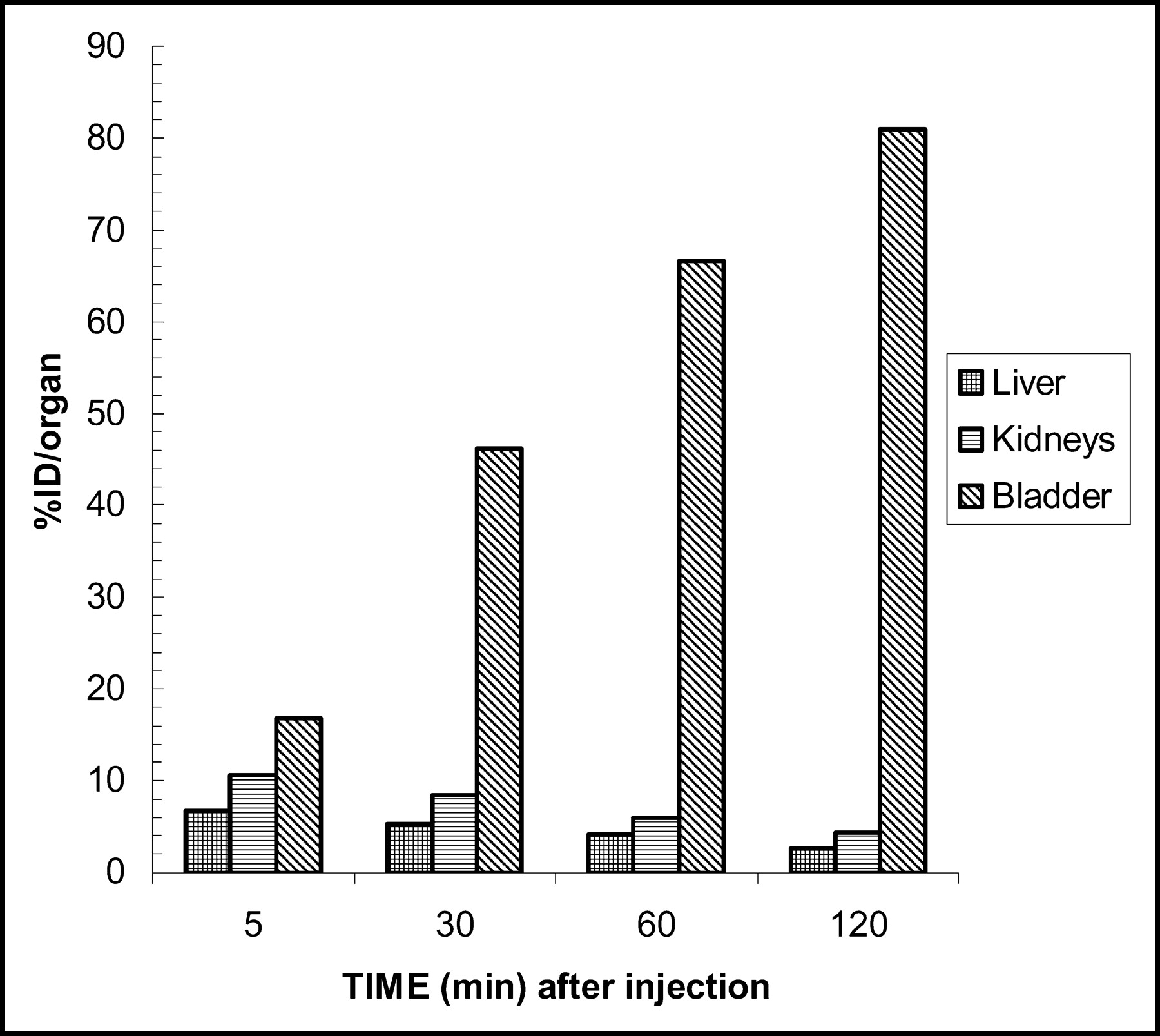
Scintigraphically determined biodistribution of UBI (29-41) in rabbits. %ID/organ = percentage injected dose per organ.

Biodistribution of 99mTc-UBI (29-41) in rabbit at 30 min after injection. Liver (solid arrow), kidney (dashed arrow), and urinary bladder (ball arrow) are well outlined.
Biodistribution of 99mTc-UBI (29-41) in Rabbits
Accumulation of 99mTc-UBI (29-41) at Site of Bacterial Infection
S. aureus and E. coli infections in rabbit thighs were visualized as areas of increased tracer accumulation within 5–30 min after injection of labeled peptide. T/NT ratios increased with the passage of time. The maximum mean T/NT for both S. aureus and E. coli was observed at 60 min after injection (Table 2). The highest T/NT ratio observed in 1 animal in the S. aureus–infected group was 3.56 at 60 min. E. coli–infected rabbits showed less accumulation of tracer compared with that of the S. aureus group, with a maximum T/NT ratio of 2.45 at 30 min in 1 animal.
T/NT Ratios of Infected Thigh Muscles in Rabbits
A statistically significant difference was found between S. aureus and E. coli T/NT ratios (P < 0.05) at 60 min after tracer injection. However, there was a minimal difference in the 2- and 3-h T/NT ratios.
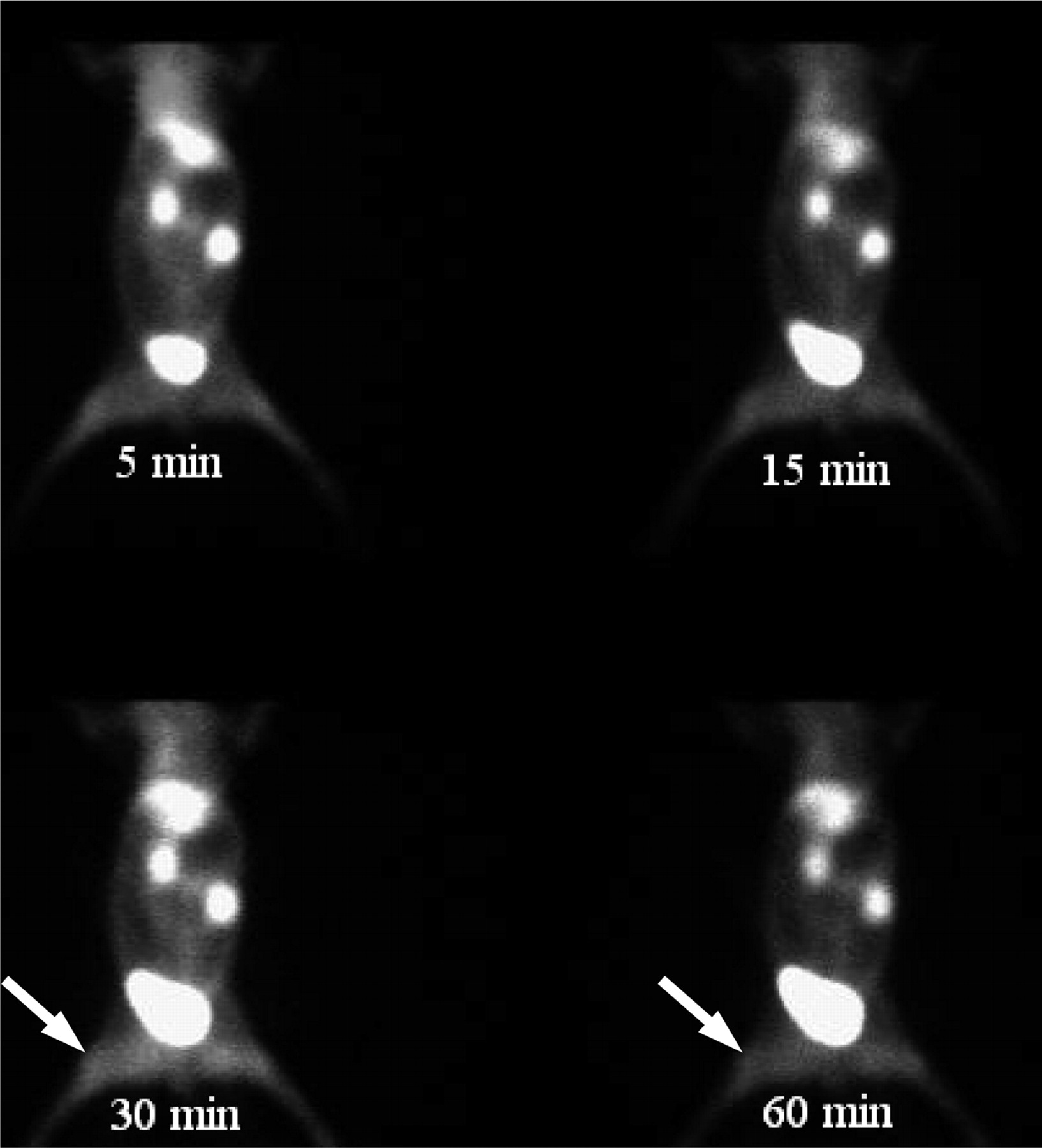
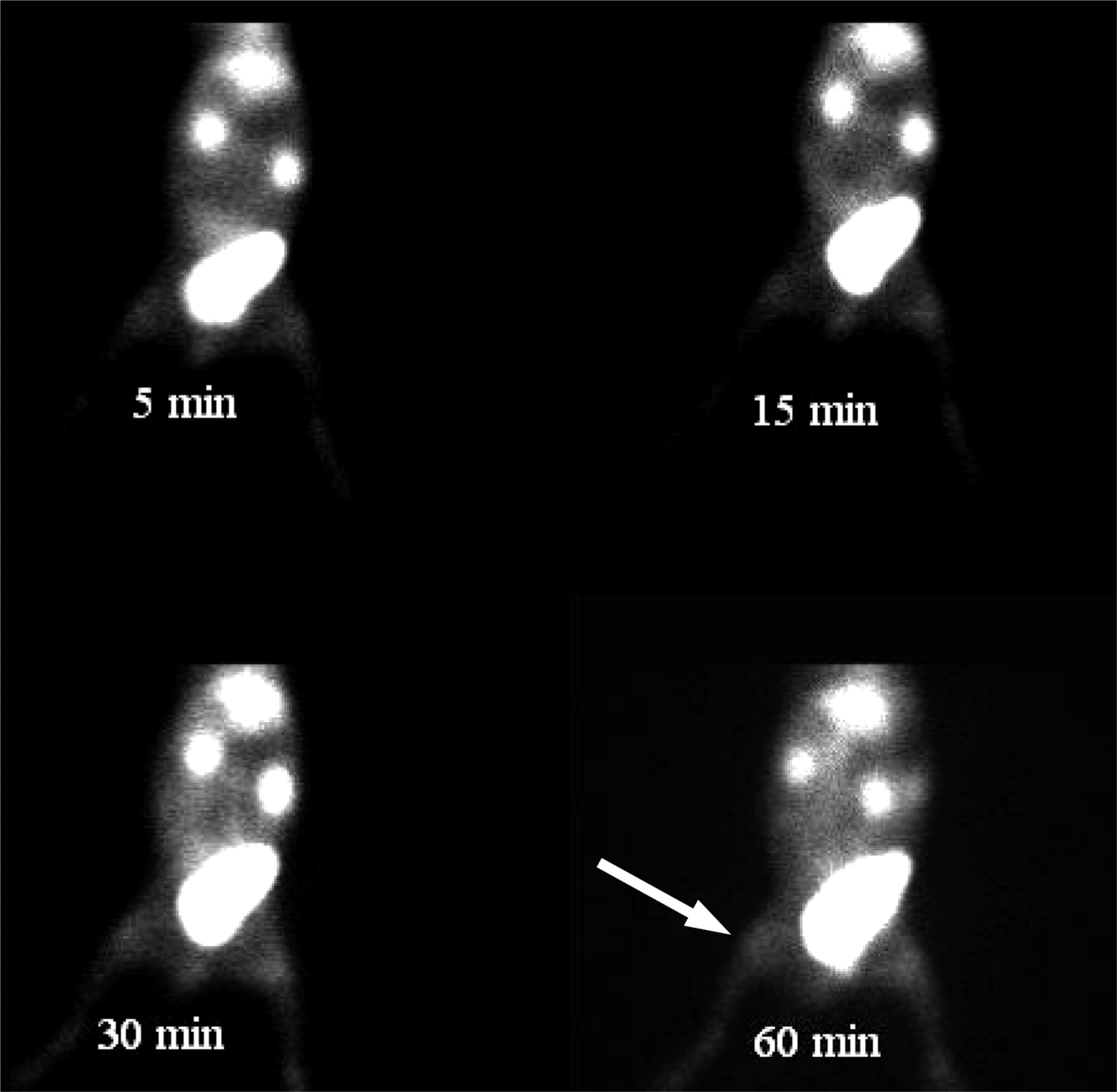
Figures 3 and 4 show increased focal tracer accumulation in S. aureus– and E. coli–infected lesions in rabbits. Cultures of aspirate taken from the site of infection were positive in all cases of the S. aureus and E. coli groups (growth of S. aureus and E. coli on blood agar and MacConkey’s agar).
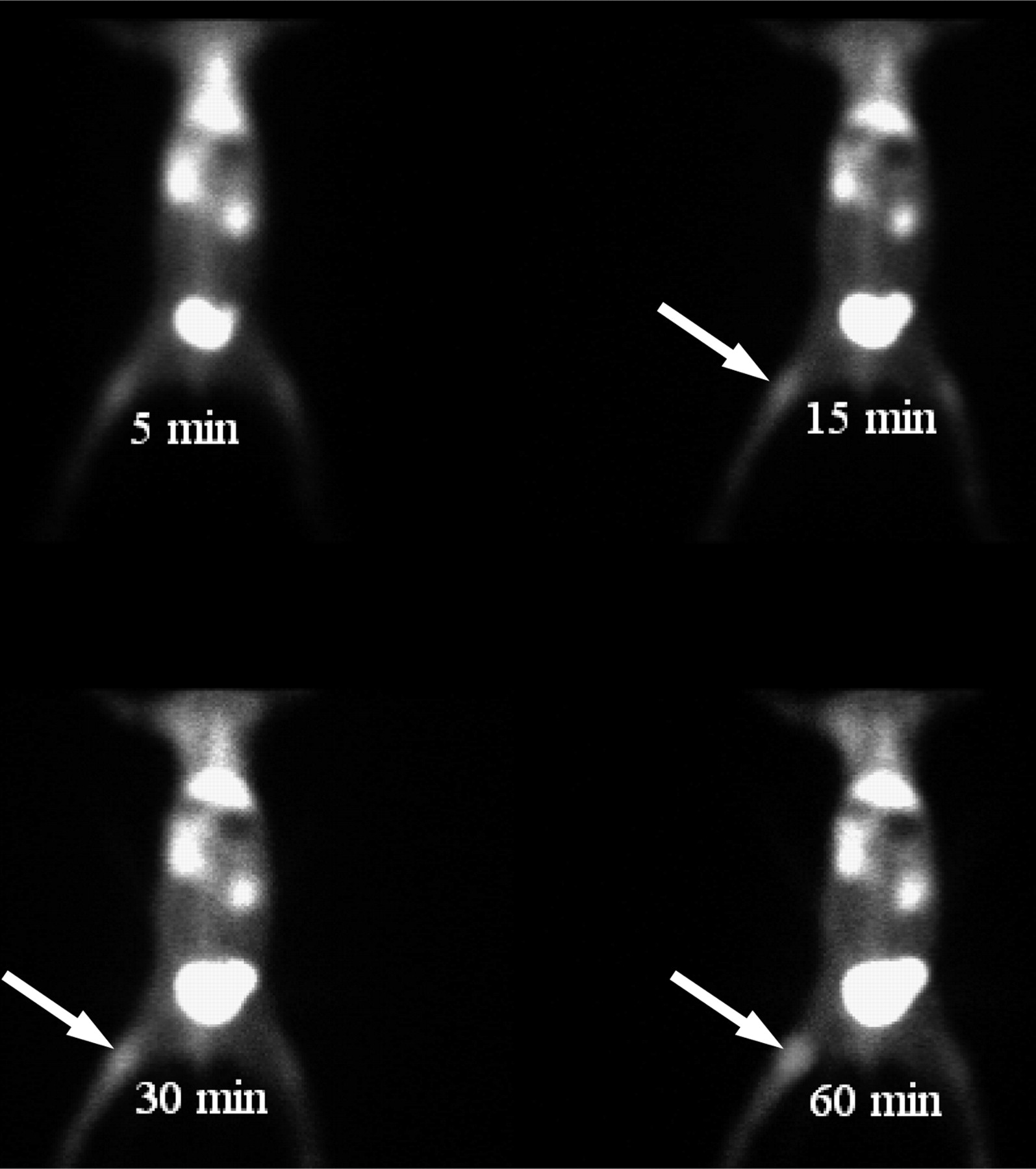
99mTc-UBI (29-41) scintigram of rabbit with S. aureus thigh muscle infection (arrow).
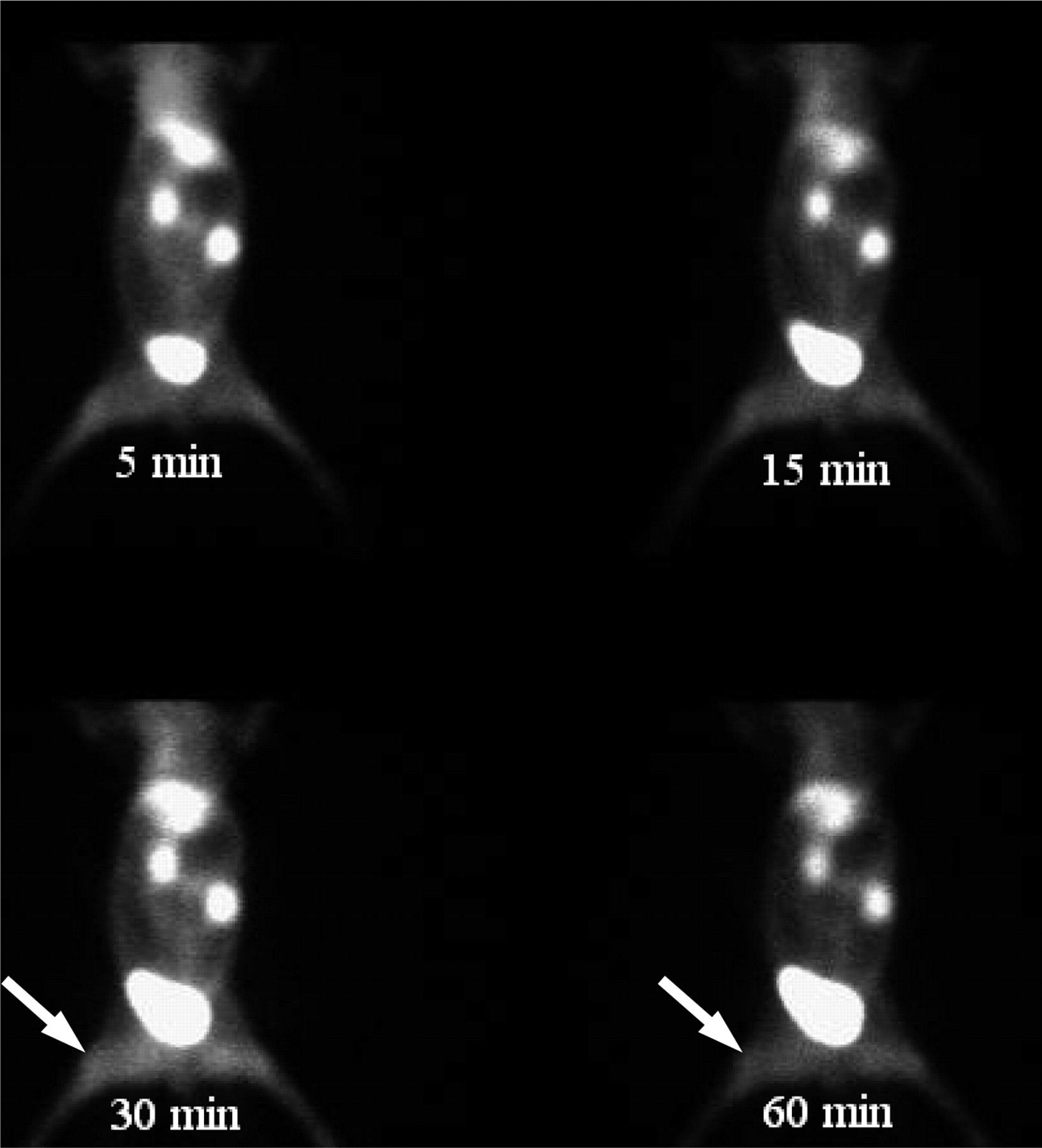
99mTc-UBI (29-41) scintigram of rabbit with E. coli thigh muscle infection (arrow).
Accumulation of 99mTc UBI (29-41) at Site of Sterile Inflammation
The uptake of 99mTc-UBI (29-41) was also studied in rabbits with sterile inflammation induced by turpentine oil and formalin-killed S. aureus. T/NT ratios given in Table 3 reveal an insignificant uptake of labeled peptide in sterile thigh muscle. T/NT ratios calculated in the case of inflammation induced by turpentine oil were 1.20 ± 0.14, 1.25 ± 0.08, 1.16 ± 0.15, and 1.03 ± 0.17 at 5, 30, 60, and 120 min after injection, respectively. These ratios are lower than the T/NT ratios of both S. aureus–and E. coli–infected animals. Similarly, lower T/NT ratios were observed in animals having formalin-killed S. aureus–induced inflammation compared with those of both bacterial infection models.
T/NT Ratios of Inflamed Thigh Muscles in Rabbits
Figure 5 shows a scintigram of a rabbit with a turpentine oil–induced thigh muscle inflammation (marked with arrow).
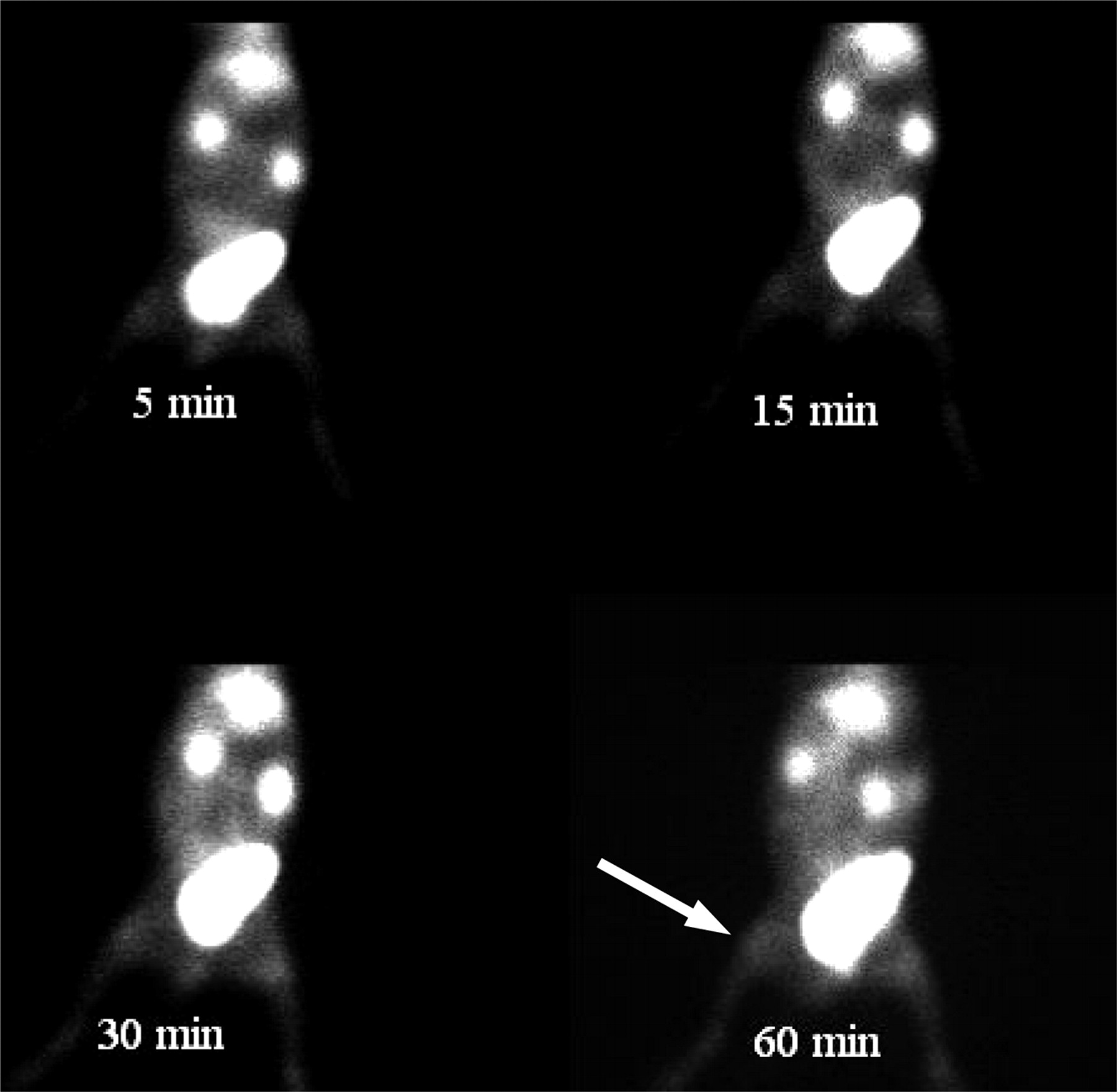
99mTc-UBI (29-41) scintigram of rabbit with turpentine oil–induced thigh muscle inflammation (arrow).
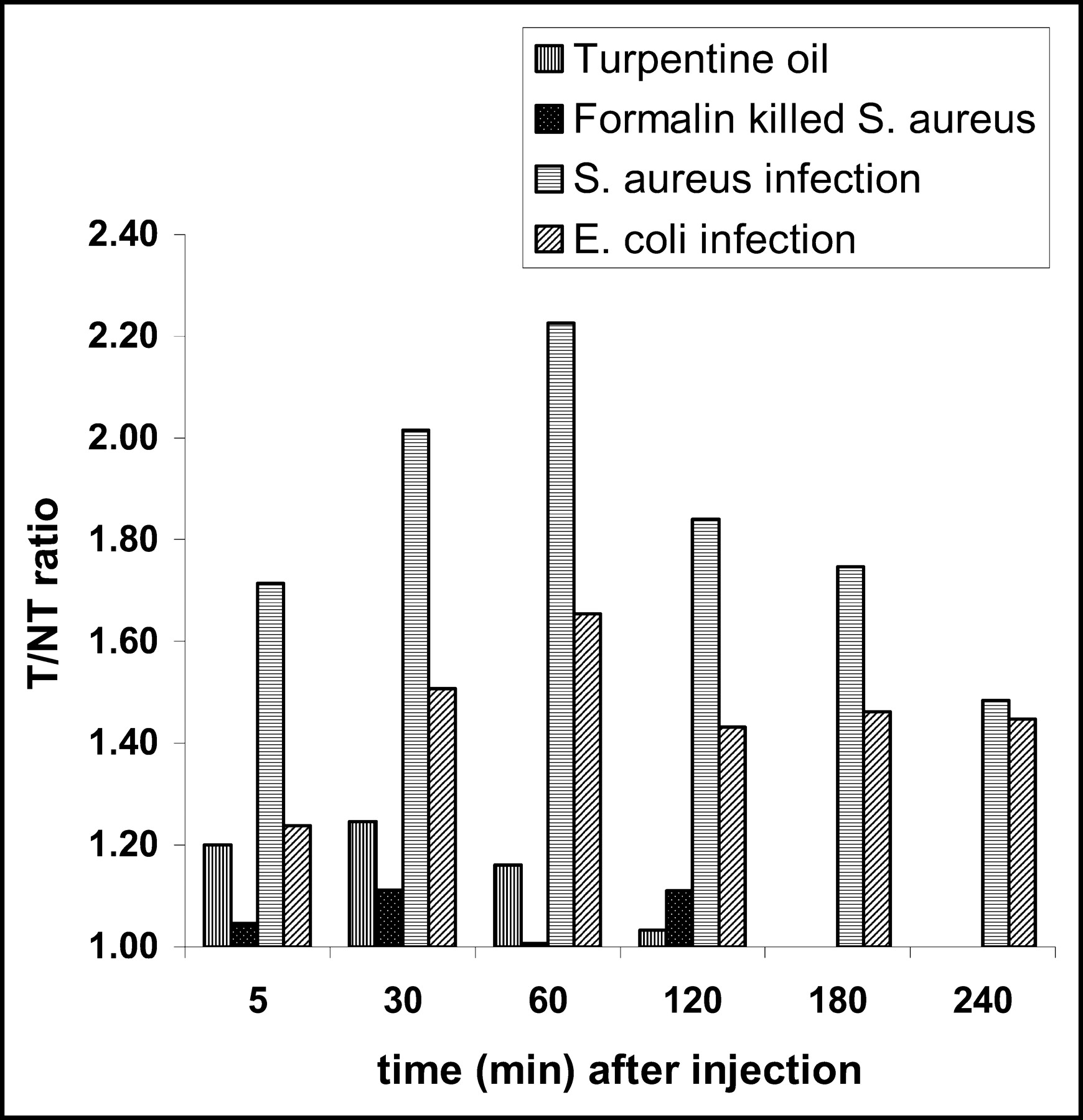
Figure 6 shows a comparison of all 4 inflammation/infection models of rabbits. Higher ratios were observed in the S. aureus group, with the maximum tracer uptake at 60 min, followed by the E. coli group. Significantly lower T/NT ratios were observed in the turpentine oil–induced inflammation group compared with those of the S. aureus and E. coli groups at 60 min after injection (P < 0.05). Similarly, a significant difference in T/NT ratios was found between the killed bacterially induced inflammation group compared with that of the live S. aureus group (P = 0.0003 at 60 min) and that of the E. coli group (P = 0.007 at 60 min).
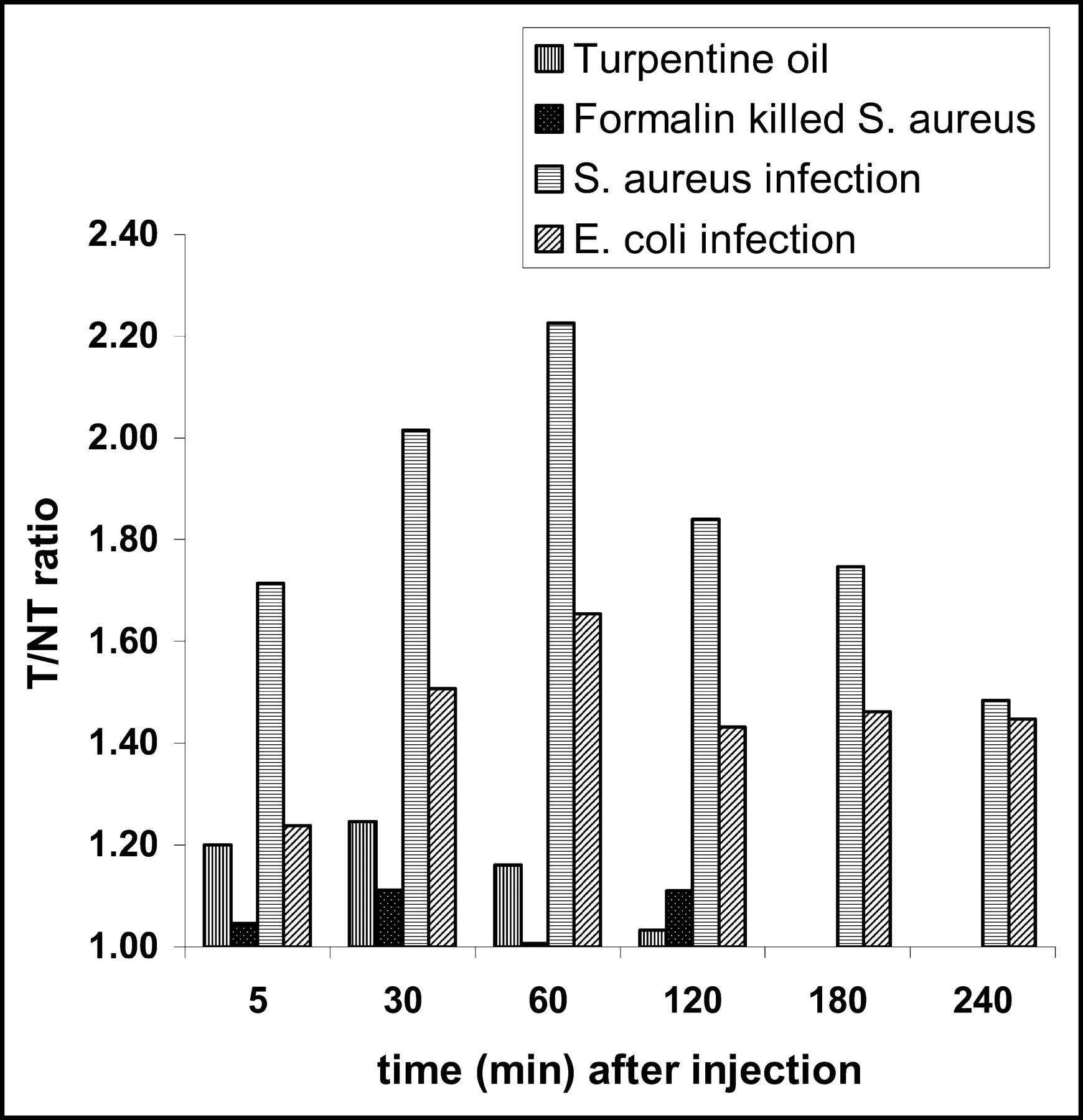
Accumulation of 99mTc-UBI (29-41) in rabbits with infected/inflamed thigh muscle. More accumulation is evident in the S. aureus group than in the E. coli group. Minimum uptake of tracer is noted in turpentine oil and killed S. aureus inflammatory groups.
In this study, we found that antimicrobial peptide UBI (29-41) detected infections with both gram-positive and gram-negative bacteria in rabbits as early as 5–30 min after injection; however, the maximum T/NT ratios were seen at 1 h after injection.
Side Effects
No anaphylactic reaction was observed with 99mTc-UBI (29-41) in all rabbits studied for biodistribution, infection, and inflammation scintigraphy. All animals tolerated the trauma of imaging and the acquisition procedure up to 4 h. No animal expired during acquisition protocol or 7 d after completion of the procedure.
DISCUSSION
99mTc-UBI (29-41) was used to differentiate between artificially induced infection and inflammation in rabbits. The aim of the radiolabeling technique is to firmly attach or incorporate the radionuclide into the peptide without altering its biologic functions, thus allowing reliable evaluation of its pharmacokinetics after intravenous administration. The direct labeling method of UBI (29-41) adopted at Leiden University Medical Centre was used in our study (18,23). This labeling method is a simple procedure in which the peptide is labeled in the absence of an external chelator. The reaction mechanism underlying this labeling of peptide has not been elucidated. It may involve the reduction of technetium, the production of a technetium intermediate, and the substitution reaction transferring the reduced technetium from this intermediate to the peptide (18). The same kit constituents in a freeze-dried kit were tried initially; however, the constituted volume used in previous studies (18,19,22) is too small to be removed even with a small-bore needle. Most of the labeled compound sticks to the glass vial and cannot be removed. Therefore, a freeze-dried kit with a higher concentration (400 μg) of UBI was prepared with a few modifications in the labeling procedure.
The classic method for studying the pharmacokinetics of small peptides in animals is to measure their levels in different organs at various intervals after injection using biochemical (or immunologic) assays. A major disadvantage of this approach is that it does not allow whole-body, real-time monitoring of the biodistribution of the peptide in an individual animal. To circumvent this drawback, scintigraphic techniques are used to quantify the amount of radiolabeled peptides in different organs at various intervals. The scintigraphic method is not ideal for biodistribution studies as one has to count radioactivity in individual organs after killing the animals at various time intervals (24). However, Welling et al. (18) have also made a comparison of the scintigraphically determined biodistribution of 99mTc-UBI (29-41) with ex vivo counting and found a good correlation of data obtained by ex vivo counting with values obtained by scintigraphy (R = 0.877; P < 0.001). A determination of the biodistribution of peptide in mice at 60 min, conducted at Leiden University, showed a higher uptake in the liver (14% ± 2%) and the kidneys (22% ± 2%) and a lower accumulation in the bladder (32% ± 5%) compared with the uptake in rabbits. Lupetti et al. (25) have also observed a similar pattern of biodistribution in mice.
In our study, the uptake of 99mTc-UBI (29-41) in various organs of the rabbit was determined by counting radioactivity in anatomically fitted regions drawn over the liver, kidneys, and urinary bladder and expressed as the mean percentage uptake (±SD) of injected activity in 3 rabbits. After injection, the peptide rapidly cleared from the circulation via the kidneys and accumulated in the urinary bladder. Scintigraphic analysis showed 66.6% ± 7.2% of tracer in urinary bladder after 1 h of injection. At 60 min, liver and kidneys revealed 4.1% ± 0.5% and 5.9% ± 0.8% uptake, respectively. Negligible accumulation was observed in the thyroid, bone marrow, spleen, and bowels. Our results are comparable with those obtained by Welling et al. (22). They used the same radiopharmaceutical to study its biodistribution in rabbits and observed that the percentage uptake of peptide in the kidneys and urinary bladder at 60 min after injection was 4% ± 1% and 65% ± 5%, respectively. They observed that the percentage uptake by the liver at 60 min was 5% ± 2%. A relatively lower uptake in the liver was observed in our study, indicating less colloid formation and the good quality of our kit.
S. aureus ATCC 25923 is a standard virulent strain widely used for quality control procedures. E. coli bacteria with the biochemical profile of 5154552 were locally isolated and their virulency was confirmed by an ileal loop ligation method. These microorganisms were injected into thigh muscles of rabbits to demonstrate the accumulation of 99mTc-UBI (29-41). Scintigraphy was performed from 5 min to 4 h after injection. Our results showed a gradual increase in the T/NT ratio, with peak values at 60 min. S. aureus–infected rabbits showed a higher T/NT ratio with a mean value of 2.2 ± 0.5 at 60 min. However, a significantly lower (P < 0.05) accumulation of this peptide was observed in E. coli–infected sites compared with that of S. aureus–infected lesions (mean value, 1.7 ± 0.4) at 60 min. Welling et al. (22) have shown a significant accumulation of 99mTc-UBI (29-41) in rabbits with experimental thigh muscle infection induced by 2 different types of S. aureus—that is, S. aureus ATCC 25923 and multidrug-resistant S. aureus. They found a mean T/NT ratio of 3.3 ± 0.2 in both cases and found similar results in mice. Furthermore, they obtained some evidence that accumulation of UBI (29-41) in infected areas is partially a receptor-mediated process. In rabbits infected with S. aureus, higher T/NT ratios were observed by these authors (3.3 ± 0.2) compared with our values (2.2 ± 0.5) at 60 min. This mismatch may be due to a lower virulence of microorganisms used in our experiment.
We induced nonspecific inflammation in 5 rabbits with turpentine oil. No significant accumulation of 99mTc-UBI (29-41) was observed at the injection site. The mean T/NT ratios in all animals were 1.2 ± 0.1, 1.2 ± 0.1, 1.2 ± 0.1, and 1.0 ± 0.2 at 5, 30, 60, and 120 min, respectively. In another group of 5 rabbits, nonspecific inflammation was induced by formalin-killed S. aureus. The mean T/NT ratios were 1.0 ± 0.1, 1.1 ± 0.4, 1.0 ± 0.3, and 1.1 ± 0.3 at 5, 30, 60, and 120 min, respectively. Welling et al. also studied the distribution of 99mTc-UBI peptide in rabbits with sterile inflammation; however, they used heat-killed bacteria and LPS as the inflammatory agent (18). Their results revealed insignificant accumulation of labeled peptide in sterile inflamed thigh muscles of mice and rabbits. The mean T/NT ratio was 1.2 ± 0.2. In another study, Welling et al. (22) found the same results in mice and rabbits in which LPS was used to induce sterile inflammation. Lupetti et al. (26) have also shown insignificant uptake of this radiotracer in mice with LPS–induced inflammation.
We compared the mean T/NT ratios of sterile inflammation–induced lesions and bacterially infected lesions. A significant difference (P < 0.05) was observed between the mean T/NT ratios of turpentine oil–induced lesions with both the S. aureus–and the E. coli–induced lesions. A similar difference (P < 0.05) was found between formalin-killed bacterially induced inflammation and both bacterially infected lesions. This indicates the capability of 99mTc-UBI scintigraphy to differentiate infection from sterile inflammation. Welling et al. (19) found a rapid detection of infection in rabbits and mice with a significantly higher scintigraphic intensity (P < 0.01) compared with that of sterile inflammatory sites.
Our results indicate that this radiolabeled peptide can detect bacterial infection in rabbits as early as 5–30 min after injection; however, maximum T/NT ratios were observed at 60 min. Relatively low T/NT ratios were demonstrated in E. coli–induced infection compared with those of the S. aureus–infected lesion, which may be due to a low virulence of the former. The pathogenicity of E. coli involves release of endotoxins after death of the microorganism inside the body of the host, which is the major difference from that of S. aureus. However, there could be other possible reasons for the selective accumulation of labeled peptides, which need to be elucidated in further studies.
CONCLUSION
99mTc-UBI (29-41) scintigraphy can be used for differentiating infection with S. aureus and E. coli with a significantly higher scintigraphic intensity (P < 0.05) compared with that of the sterile inflammatory site. The optimum time for imaging is 60 min after tracer injection. Relatively low T/NT ratios were observed in E. coli–induced infections compared with those of S. aureus–infected lesions, which may be due to a low virulence of E. coli used in our experiments. However, there may be other possible reasons for this significant difference as the mode of pathogenicity of the 2 microorganisms is different. This finding needs to be elucidated in further investigations.
Acknowledgments
The authors thank the staff of Punjab Institute of Nuclear Medicine (PINUM), particularly Muhammad Yousuf and Athar Khan, who worked hard during the performance of this study. This work was conducted at PINUM in collaboration with the Isotope Production Division of PINSTECH, Islamabad, Pakistan. The Department of Clinical Medicine and Surgery, Agriculture University, Faisalabad, and the Department of Clinical Pathology, Allied Hospital, Faisalabad, also contributed. UBI (29-41) was provided to PINSTECH through the International Atomic Energy Agency under grant CRP-11263.
Footnotes
Received Aug. 15, 2003; revision accepted Dec. 2, 2003.
For correspondence or reprints contact: Muhammad Saeed Akhtar, MBBS, MSc, Punjab Institute of Nuclear Medicine, P.O. Box 2019, Faisalabad, Pakistan.
E-mail: Saeed_pinum{at}yahoo.com.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Preclinical Evaluation of 68Ga-Labeled 1,4,7-Triazacyclononane-1,4,7-Triacetic Acid-Ubiquicidin as a Radioligand for PET Infection Imaging
- Microbial Targeting of 99mTc-Labeled Recombinant Human {beta}-Defensin-3 in an Animal Model of Infection: A Feasibility Pilot Study
- Leukocyte Receptor-Binding Radiopharmaceuticals for Infection and Inflammation Scintigraphy
- Antimicrobial Peptide 99mTc-Ubiquicidin 29-41 as Human Infection-Imaging Agent: Clinical Trial