


Article Figures & Data
Figures
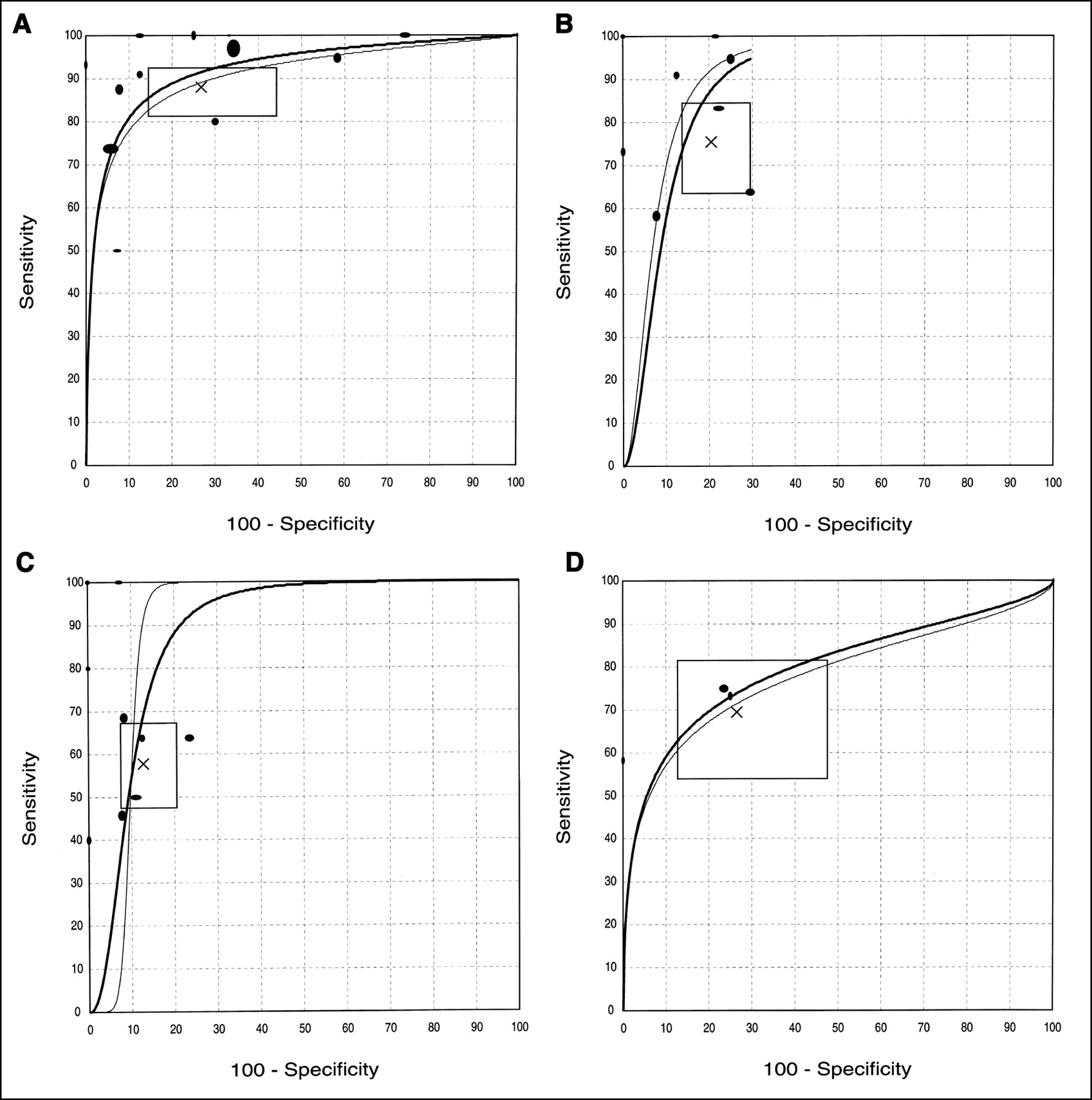
- FIGURE 1.
SROC curves for (A) qualitative visualization, (B) standard uptake value (cutoff, 2.0), (C) standard uptake value (cutoff, 3.0), and (D) metabolic rate of glucose (cutoff, 6.0 μmol/100 g/min). Curves show trade-off between true-positive rate (sensitivity) and false-positive rate (100 − specificity) across all pertinent studies. Each study is shown by eclipse with diameters approximately proportional to number of subjects evaluated for sensitivity (vertical dimension) and specificity (horizontal dimension) of study. Two SROC curves are shown based on weighted (bold line) and unweighted (thin line) calculations. SROC curves should be used for inferences of diagnostic accuracy preferably within range of sensitivity and specificity values of studies that are included in their calculations. X = random effects estimates of sensitivity and specificity; horizontal and vertical dimensions of rectangle = corresponding 95% confidence intervals.

Tables
Study Mean age (range) Patients with STL Evaluable patients* (lesions) Malignant (%) Inclusion/exclusion criteria Primary/recurrent Design Schwarzbach 2000 54 (16–78) 50 47 (56) 35 (63) Consecutive patients suspected of STS from clinical symptoms and MRI or CT 19/37 Prospective Watanabe 2000 47 (12–77) 37 37 (37) 7 (19) Patients referred for STM evaluation after CT, MRI, or angiography 33/4 Unclear Griffeth 1992 50 (16–84) 21 19 (20) 10 (50) Patients referred for STM evaluation after CT or MRI 10/10? Unclear Schulte 1999 49 (1–89) 102 102 (102) 66 (65) Patients with STL suggestive of benign or malignant tumor on US or MRI 88/14 Prospective Lucas 1999 51 (6–85) 30 30 (31) 19 (61) Consecutive patients with suspected STS from clinical symptoms and MRI 31/0 Unclear Nieweg 1996 50 (18–82) 22 22 (22) 18 (82) Patients suspected of STS from clinical findings 22/0 Prospective Hain 1999 39 (11–81) 16 16 (16) 2 (13) Patients after amputation for STS, evaluated for recurrence 0/16 Retrospective Kern 1988 30 (12–63) 4 4 (4) 3 (75) Patients referred with STM 4/0 Unclear Lucas 1998 51 (3–84) 62 62 (72) 19 (26) STS patients evaluated for local recurrence 0/72 Retrospective Lodge 1999 50 (18–76) 29 29 (29) 12 (41) STM suspected to be malignant based on clinical examination and MRI 29/0 Prospective van Ginkel 1996 49 (18–80) 20 7 (7) 7 (100) Patients with biopsy-proven recurrent STS, assessed before HILP therapy 0/7 Prospective Kole 1997 54 (32–83) 17 17 (17) 15 (88) Patients with proven or suspected local recurrence of STS 0/17 Prospective Ferner 2000 26 (12–62) 15 15 (19) 5 (26) Patients with neurofibromatosis with symptomatic visible neurofibromas 19/0 Unclear Adler 1990 ND (41–85) 5 5 (5) 5 (100) Patients with liposarcoma of the thigh 5/0 Prospective? Jones 1996 54 (46–65) 4 4 (4) 4 (100) Histologically confirmed STS with planned radiotherapy/hyperthermia 4/0 Unclear ↵* In Schwarzbach et al. (2000), 3 patients were excluded because of no biopsy or technical failure; in Griffeth et al. (1992), 2 patients were excluded because of no diagnostic documentation or follow-up; in van Ginkel et al. (1996), 20 patients with STS were assessed, but those with primary lesions overlapped with patients included in Nieweg et al. (1996). Thus, only the 7 recurrent lesions were considered in all analyses and are listed in table.
STL = soft-tissue lesion; STM = soft-tissue mass; US = ultrasound; HILP = hyperthermic isolated limb perfusion; ND = no data.
Whenever both soft-tissue lesions and other lesions were included (Watanabe, Kern, Ferner, Jones), only data on soft-tissue lesions are presented in table. Median age is provided in Schwarzbach et al. (2000) and in Schulte et al. (1999).
Study 18F-FDG dose (MBq) Measures Reference standard Potential verification bias Schwarzbach 2000 370–440 Visualization, SUV Biopsy, except for 7 patients followed clinically and radiologically for 4–27 mo Limited Watanabe 2000 185–350 Visualization, SUV Biopsy, surgical excision or postmortem, except for 1 patient (clinical and radiologic criteria) Very limited Griffeth 1992 370 Visualization (TBR), SUV Biopsy or surgical excision, except for 1 patient (clinical and radiologic criteria) Very limited Schulte 1999 120–300 Visualization (TBR) Excisional, incisional, or needle biopsy followed by surgical resection when indicated No Lucas 1999 350 Visualization, SUV Open biopsy, followed by surgical excision when appropriate No Nieweg 1996 187–407 Visualization, SUV, MRG Biopsy (no details) No Hain 1999 320 Visualization Unclear, presumably biopsy performed only when indicated Considerable Kern 1988 185 Visualization, MRG Biopsy and tumor resection No Lucas 1998 350 Visualization Biopsy (and operative diagnosis), when PET or MRI suggested recurrence, otherwise clinical and imaging follow-up Considerable Lodge 1999 350 SUV (at 60, 120, 255 min),* MRG Biopsy followed by appropriate surgical excision No Van Ginkel 1996 370 Visualization, MRG Biopsy of irresectable tumors No Kole 1997 370 Visualization, MRG Biopsy (no details) No Ferner 2000 350 Visualization, SUV Biopsy, except for 9 patients assessed clinically and radiologically Considerable Adler 1990 148–278 Visualization (TBR), SUV Biopsy presumably (no details) No? Jones 1996 370 Visualization, SUV Needle or incisional biopsy followed by surgical resection No ↵* SUV data at 60 min are used in quantitative synthesis.
- TABLE 3
Summary Diagnostic Performance of 18F-FDG PET for Diagnosing Malignant vs. Benign Soft-Tissue Lesions
Diagnostic parameter Case series (subjects) Independent estimates (95% CI)* Typical SROC estimates (sensitivity, specificity)† Sensitivity Specificity Unweighted Weighted Qualitative visualization 13 (398) 88% (81–93) 73% (56–86) (90%, 73%) (92%, 73%) Primary lesions 7 (231) 95% (89–98) 59% (38–78) (95%, 59%) (96%, 59%) Recurrent lesions 5 (146) 81% (69–89) 91% (81–96) (74%, 91%) (81%, 91%) SUV ≥ 2.0 10 (208) 76% (64–85) 79% (71–86) (92%, 79%) (87%, 92%) Primary lesions 7 (157) 79% (67–88) 77% (67–85) (93%, 77%) (91%, 77%) Recurrent lesions 3 (51) 63% (44–78) 91% (71–98) (70%, 91%) (72%, 91%) SUV ≥ 3.0 10 (208) 58% (48–67) 87% (79–92) (90%, 87%) (70%, 87%) Primary lesions 7 (157) 60% (48–72) 86% (77–92) (82%, 86%) (66%, 86%) Recurrent lesions 3 (51) 52% (35–69) 91% (71–98) (62%, 91%) (62%, 91%) MRG ≥ 6.0 μmol/100 g/min 4 (66) 70% (54–82) 73% (53–87) (72%, 73%) (74%, 73%) Primary lesions 3 (52) 75% (57–87) 72% (50–87) (76%, 72%) (76%, 72%) Recurrent lesions 1 (14) 58% (29–83) 100% (16–100) NE NE
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Comparison of [68Ga]Ga-Fibroblast Activation Protein Inhibitor-04 and [18F]FDG PET Imaging for Solitary Fibrous Tumor and Preliminary Application of FAP-Targeted Radiopharmaceutical Therapy
- Diagnostic Accuracy of 68Ga-FAPI Versus 18F-FDG PET in Patients with Various Malignancies
- 68Ga-FAPI as a Diagnostic Tool in Sarcoma: Data from the 68Ga-FAPI PET Prospective Observational Trial
- Simulation of Tracer Dose Reduction in 18F-FDG PET/MRI: Effects on Oncologic Reading, Image Quality, and Artifacts
- Imaging in Sarcoma
- Correlation Between Glycolytic Phenotype and Tumor Grade in Soft-Tissue Sarcomas by 18F-FDG PET
- Contemporary Imaging in Sarcoma
- 11C-Methionine vs. 18F-FDG PET in Soft Tissue Sarcoma Patients Treated with Neoadjuvant Therapy: Preliminary Results
- Imaging Bone and Soft Tissue Tumors with the Proliferation Marker [18F]Fluorodeoxythymidine
- 18F-FDG PET for Evaluation of Bone Marrow Infiltration in Staging of Lymphoma: A Meta-Analysis
- Detection and Grading of Soft Tissue Sarcomas of the Extremities with 18F-3'-Fluoro-3'-Deoxy-L-Thymidine