


Abstract
It has been reported that lipiodol solution of 188Re-labeled 2,2,9,9-tetramethyl-4,7-diaza-1,10-decanedithiol (TDD), an N2S2 derivative, shows excellent targeting of liver cancer after transhepatic arterial embolization (TAE). However, its tumor retention is not high enough to treat liver cancer. Therefore, a new form of TDD, 4-hexadecyl-TDD (HDD), was developed to improve tumor retention by introducing a long alkyl chain. In this study, we compared the tumor retention properties of 188Re-HDD/lipiodol and 188Re-TDD/lipiodol, using a rabbit liver cancer model, and performed dosimetry using the results. Methods: The VX2 cancer cell line was implanted into the livers of 7 rabbits. TAE was performed on 3 rabbits with 188Re-TDD/lipiodol and on 4 rabbits with 188Re-HDD/lipiodol, and conjugated anterior and posterior planar scans were obtained at 1, 2, 6, 24, and 48 h after TAE. From these images, tumor retention was calculated and compared between 188Re-TDD and 188Re-HDD. Afterward, the required dose of radioactivity and the radiation dosimetry for exposure of major organs were calculated using MIRDOSE3.1 software. Results: The residence times of radioactivity in the liver were 10.2 ± 1.0 h in the 188Re-TDD group and 17.6 ± 0.8 h in the 188Re-HDD group (P = 0.034). The required radioactivity for 100 Gy of irradiation to 2.64- to 5.27-cm tumors was 142–1,070 MBq of 188Re-HDD in the rabbit model. The radiation exposures for the major organs were within the tolerable range, and the S-value for the whole body (effective dose equivalent) was calculated to be 0.209 mSv/MBq. Conclusion: Introduction of a long alkyl chain significantly improved the tumor retention of 188Re-HDD/lipiodol, compared with that of 188Re-TDD/lipiodol. Moreover, the required radioactivity for humans and the radiation exposure were within the feasible range for clinical application.
- 188Re-labeled 4-hexadecyl-2,2,9,9-tetramethyl-4,7-diaza-1,10-decanedithiol
- liver cancer
- lipiodol
- transarterial embolization
Liver cancer is one of the most common malignancies in the world and causes about 1 million deaths annually. The disease is most prevalent in Asia, which has the largest population on the earth. In addition, colon cancer is the second most common cause of cancer death in the West, and the majority of the patients die from liver metastases (1,2).
More than 85% of liver cancer cases are inoperable because of late diagnosis. In cases of inoperable primary or metastatic liver cancer, transhepatic arterial embolization (TAE) is the most important therapy (3). In TAE, hepatic tumor-feeding arteries are embolized under angiographic guidance, and blood supply to the tumor is cut off. To enhance the effect of TAE, some adjunctive therapies using radioisotopes or chemotherapeutic agents have been investigated. Several β-emitters, such as 166Ho, 90Y, 131I, 186Re, and 188Re, have been reported to be possible candidates for TAE (4–8). Among the reported radioisotopes, 188Re has several outstanding physical properties for clinical use. It has a half-life of 17 h and emits a 2.1-MeV β-ray. The coemission of a 155-keV γ-ray enables adequate imaging and monitoring of therapeutic efficacy. Moreover, because 188Re can be produced from the 188W/188Re-generator system, it offers practical clinical availability for routine application and eminent economic advantage.
Lipiodol, an iodinated and esterified lipid of poppy seed oil, was initially developed for use as a radiocontrast agent (9) and is currently used as a common embolizing agent for TAE because of high viscosity. Because hepatic tumors have a highly tortuous microvasculature, they retain viscous lipiodol. 131I-labeled lipiodol has been investigated as a radioembolizing material (8,10–12) and is commercially available. Although 131I-labeled lipiodol has been clinically effective, it has some shortcomings, including high-energy γ-ray emission, long half-life, and high cost. 188Re-labeled lipiodol has been determined to have physical advantages over 131I. The typical approach for labeling lipiodol with 188Re is through use of a bifunctional chelating agent. However, the approach has not been very effective because of the chemical incompatibility between 188Re and lipiodol (13).
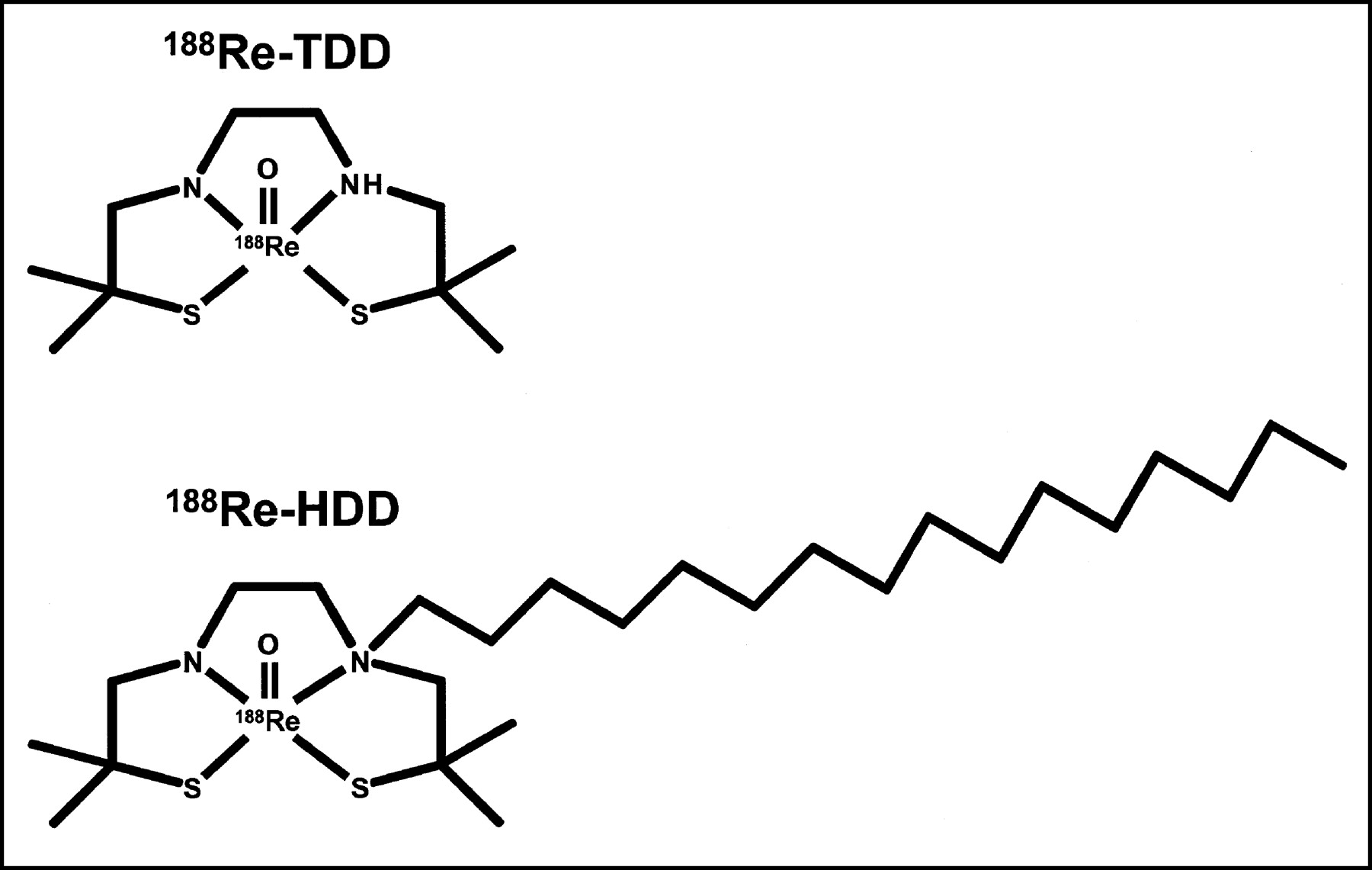
Recently, a new method bypassing the difficult labeling process was reported (14). This method involved the use of 2,2,9,9-tetramethyl-4,7-diaza-1,10-decanedithiol (TDD) labeled with 188Re (Fig. 1). TDD is an N2S2 or a diaminedithiol derivative and is known to form a stable lipophilic chelate with rhenium or technetium. It can make a stable lipophilic solution with lipiodol because of high lipophilicity. However, tumor retention of 188Re-TDD/lipiodol solution is not satisfactory despite high accumulation in tumors after arterial administration. Consequently, a new agent, 4-hexadecyl-TDD (HDD), has been synthesized (Fig. 1) to improve tumor retention (15). HDD, a derivative of TDD, contains a pendant alkyl hexadecyl group and has significantly increased lipophilicity.
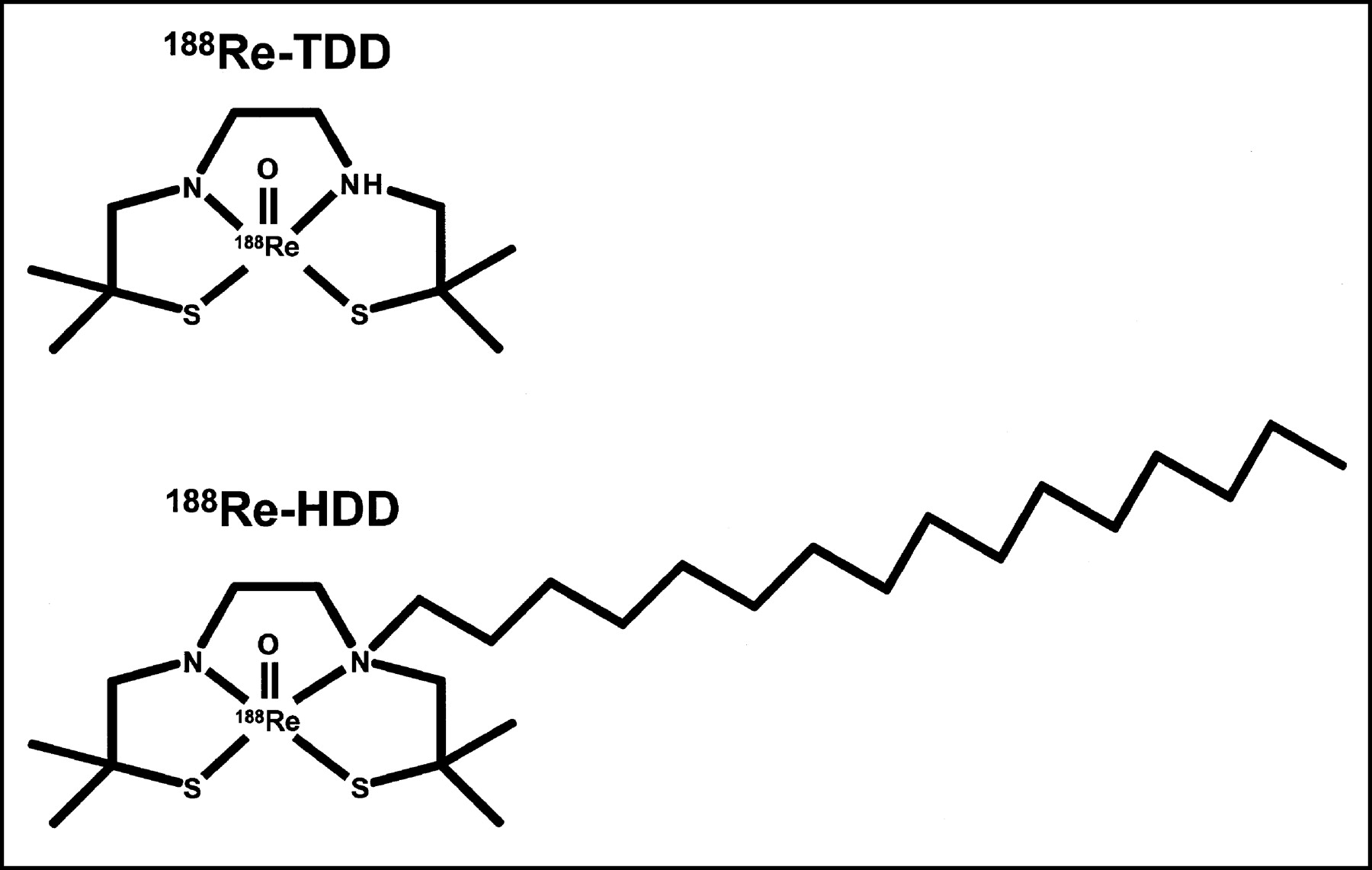
Molecular formulas of 188Re-TDD and 188Re-HDD. TDD is derivative of N2S2 compound, and its 188Re chelate is highly lipophilic. 188Re chelate of HDD has higher lipophilicity because of presence of long alkyl chain.
In this study, we compared the tumor retention of 188Re-TDD/lipiodol and 188Re-HDD/lipiodol solutions after TAE in liver cancer-xenografted rabbits. In addition, both the required dose of radioactivity for human application and the radiation dosimetry for major organs were calculated using the results of this animal experiment.
MATERIALS AND METHODS
Preparation of Agents and Cancer-Bearing Rabbits
The method of preparing the 188Re-HDD and TDD lipiodol solutions has previously been reported (14,15). The preparation was straightforward and was performed using a simple kit, which also has previously been reported (16).
VX2 carcinoma was induced in the livers of 8 rabbits. VX2 is a kind of dermatologic squamous cell carcinoma of rabbits induced by the Shope virus and is a widely used model of metastatic hepatic tumor (17). VX2 carcinoma was inoculated in the left lobes of livers by injection of 0.5 mL of tumor suspension with an 18-gauge needle during laparotomy. The method of preparing the VX2 carcinoma was the same as previously reported (18). Tumor size was checked by CT imaging serially. Only rabbits having tumors of 2–3 cm were included in the experiment.
TAE, Image Acquisition, and Analysis
TAE was performed by a femoral approach. The femoral artery was punctured, and the tumor-feeding artery was selectively catheterized using a 3.0-French catheter (Microferret; William Cook Europe). To prevent vasospasm, a mixed solution of verapamil (100 μg) and nitroglycerin (200 μg) was injected after selection of the celiac axis. About 185 MBq/0.4 mL of 188Re-TDD/lipiodol or 188Re-HDD/lipiodol were then injected through the catheter. Each group contained 4 rabbits. The efficacy of TAE and the retention of lipiodol were evaluated on the follow-up CT scan.
At intervals of 1, 2, 6, 24, and 48 h after TAE, conjugated anterior and posterior whole-body scans were obtained using a dual-head γ-camera (Prism2000; Picker International) with medium-energy general-purpose collimators. The energy window was centered for 155 keV and opened by ±15%. Images were acquired for 10 min using a 256 × 512 matrix. Regions of interest (ROI) were drawn manually on a 1-h image around areas of high uptake. Whole-body ROIs were also drawn around the body contour. ROIs of the same size and shape were applied to 2-, 6-, 24-, and 48-h images. The radioactivity counts of each ROI were determined by the geometric mean of the counts obtained from anterior and posterior images, using:
 Eq. 1 where CROI is the calculated geometric mean of the counts in the ROI, CROIant is the ROI count of the anterior image, and CROIpost is the ROI count of the posterior image.
Eq. 1 where CROI is the calculated geometric mean of the counts in the ROI, CROIant is the ROI count of the anterior image, and CROIpost is the ROI count of the posterior image.
Although similar doses were injected through the hepatic arteries, the initial tumor uptake could have been different because of several factors, such as adhesion of the agent to the catheter, spillover from the selected artery, and intratumoral arteriovenous shunts. Initial tumor uptake was calculated by regressive extrapolation using the time-activity curve.
Dosimetry
Exponential linear regression analysis was performed using the CROI values obtained from the images, and decay constants were calculated. A half-life and a residence time for 188Re-TDD and 188Re-HDD were also calculated from the decay constant. The residence time is defined as half-life/ln 2 and is a more useful parameter for dosimetry. The calculated residence times were compared for the 188Re-TDD and 188Re-HDD groups using the Mann-Whitney U test. In this study, all decay constants and half-life values were calculated in the form of effective decay constant and effective half-life, which consider both the physical decay of the radioisotope and biologic washout from the ROI.
On the basis of the residence times obtained from the experiments, the dose necessary for human application was calculated. Tumor self-radiation S-values were obtained for variable tumor sizes using the Nodule Module in MIRDOSE3.1 software (Oak Ridge Associated University) (19). From the calculated S-values and residence times in the rabbit model, the amount of radioactivity to obtain 100 Gy of tumor irradiation was calculated.
Radiation exposures of major organs were also calculated using MIRDOSE3.1 software. Based on the rabbit distribution data, the S-values for major organs were obtained and the radiation exposures for man were predicted assuming an administration of 740 MBq.
RESULTS
Preparation and TAE
The overall radiochemical yields were 72% ± 5% and 65% ± 7% for 188Re-TDD/lipiodol and 188Re-HDD/lipiodol, respectively. Their radiochemical purities were always higher than 95%.
The average mass of the induced tumor at the time of TAE was measured as 10.9 ± 7.2 g on CT. Most of the tumors had several small satellite daughter nodules. Although TAE was generally satisfactory (Fig. 2), a rabbit in the 188Re-TDD group was excluded from the analysis because of a technical failure. Therefore, 7 rabbits were included in the final analysis. Intratumoral arteriovenous shunts of various degrees were generally observed in angiography.

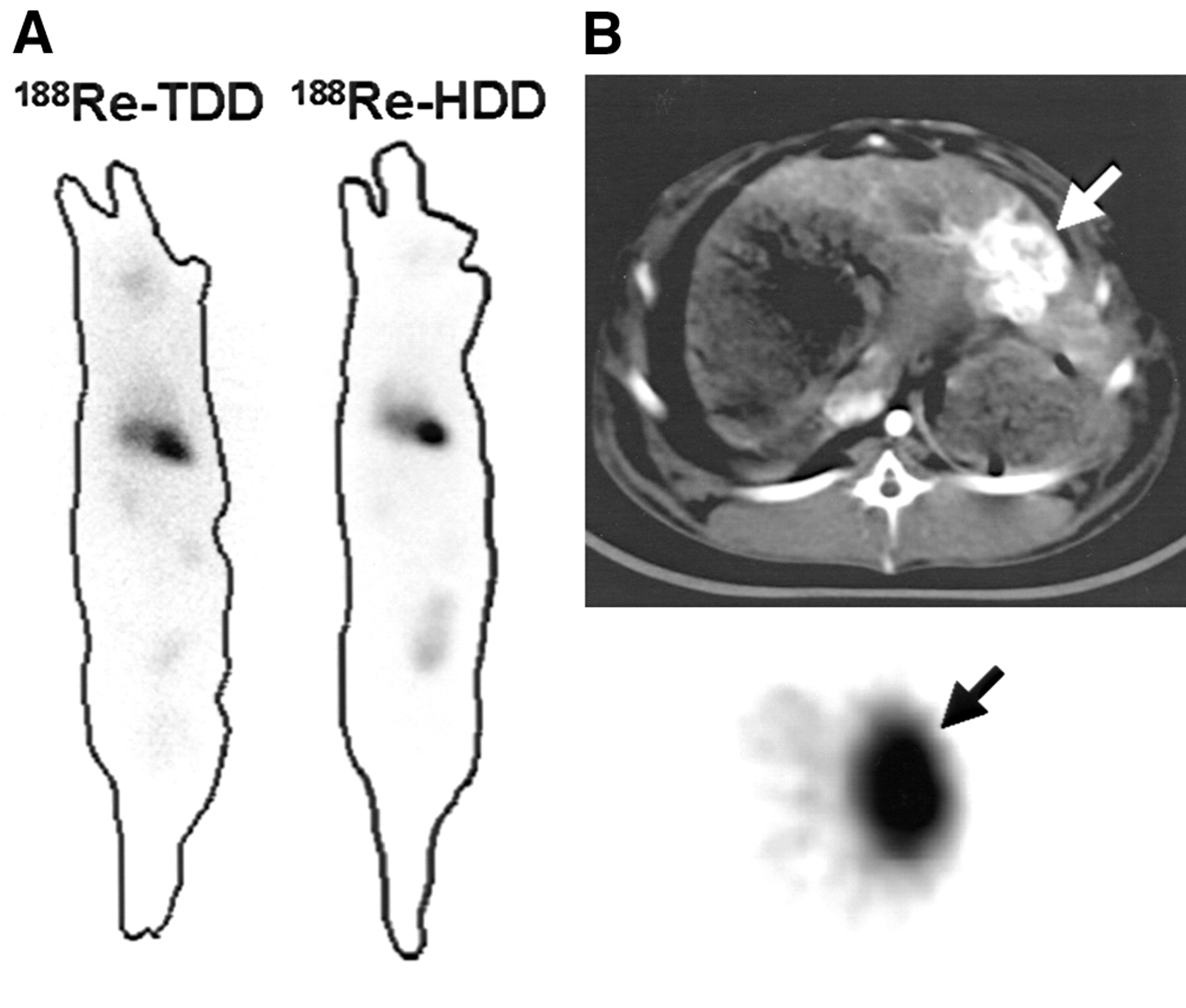
Rabbits with TAE. (A) ROIs were drawn for whole body and tumor in rabbits of each group. (B) In CT (top) and SPECT (bottom) images, lipiodol (white arrow) and matching radioactivity (black arrow) were effectively localized and visualized in hepatic tumors.
Image Acquisition and Calculation of Residence Time
Examples of acquired images are shown in Figure 2. 188Re-HDD was retained longer in the tumor than was 188Re-TDD (Fig. 3). 188Re-TDD showed higher gut activity, indicating excretion mainly through the hepatobiliary tract, whereas 188Re-HDD showed minimal gut activity and higher bladder activity. The decay curves are shown in Figure 4, and the calculated decay constants, effective half-lives, and residence times are summarized in Table 1. The residence time of 188Re-HDD was 17.6 h, which was significantly longer than that of 188Re-TDD, 10.2 h (P = 0.034).

Dynamic images of 188Re-HDD/lipiodol and 188Re-TDD/lipiodol. 188Re-HDD shows significantly longer retention in tumor (arrow) until 48 h than does 188Re-TDD. 188Re-TDD was excreted to gut faster than was 188Re-HDD.
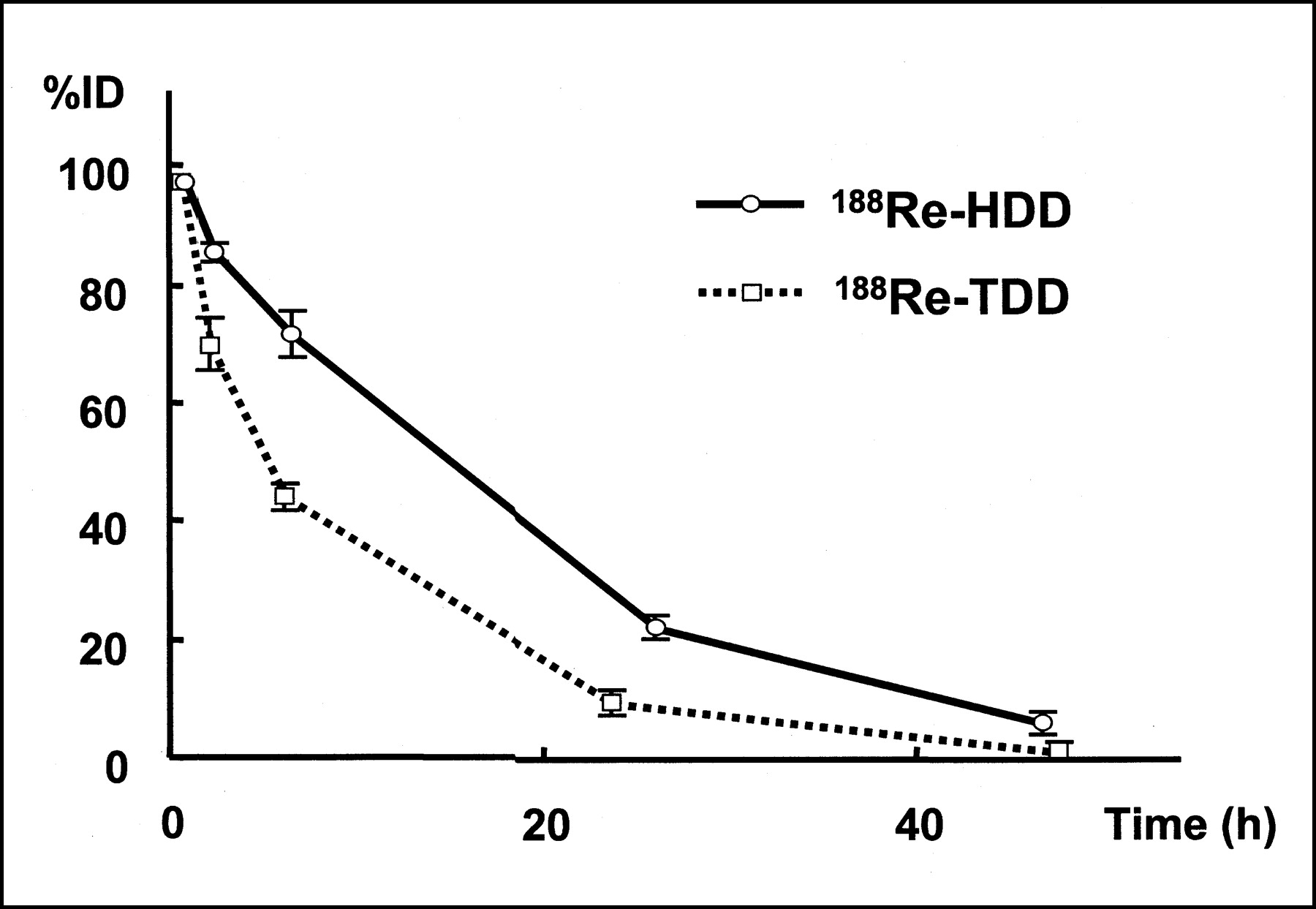
Time-activity curve of ROIs around hepatic tumors for 188Re-TDD/lipiodol and 188Re-HDD/lipiodol treatment. Half-life and residence time of 188Re-HDD/lipiodol were significantly longer than those of 188Re-TDD/lipiodol.
Calculated Parameters for Tumor Retention of 188Re-Labeled Agents in Liver
Calculation of Radioactivity Dose Required for Human Application
The nodular self-dose S-values were acquired using MIRDOSE3.1. From these S-values and the mean residence times, the radioactivity required for a target irradiation dose of 100 Gy was calculated for both the 188Re-TDD/lipiodol and 188Re-HDD/lipiodol groups. The necessary dose of radioactivity required for human application was 142–1,070 MBq of 188Re-HDD/lipiodol for a 2.64- to 5.27-cm tumor (Table 2). Significantly less 188Re-HDD/lipiodol was required for the given target dose of irradiation.
Required Doses of Radioactivity for Tumor Irradiation of 100 Gy in Various-Sized Tumors
The radiation exposure of a major organ was calculated assuming an administered dose of 740 MBq of 188Re-HDD/lipiodol. The liver was the organ of highest radiation exposure, and the urinary bladder was the second most irradiated organ. The proportion of excreted radioactivity was 27%. However, the radiation exposures of critical organs, including the red marrow and the liver, were within tolerable ranges, and the calculated whole-body radiation exposure was 155 mSv (Table 3).
Radiation Exposures of Major Organs for 740 MBq of 188Re-HDD/Lipiodol Solution Administered via Hepatic Artery
DISCUSSION
188Re is a promising candidate for a therapeutic radioisotope. It has appropriate β- and γ-rays for therapy and imaging and an adequate half-life of 17 h. In addition, it is conveniently provided by an in-house generator system. To take advantage of 188Re in TAE, direct labeling of lipiodol was initially tried yet was not easy because of some chemical limitations. Because 188Re is obtained in an aqueous form whereas lipiodol is available as an oil form, they are chemically immiscible. In addition, if a bifunctional chelating agent is linked with lipiodol for labeling, the chemical property of the resultant conjugate is altered.
Making a solution of 188Re-labeled lipophilic agent with lipiodol is a practical method bypassing direct labeling of lipiodol. Nevertheless, in cases of solution form, tumor retention without dissociation and washout is an important concern. This was the actual situation encountered when 188Re-TDD/lipiodol was first developed as a solution form. However, 188Re-HDD, which has a stronger hydrophobic interaction with lipiodol because of its long alkyl chain, demonstrated better clinical applicability than did 188Re-TDD, with improvement of tumor retention by 1.8-fold. In this study, 188Re-HDD/lipiodol showed an effective half-life of 12.2 h and a biologic half-life of 69 h, which were comparable to the values for directly labeled lipiodol agents (5,6).
Because direct administration of radioactivity to the lesion is involved, radioembolization in TAE is considerably dependent on the operator’s skill. The rabbit TAE model has several technical difficulties uncommon in humans. For example, severe vasospasm and spillover of the agent from the selected artery occurred despite premedication with vasodilators. Moreover, minute selection of the tumor-feeding artery was nearly impossible because of the small diameter of the artery. In human TAE, however, vasospasm is not a big concern, and well-trained interventional radiologists can easily select the feeding artery. Therefore, the radioactivity should be delivered more efficiently in humans.
In the present study, about 20% of the administered radioactivity was localized in the tumor or in the tumor-bearing hepatic lobe. Madsen et al. reported that when 131I-ethiodol (ethiodol is a type of poppy seed oil used for TAE) was injected via the hepatic artery, 69%–90% of the radioactivity localized to the liver and 10%–12% localized to the hepatic tumor (7). In humans, the general assumption is that 50% of lipiodol injected during TAE accumulates in the hepatic tumor (8). The remaining 50% is lost through arteriovenous shunts or by spillover from the hepatic artery. With this assumption, the necessary dose for humans can be calculated by doubling the results shown in Table 2.
In TAE through irradiation, the organ of most concern for protection from radiation is the lung, because a significant amount of the nonlocalized lipiodol usually accumulates in the lung. About 30% of the administered radioactivity was reported to accumulate in the lung in cases of 131I-lipiodol administration (8). However, no significant detectable radioactivity from 188Re-HDD/lipiodol was found in the lung in this study, probably because of dissociation of 188Re-HDD from lipiodol.
This study suggests that the kidney and urinary bladder should be the main organs of concern for radioprotection, because most 188Re-HDD/lipiodol was excreted through the renal system. Lipiodol itself is eliminated as 2 components. After catabolism, the iodine component of the lipiodol complex is excreted through the renal system and the lipid component is excreted through the biliary system (20). Although the exact mechanism has not been established, most of the excreted radioactivity of 188Re-HDD was found in the bladder. Consequently, no organ except the liver and the bladder was significantly irradiated by the radiotherapy.
In the hypothesis of the Nodule Module in MIRDOSE3.1, radioactivity is homogeneously distributed in the tumor. However, because the injected radioactivity is retained in the microvasculature of the tumor and the necrotic portion usually does not have microvasculature, the dose of irradiation delivered to cancer cells is somewhat higher than the calculated amount. Furthermore, because the Nodule Module of MIRDOSE3.1 considers only the self-radiation dose, the amount of irradiation applied to the tumor would be somewhat higher if the radioactivity around the tumor were also considered. A more complicated model is needed to accurately calculate the actual irradiation of the tumor. However, the dose calculated by this study may be used as an approximate guideline for clinical trials.
Although radiolabeled tumor-specific peptides are studied extensively for targeting and treating cancer, they are less practical than 188Re-HDD/lipiodol. Many human studies have shown that less than 1% of the injected dose accumulated in tumors. Therefore, the required dose for delivery of enough radiation to cancer would be 10–50 times that of 188Re-HDD/lipiodol.
A limitation of this study was image resolution for small animals such as rabbits. Some important information, such as the tumor-to-nontumor ratio in the liver, could not be assessed because of the small size of rabbits and the Bremsstrahlung effect of high-energy β-rays. However, this limitation did not affect the main results of the study, because the achieved resolution was sufficient for our purposes.
CONCLUSION
Lipiodol solution of 188Re-HDD, containing a long alkyl chain, was retained in tumors significantly longer than was 188Re-TDD. Therefore, 188Re-HDD/lipiodol had better potential as a new therapeutic agent in TAE for liver cancer. The necessary dose of radioactivity for human application was 142–1,070 MBq of 188Re-HDD/lipiodol for a 2.64- to 5.27-cm tumor. After 740 MBq of 188Re-HDD/lipiodol were administered, the radiation exposures of major organs were within the tolerable range and the radiation exposure of the whole body was 155 mSv.
Acknowledgments
The authors thank Young Ju Kim and Dr. Dong Soo Lee for their contribution to this study and appreciate Keagan Lee’s kind language support. This study was supported by the Korean Ministry of Science and Technology, with additional funding from the Nuclear Research Program for Application.
Footnotes
Received Apr. 24, 2003; revision accepted Sep. 8, 2003.
For correspondence or reprints contact: Jae Min Jeong, PhD, Department of Nuclear Medicine, Seoul National University Hospital, 28 Yeongeon-dong Jongno-gu, Seoul, 110-744, Korea.
E-mail: jmjng{at}snu.ac.kr
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.