


Abstract
Captopril renography is a reliable, widely used test for the functional diagnosis of renovascular hypertension. Well-recognized drawbacks of the procedure include reduced accuracy in patients with bilateral disease or renal impairment as well as the possible interference from concurrent antihypertensive medication (diuretics, β-blockers, angiotensin-converting enzyme inhibitors, calcium channel blockers). Currently, no data exist regarding the reliability of captopril renography in patients with renovascular hypertension evaluated while they are under chronic treatment with angiotensin II (AT1) receptor antagonists (Sartans). Moreover, the renographic response of the kidney with renal artery stenosis to prolonged therapy with angiotensin II receptor antagonists has not yet been evaluated. Methods: We investigated the diagnostic effectiveness of 99mTc-mercaptoacetyltriglycine captopril renography performed after acute addition of 25 mg of captopril to the daily dose of AT1 receptor antagonist in 13 patients with unilateral renal artery stenosis and subsequent evidence of renovascular hypertension, based on short-term (3 mo) blood pressure outcome after revascularization. The renographic evaluation was first performed after ingestion of the daily therapy of angiotensin II receptor antagonist alone (Sartan renography) and was repeated within 7 d after the acute addition of 25 mg of captopril to chronic treatment with angiotensin II receptor antagonist (captopril-Sartan renography). A cohort of 13 patients with a final diagnosis of essential hypertension was chosen as the control subjects. Results: Twelve of 13 patients were correctly detected by captopril-Sartan renography (92% sensitivity), and 3 subjects were also identified without the addition of captopril. Adding captopril to Sartan therapy resulted in a slight reduction in mean arterial blood pressure, while significant side effects were never observed. No false-positive results were found in the 13 patients with essential hypertension. Conclusion: We conclude that performing captopril renography with the acute addition of 25 mg of captopril to the chronic monotherapy with Sartans has the same diagnostic effectiveness as performing captopril renography alone. Interrupting the vasoactive action of angiotensin II alone on the efferent glomerular arteries, which can also be selectively achieved by chronic administration of angiotensin II receptor antagonists, does not fully explain the effectiveness of captopril renography in detecting renovascular hypertensive patients.
- renovascular hypertension
- angiotensin II (AT1) receptor antagonists
- captopril renography
- renal artery stenosis
It is well known that some concurrent antihypertensive medications can decrease the overall accuracy of captopril renography and that chronic treatment with angiotensin-converting enzyme (ACE) inhibitors should be discontinued for several days before the study (1–3). Angiotensin II, the principal effector of the renin-angiotensin system, can now be selectively inhibited by orally active receptor antagonists—that is, Sartans, at the level of the subtype 1 receptors (4). Sartans represent a continuously growing, heterogeneous family of drugs (5–7) with a wide array of pharmacologic characteristics, including bioavailability, binding specificities, dissociation rates, and affinity to receptors. They induce a dose-dependent blockade of angiotensin II effects and are generally better tolerated than ACE inhibitors. Both Sartans and ACE inhibitors lower blood pressure, increase renal plasma flow, decrease proteinuria, and do not affect glomerular filtration rate, and several studies have suggested that combining an ACE inhibitor with an angiotensin II receptor blocker is more effective to block the renin-angiotensin system than either substance given alone (8,9).
To date, it is still not known how or whether chronic administration of Sartans acts on the diagnostic effectiveness of captopril renography. Therefore, as a precaution, angiotensin II receptor blockers should also be discontinued before the study (1–10). However, the effects of chronic therapy with ACE inhibitors on renal hemodynamics may be somewhat different from those produced by prolonged therapy with Sartans. Moreover, unneeded discontinuation of antihypertensive therapy may uselessly complicate the feasibility of a diagnostic procedure such as captopril renography, and this is quite relevant from a practical point of view.
The objective of this clinical study was to investigate the effectiveness of captopril renography in patients with a definite diagnosis of renovascular hypertension, evaluated during chronic monotherapy with Sartans. In addition, the renographic behavior of the ischemic kidney after prolonged treatment with Sartans was also investigated.
MATERIALS AND METHODS
Study Population
The files of 75 hypertensive patients who underwent captopril-Sartan renography from January 1998 to December 2002 were reviewed retrospectively and, to be included in the study, the patients had to meet the following criteria:
Renographic evaluation performed after at least 2 wk of therapy with Sartans (with or without thiazide) and repeated within 7 d, 60–90 min after ingesting 25 mg of captopril in addition to daily therapy with Sartans
Normal or near-normal renal function (i.e., serum creatinine ≤ 1.4 mg/dL)
Split function of the kidney with arterial stenosis ≥ 30%
Angiographic evidence of >50% unilateral renal artery stenosis
Improvement or cure of hypertension after revascularization
Only patients with unilateral renal artery stenosis, normal or near-normal renal function, and split function of the kidney with stenosis ≥ 30% were included in the study, because renal failure and the presence of a poorly functioning kidney increase the likelihood of false-negative results. Thirteen patients (8 men, 5 women; age range, 27–79 y; with improved [n = 9] or cured [n = 4] hypertension after revascularization) met the criteria. Patient characteristics (age, sex, angiographic results, revascularization type, and early blood pressure outcome) are given in Table 1.
Patient Characteristics
The inclusion criteria for hypertensive patients recruited as control subjects were the following:
Renographic evaluation performed after at least 2 wk of therapy with Sartans (with or without thiazide) and repeated within 7 d, 60–90 min after ingesting 25 mg of captopril in addition to daily therapy with Sartans
Normal or near-normal renal function (i.e., serum creatinine ≤ 1.4 mg/dL)
The same age range as the study patients
A definite, clinical diagnosis of essential hypertension
The blood pressure response after renal revascularization was classified according to the U.S. Cooperative Study of Renovascular Hypertension criteria (11). A patient was said to be cured if the supine diastolic blood pressure was <90 mm Hg without antihypertensive medication, whereas a decrease in the diastolic blood pressure of at least 15%—although with values still >90 mm Hg and <110 mm Hg—was classified as an improvement.
Renal Scintigraphy
In agreement with the referring physician, antihypertensive drugs were withheld 2–7 d before the study with the exception of angiotensin II blockers. The first renographic evaluation was performed 2.5–3 h after ingestion of the daily therapy of angiotensin II receptor antagonist (Sartan renography). Thirty minutes before the study, we started hydrating the patients with 7–10 mL water/kg body weight; then they were asked to empty their bladder immediately before the study. Patients were positioned supine with the camera below them, and an intravenous line with saline was established.
Computerized data acquisition (10-s per frame in a 128 × 128 pixel matrix for 180 frames) was performed using a large-field-of-view gamma camera (XRT-Starcam 4000i; General Electric) equipped with a low-energy, high-resolution collimator, immediately after a bolus injection of 1.5 MBq/kg body weight of 99mTc-mercaptoacetyltriglycine (99mTc-MAG3) (Mallinckrodt Medical).
After checking that the patients were fasting and not volume depleted, a second renographic study was performed within 7 d, 60–90 min after swallowing a crushed 25-mg tablet of captopril, 2.5–3 h after intake of their daily dose of Sartan (captopril-Sartan renography). Before the administration of captopril, the subject’s arterial blood pressure was checked twice, and patients with values <130/80 mm Hg were rescheduled. After captopril administration, blood pressure was measured and recorded at 15-min intervals for 120 min.
One patient (patient 7) was first evaluated by 99mTc-diethylenetriaminepentaacetic acid (Sartan renography) and afterward by 99mTc-MAG3 (captopril-Sartan renography).
Baseline renography was performed within 2 wk, at least 5–7 d after discontinuing Sartan therapy.
Background-subtracted time-activity curves and 3-min serial images were generated from a second online computer (Pegasys Workstation; ADAC Laboratories), and data analysis was performed by plotting regions of interest around the whole kidney and cortex. The presence of unilateral cortical retention of radiotracer found on qualitative or quantitative evaluation, which was no longer recognizable or less evident at baseline study (i.e., difference in time-to-maximum activity of at least 2 min or in the 20-min-to-maximum ratio of the cortical activity of ≥15%), was deemed suggestive of renovascular hypertension (10).
RESULTS
On intraarterial digital subtraction angiography, 3 patients had mild-to-moderate stenosis (50%–70%) and 10 had severe stenosis (>70%). Arterial stenosis was caused by atherosclerosis in 9 patients (1 case of ostial restenosis after a previously conducted balloon angioplasty) and by fibromuscular disease in 4 patients. One patient had stenosis in a branch of the main renal artery, and 2 patients had single stenosis in the kidney with multiple renal arteries.
The short-term (3 mo) blood pressure outcome after revascularization (4 percutaneous renal angioplasties and 9 percutaneous angioplasties with endovascular stenting) showed improvement in 9 patients and cure in 4 patients.
Renographic results are summarized in Table 2. Twelve of 13 subjects (92%) were correctly detected by captopril-Sartan renography (Fig. 1). Two patients (patients 1 and 6) with positive captopril-Sartan renography had stenosis involving only 1 of 2 hilar arteries, and 1 patient (patient 3) had branch stenosis. The only patient with negative captopril-Sartan renography (patient 2) was also negative for captopril renography, which had been performed under amlodipine, 2 wk after discontinuing Sartan intake.
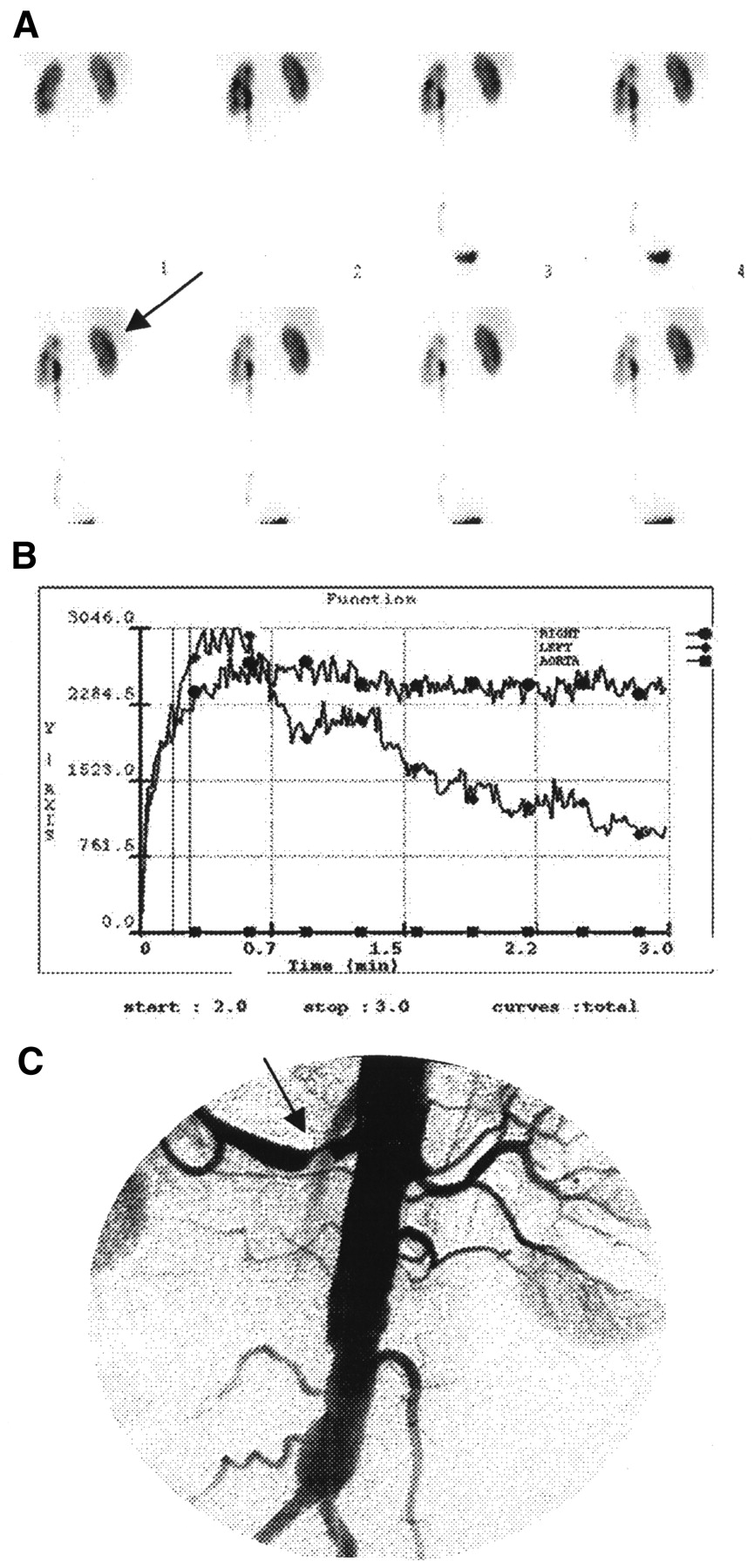
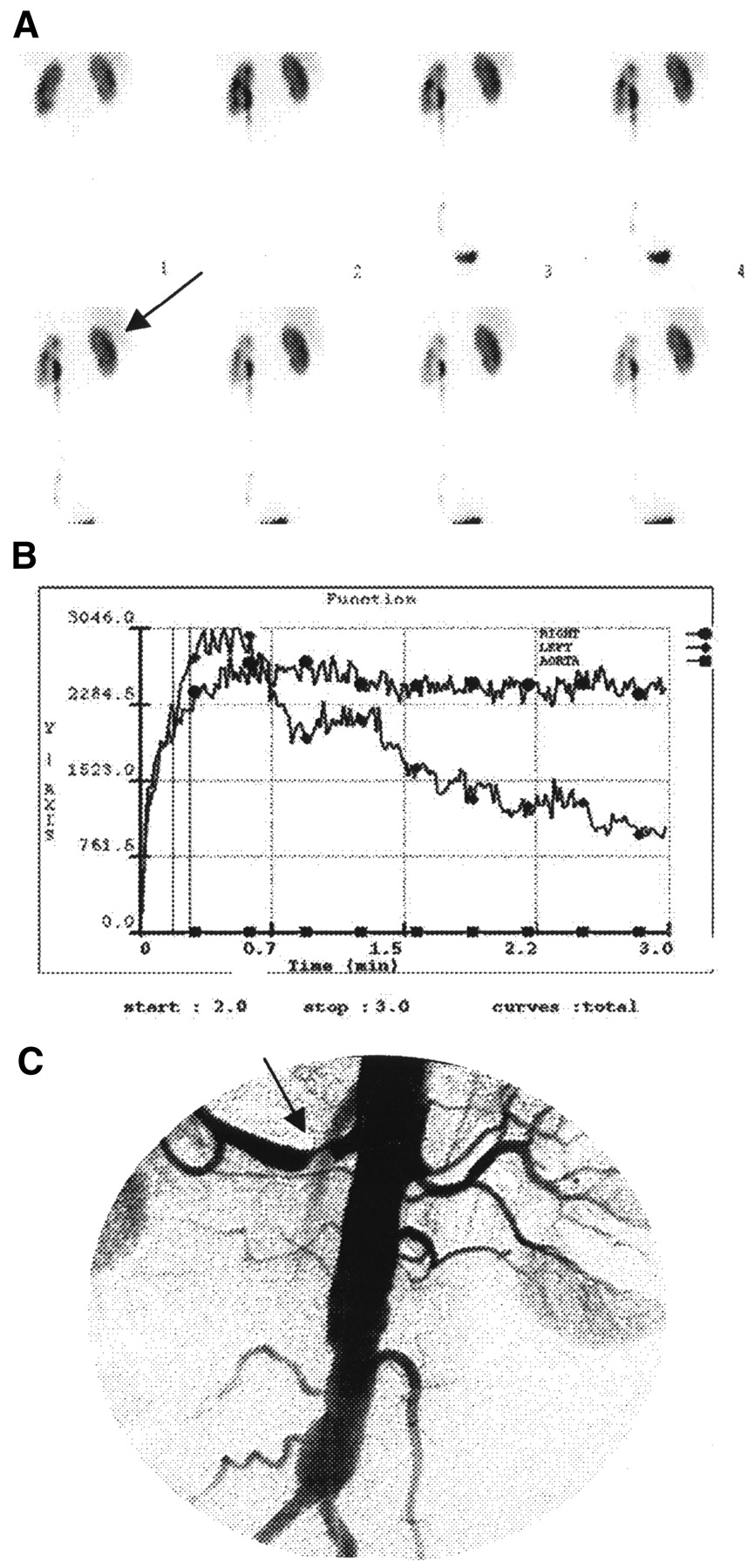
Patient 7: Positive captopril-Sartan renography (80 mg valsartan + 25 mg captopril) in 69-y-old woman with >70% truncal stenosis of right renal artery (C, arrow). There is bilateral delayed excretion on renograms (B) with cortical retention in right kidney on scinti-images (A, arrow) suggesting lateralization. (C) Arteriogram shows severe stenosis (arrow) of right renal artery. Hypertension control improved after angioplasty and stent placement.
Results of Renography Listed by Case
Three of 13 patients were also detected by Sartan renography (patients 5, 8, and 12) (Fig. 2). Of interest, only kidneys with renal artery luminal narrowing of >70% and relative uptake of the involved kidney of <40% were positive on Sartan renography. Two patients had normal renography under Sartan, and the remaining 8 patients had renographic evidence of a moderately decreased uptake of 99mTc-MAG3, with or without delayed transit and excretion of the involved kidney (Fig. 3), that did not change significantly on renography performed under baseline conditions. For ethical reasons, 2 patients with normal renography under Sartan did not undergo a baseline study. For these patients, we considered the Sartan renography, rather than the baseline renography, as the reference study, and thus compared this with the captopril-Sartan renography.

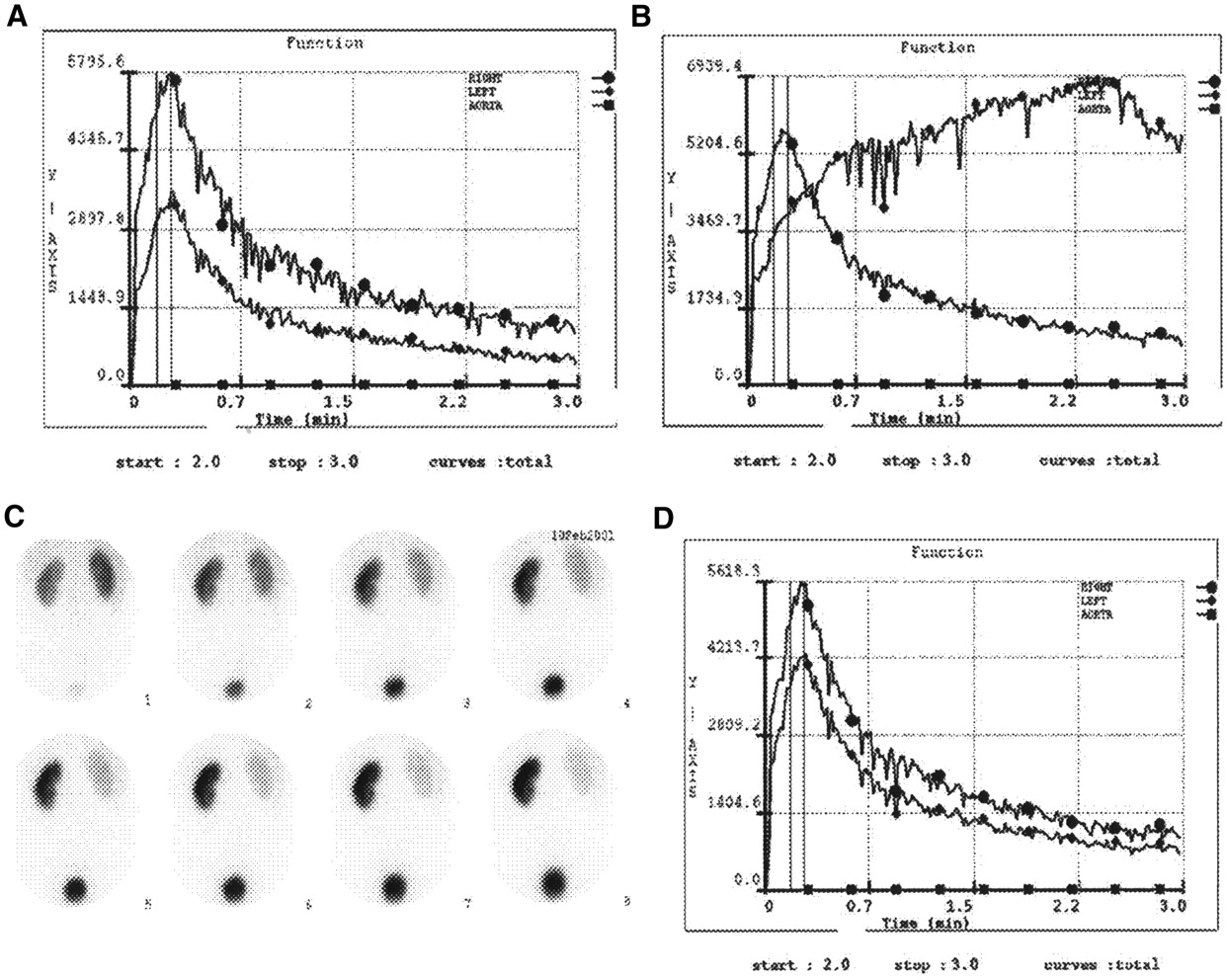
Patient 8: Positive Sartan renography (80 mg valsartan) in 39-y-old man with >70% fibromuscular stenosis of left renal artery (E, arrow). There is parenchymal retention and delayed excretion in left kidney (A and B) that is no longer detectable on baseline renography (C) and on captopril renography (D) performed after revascularization. (E) Arteriogram shows severe stenosis (arrow) of left renal artery. (F) Arteriogram after angioplasty and stent insertion illustrates wide patency of artery. Hypertension was cured after revascularization and split function of left kidney unexpectedly improved from 34% to 45%.
Patient 13: Negative Sartan renography (150 mg irbesartan) with positive captopril-Sartan renography (25 mg captopril + 150 mg irbesartan) in 61-y-old man with >70% ostial stenosis of left renal artery. (A) Sartan renogram only shows nonspecific reduction of left kidney uptake. (B) Captopril-Sartan renogram demonstrates diminished uptake in left kidney, with abnormal curve suggesting left-sided renovascular disease. (C) Captopril-Sartan sequential 3-min images illustrate prolonged cortical retention in left kidney. (D) Captopril renogram after angioplasty and stent placement shows only decreased amplitude of left renal curve. Hypertension control improved after revascularization.
Pre-captopril mean arterial blood pressure was 109 mm Hg (range, 84–152 mm Hg) and 90 min after captopril intake was 103 mm Hg (range, 77–128 mm Hg). Acute addition of 25 mg of captopril to Sartan therapy usually resulted in a slight reduction in mean arterial blood pressure, while no hypotension or significant side effects were ever observed.
No false-positive results were found in the 13 patients with essential hypertension chosen as the control subjects.
DISCUSSION
Clinical practice has proven that captopril renography is a reliable, cost-effective test for the functional diagnosis of renin-dependent renovascular hypertension, particularly in patients with unilateral renal artery stenosis and normal or moderately reduced renal function (1–3,12). The predictive value of positive captopril renography is high, but some conditions, such as concurrent antihypertensive medication and dehydration or hypotension, can increase the number of false-positive results (13,14). This should not be a problem, because these conditions usually act bilaterally and symmetrically, therefore warning the reporting physician of the possible misinterpretation of the study (15). Conversely, chronic ACE inhibition may cause false-negative results (16,17) that are technically indistinguishable from true-negative responses. Therefore, ACE inhibitors should be discontinued before performing the study (1–3,10,16,17).
The renin-angiotensin system can now be selectively inhibited by angiotensin II (AT1) receptor antagonists (Sartans), and treatment with this class of drugs should also be discontinued, as a precaution, before the study (1). However, the effects of chronic therapy with Sartans on renal hemodynamics may be somewhat different from those produced by prolonged therapy with ACE inhibitors. It is well known that ACE inhibition often produces incomplete suppression of angiotensin II levels and that the effects of ACE inhibitors on angiotensin II levels are under the influence of the renin response. ACE inhibition-induced renin secretion causes angiotensin I levels to increase and promotes ceaseless angiotensin II generation by residual uninhibited ACE. Moreover, in long-term treatment with ACE inhibitors, the blockade of angiotensin II synthesis might become less effective through the activation of alternative pathways of angiotensin II production that would restore previous levels of angiotensin II (18). This condition—called “ACE escape”—might decrease the effectiveness of captopril renography, especially in patients undergoing chronic treatment with ACE inhibitor. One possible pathway of alternative angiotensin II generation is shown in Figure 4. Conversely, the distinct advantage of interrupting the renin-angiotensin system, which is achieved by Sartans at the angiotensin II receptor level, is that it blocks the action of angiotensin II, regardless of its formation pathway. Thus, acute addition of 25 mg of captopril to chronic treatment with angiotensin II receptor antagonists may be more effective at blocking the renin-angiotensin system than captopril alone.
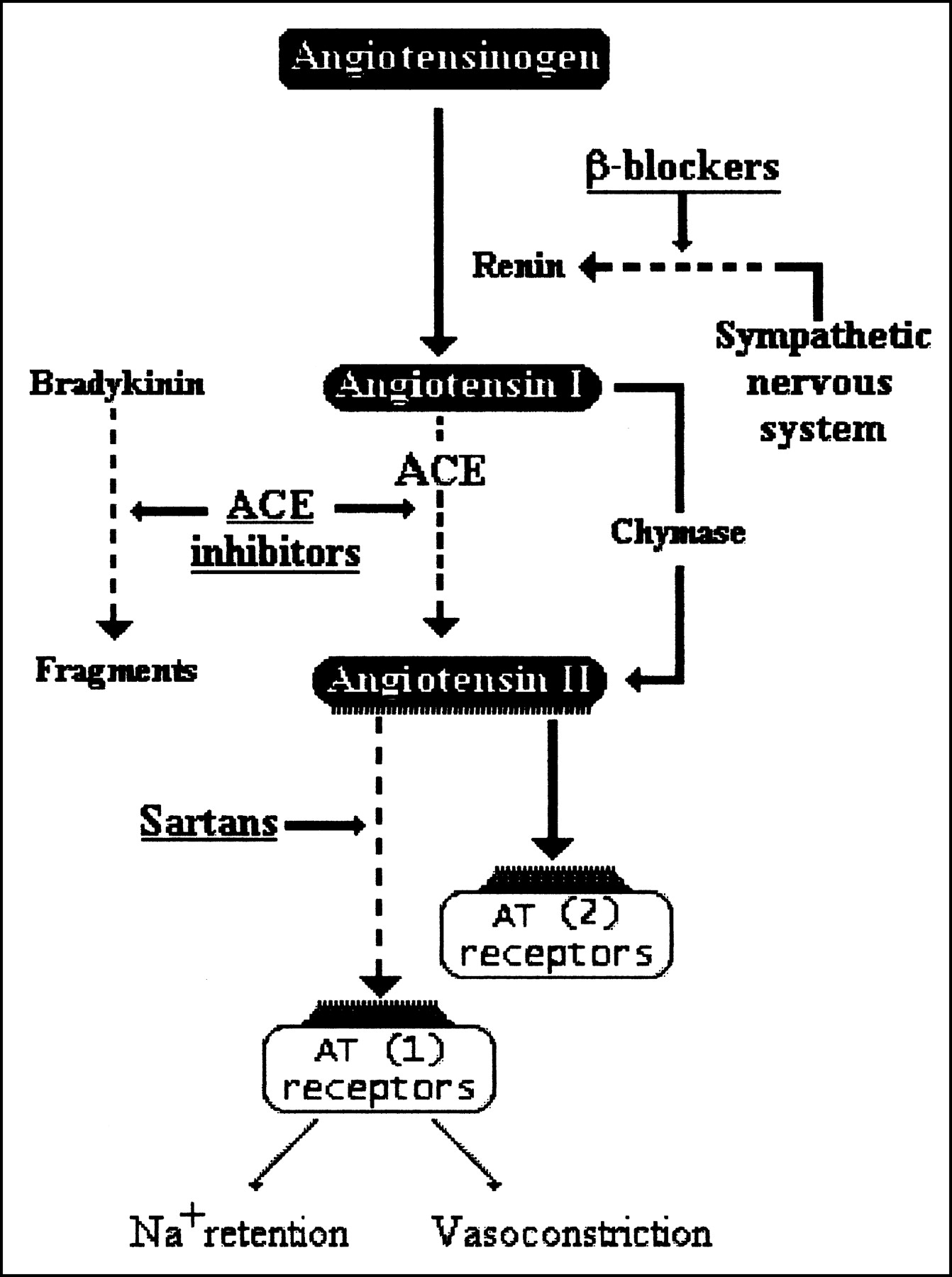
Outline of renin-angiotensin system.
The results of our study are in accordance with the above observations. Despite the limited number of cases that were evaluated, it should be emphasized that the percentage of patients with renovascular hypertension detected by captopril-Sartan renography was high (12/13) and that 3 patients with regional ischemia, from stenosis involving only 1 of 2 hilar arteries (2 patients) and from branch stenosis (1 patient), were also successfully detected. Moreover, the 1 patient not detected by captopril-Sartan renography was also negative for captopril renography, and no false-positive results were found in the 13 patients with essential hypertension recruited as the control subjects.
The main limitation of our study is that we cannot compare the effectiveness of captopril-Sartan renography against captopril renography. However, the sensitivity of captopril-Sartan renography (92%) was similar, or even better than the values reported for captopril renography (1–3), and suggests that discontinuation of prolonged treatment with Sartans is not a requisite for the diagnostic effectiveness of captopril renography.
Although the primary goal of our study was to evaluate the reliability of captopril-Sartan renography, we also investigated the renographic response of the stenosed kidney after prolonged treatment with angiotensin II receptor antagonists alone (Sartan renography). Only 3 of 13 patients were detected by Sartan renography (Fig. 2). Even though the renal effects of chronic and acute administration of drugs interfering with the renin-angiotensin system may be somewhat different, these results are consistent with the findings by Karanikas et al., who investigated the effectiveness of Sartan renography after a single ingestion of 80 mg of valsartan (19). Because Sartans induce a dose-dependent blockade of angiotensin II effects, a possible explanation for the negative results of Sartan renography could be that the blockade of AT1 receptors was incomplete at the administered doses. This possibility was recently emphasized by Maillard et al., who assessed the reactive rise of plasma renin activity values as a marker of AT1 receptor blockade efficacy and found that some AT1 receptor antagonists, administered at the recommended dose, exhibit less-than-optimal blockade efficacy (20).
Although we cannot exclude this hypothesis, we believe that ineffective dosing may account for only some of the negative results. We performed Sartan renography 2.5–3 h after ingestion of the Sartan dose—that is, roughly when the blood level of the drug was at its peak. Moreover, 8 of 13 patients took Sartan twice a day, and the duration of therapy before performing Sartan renography was >8 wk in 10 of 13 patients (Table 2). Hence, ineffective dosing may account for only some of the negative results, because the dosing of angiotensin II receptor blockers was, at the time of examination—more often than not—adequate to antagonize the AT1-mediated angiotensin II effects.
Another explanation might be that Sartans are less effective than captopril in reducing efferent arteriolar tone. It must be stressed that the transglomerular pressure gradient and glomerular filtration rate depend on preglomerular and postglomerular arteriolar resistances, increasing with selective efferent vasoconstriction or afferent vasodilatation. The main effect of captopril that is not shared by Sartans is the influence on the bradykinin metabolism, because ACE (kininase II) participates in catabolizing bradykinin to inactive peptides (21–23). Thus, inhibition of ACE produces an increase in bradykinin plasma levels, which, in turn, enhancing the production of nitric oxide and prostacyclin, counteracts angiotensin II and endothelin-1 vasoconstrictor action (24–27).
It is well known that renal vasodilating prostaglandins play an important role in maintaining the renal blood flow and glomerular filtration rate, particularly under conditions of elevated angiotensin II levels. In kidneys with mild-to moderate renal arterial stenosis, vasodilating prostaglandins limit the glomerular filtration rate decrease by reducing angiotensin II-mediated preglomerular constriction without interfering with postglomerular constriction (28). Under these circumstances, inhibition of prostaglandin biosynthesis, as shown by the favorable results obtained by aspirin renography, may be critical to the modulation of renal vascular resistances (29,30). When the degree of renal arterial stenosis is severe, the greater narrowing of the renal artery limits the effects of vasodilating prostaglandins on the renal blood flow, whereas the non-counteracted action of angiotensin II on postglomerular arteries preserves the glomerular function. In this context, ACE inhibition decreases the angiotensin II-dependent constriction of the postglomerular arteries and, in addition, enhancing the levels of bradykinin, causes selective efferent arteriolar dilatation and further reduces the resistances at the postglomerular level (31). The result is that captopril is more likely to reduce the glomerular capillary pressure and glomerular filtration rate than Sartans are. Like captopril, Sartans can also increase bradykinin levels through unopposed activation of the AT2 receptors (32), but the magnitude of this increase is usually much lower than that after ACE inhibitor. The fact that Sartan renography was positive only in the kidneys with renal artery luminal narrowing of >70% and split function of <40% would appear to be of the utmost importance, because in these conditions the expression of AT2 receptors may be upregulated (33), and the Sartan-induced blockade of the angiotensin II-mediated postglomerular constriction may be adequate to induce a significant decrease in the glomerular filtration rate.
CONCLUSION
The reliability of captopril renography did not worsen by the chronic administration of Sartans, and the acute addition of 25 mg of captopril was safe and free of side effects. Unlike ACE inhibitors, Sartans might neutralize at the target level the activation of alternative pathways of angiotensin II production or ceaseless angiotensin II formation by uninhibited ACE, thus preserving, or even enhancing, the diagnostic effectiveness of captopril renography.
The poor sensitivity of Sartan renography suggests the possibility of ineffective Sartan dosing in some patients and that captopril-induced reduction in bradykinin breakdown might play a key role in the renographic detection of renovascular hypertensive patients by captopril renography.
Acknowledgments
The authors acknowledge the assistance provided by Valerie Perricone in reviewing the manuscript. This work was supported in part by a grant from Byk Gulden Italia.
Footnotes
Received Feb. 20, 2003; revision accepted May 20, 2003.
For correspondence or reprints contact: Giuseppe Picciotto, MD, SC Medicina Nucleare 1, Ospedale Molinette, Corso Bramante 88, 10126 Torino, Italy.
E-mail: gpicciotto{at}molinette.piemonte.it
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.