


Abstract
This study evaluated the role of 99mTc-sestamibi washout in the prediction of pathologic tumor response to neoadjuvant chemotherapy in 30 patients with locally advanced breast cancer. Methods: Two 99mTc-sestamibi studies were performed before and after chemotherapy for each patient. Early (10 min) and delayed (240 min) planar breast views were acquired after a 740-MBq 99mTc-sestamibi intravenous injection, and the washout rate (WOR) was computed. All patients underwent radical mastectomy with pathologic evaluation of the residual tumor size. Results: The pretherapy 99mTc-sestamibi WOR ranged from 14% to 92% (mean ± SD, 50% ± 18%). At pathologic examination, 15 patients showed no tumor response to chemotherapy and 15 patients showed an objective response to chemotherapy. The pretherapy 99mTc-sestamibi study predicted chemoresistance (WOR > 45%) in 18 of 30 patients and no chemoresistance (WOR ≤ 45%) in 12 of 30 patients. When the WOR cutoff was set at >45%, the prognostic performance of the test was indicated by a sensitivity of 100%; a specificity of 80%; positive and negative predictive values of 83% and 100%, respectively; and a likelihood ratio of 5. The repeatability of the test was good, with 80%–93% interreader agreement (κ = 0.57−0.85). Posttherapy 99mTc-sestamibi studies confirmed the pretherapy study prediction in 29 of 30 patients. Conclusion: 99mTc-Sestamibi WOR is a reliable test for predicting tumor response to neoadjuvant chemotherapy. In fact, negative findings (WOR ≤ 45%) rule out chemoresistance and positive findings (WOR > 45%) indicate a high risk of chemoresistance.
Biochemical resistance to chemotherapy is the major cause of treatment failure in patients with breast cancer. In fact, an intrinsic chemoresistance is present in 18%–51% of untreated cancer, whereas resistance is acquired later during the treatment in up to 75% of patients (1–3).
Chemoresistance is a multifactorial phenomenon including several nonspecific and specific mechanisms (4–7). The term multidrug resistance (MDR) is commonly used to indicate an overexpression of transmembrane glycoproteins, the P-glycoprotein (Pgp), and the MDR-associated glycoprotein (1,8). These proteins allow outward transport of the most important antineoplastic chemotherapeutic drugs, such as anthracyclines, and are responsible for the clinical manifestation of the MDR phenotype in breast cancer (7–12). Knowledge of the MDR pattern before and during the treatment can improve therapy planning, including selection of drug-resistant patients for chemorevertant drugs.
The available in vitro techniques to measure MDR gene expression in tumor samples are clinically ineffective to achieve this aim (13–15) because they do not necessarily provide information about the dynamic function of drug efflux pumps (16). 99mTc-Sestamibi [hexakis (2-methoxy-isobutylisonitrile) technetium (I)], a radiopharmaceutical widely used as a tumor-seeking agent for diagnostic imaging (17,18), has been recently used as a general probe for functional imaging of these 2 MDR pumps (19–21). Several clinical studies have therefore been designed to study Pgp functionality with 99mTc-sestamibi in cancer patients (22–24), and a correlation between the efflux rate of 99mTc-sestamibi and quantitative Pgp expression in breast carcinoma patients was clearly evident in a pilot study (25).
This study evaluated the prognostic value of 99mTc-sestamibi washout for predicting the outcome of neoadjuvant chemotherapy in locally advanced breast cancer using pathologic tumor response as the gold standard.
MATERIALS AND METHODS
Study Design
This phase II clinical trial was a prospective cohort study on a sample of 30 patients with untreated locally advanced breast cancer. The patients were evaluated before neoadjuvant chemotherapy and were followed until surgery to verify the chemotherapy outcome.
The primary endpoint of the study was determination of the prognostic value of 99mTc-sestamibi scintigraphy in predicting tumor response to neoadjuvant chemotherapy. The predictor variable of chemoresistance was considered 99mTc-sestamibi washout in the pretherapy study (prognostic test). The outcome variable was considered the residual tumor size evaluated on pathologic samples.
The tests and the outcome results were read in a standardized and masked fashion. The local Ethics Committee approved the study, and all patients gave written informed consent before entering the study.
Patients
Thirty patients (age range, 31–70 y) with locally advanced breast cancer entered the study on the basis of the following eligibility criteria: clinical stage, according to the system of the Union Internationale Contre le Cancer, of T2 ≥ 3 cm N0–N1 M0, T1–T3 N2 M0, or T4 N0–N2 M0 and adequate hematologic function (baseline total white blood cell count ≥ 4 × 109/L, neutrophil count ≥ 2 × 109/L, and total platelet count ≥ 100 × 109/L). The following exclusion criteria were also considered: a performance status ≥ 1 according to the criteria of the World Health Organization; previous hormonal treatment, chemotherapy, or radiotherapy; evidence of systemic metastases or a second active malignant tumor; and severe heart disease or insulin-dependent diabetes.
Protocol
Before starting chemotherapy, all patients underwent a baseline evaluation that included a clinical examination, bilateral mammography, fine-needle aspiration cytology or histologic biopsy of the lesion, bone scintigraphy, standard chest radiography, liver sonography, and a basal 99mTc-sestamibi study. The clinical tumor size was determined by measuring the 2 largest perpendicular diameters evidenced on clinical and mammographic examinations.
Two chemotherapy regimens were used. Schedule A, administered to 7 patients, included 3 cycles of chemotherapy (cyclophosphamide, 400 mg/m2; epirubicin, 50 mg/m2; and fluorouracil, 500 mg/m2, on days 1 and 8) every 3 wk. Schedule B, administered to 23 patients, included 4 cycles of high-dose epirubicin (80 mg/m2 plus docetaxel, 75–80 mg/m2, on day 1) every 3 wk. Granulocyte colony-stimulating growth factor as support therapy was administered when required.
At the end of chemotherapy, the patients were reevaluated clinically, mammographically, and with 99mTc-sestamibi. All patients underwent radical mastectomy and axillary lymphadenectomy, with pathologic examination of the removed tumor and nodes.
99mTc-Sestamibi Scintigraphy
Two 99mTc-sestamibi scintigraphic studies, with different aims, were performed for each patient before and after chemotherapy. The study performed before chemotherapy investigated the risk of intrinsic chemoresistance and was aimed at predicting tumor response to chemotherapy (prognostic test). The study performed after the end of chemotherapy and immediately before surgery investigated the effect of the just-completed chemotherapy. This latter study was aimed at assessing the actual tumoral mass (diagnostic test) and at confirming the pretherapy study prediction. Both studies were performed with the following criteria.
Image Acquisition.
99mTc-sestamibi (Cardiolite; DuPont Pharmaceuticals Co., Billerica, MA), 740 MBq, was injected intravenously in the arm contralateral to the lesion. Early (10 min after the injection) and delayed (240 min after the injection) acquisitions were obtained with the patient carefully placed in the same position. In both acquisitions, digital planar images of the breast region (256 × 256 matrix, 10-min preset time) were acquired with the patient prone (lateral views) and supine (anterior views). A large-field-of-view gamma camera (PRISM 2000 XP; Picker Medical Systems, Cleveland, OH) equipped with a high-resolution low-energy parallel-hole collimator and a dedicated foam rubber mattress was used.
Image Reading and Processing.
Tumoral and background regions of interest were drawn on the lateral views of the early images and then translated to the delayed images to compute mean 99mTc-sestamibi uptake counts. The uptake index was calculated both for early and for delayed images by the ratio of tumor to background mean count, with decay correction for delayed images. The washout rate (WOR) was computed by the ratio of delayed to early uptake index, with decay and background correction as follows: WOR = [(T − B)10 min − (T − B) 240 min]/(T − B)10 min, where T is the tumoral region of interest and B is the background region of interest. Film reading and processing were performed in clinically masked fashion. Intra- and interobserver agreements for WOR estimation were evaluated.
Pathologic Studies
Mastectomy specimens from each patient were evaluated. The pathologic residual tumor size was estimated as the residual tumor burden and quantitated from the 2 largest perpendicular diameters, measured in centimeters. The number of metastatic nodes was also evaluated for each patient.
Hormone receptor status (estrogen and progesterone receptors) was determined immunohistochemically on frozen sections using commercially available kits. The cutoff value was nuclear staining of 10% of neoplastic cells.
Data Evaluation
Prognostic Test Results.
Prediction of tumor response to neoadjuvant chemotherapy was based on the results of the pretherapy 99mTc-sestamibi WOR. Accordingly, the test was defined as a positive prognostic test when it predicted high expression of intrinsic chemoresistance and, consequently, a high risk of no tumor response to the therapy. The test was conversely defined as a negative prognostic test when it predicted low expression of intrinsic chemoresistance and, consequently, a low risk of no tumor response to the therapy. The criteria for defining a test as positive or negative were based on the WOR cutoff point identified by the likelihood ratio method.
Outcome Measures.
The gold standard of the study was the objective response of the primitive tumor to neoadjuvant chemotherapy, as evaluated on pathologic specimens obtained at surgery. An objectively determined reduction in the dimensions of the tumor (i.e., reduction of the product of the 2 largest perpendicular diameters of the pathologic residual tumor size vs. the baseline clinical tumor size) was considered the criterion for pathologic response. The pathologic outcome was classified as no response to chemotherapy if the residual tumor size was reduced <75% or was increased. The pathologic outcome was conversely classified as a positive response to chemotherapy if the residual tumor size was reduced >75%. Accordingly, patients presenting with no response to chemotherapy were considered to be nonresponders, whereas patients presenting with a positive response to chemotherapy were considered to be responders.
Other Results.
Tumor response to chemotherapy was also evaluated by determining clinical response and scintigraphic response as additional outcome measures. Clinical response, evaluated through clinical examinations and mammography, was classified as positive or negative according to whether tumor reduction was appreciable or not. Scintigraphic response was evaluated by comparing early 99mTc-sestamibi uptake in the posttherapy study (diagnostic study) versus the pretherapy study (prognostic study). Scintigraphic response was classified as positive if tracer uptake was markedly reduced and negative if tracer uptake was not reduced or only faintly reduced.
Statistical Analysis
The results of 99mTc-sestamibi prognostic tests were expressed in terms of sensitivity, specificity, positive and negative predictive values, and likelihood ratio; 95% confidence intervals were also evaluated for sensitivity and specificity. A 2-tailed t test or Fisher exact test was used, as appropriate, to evaluate differences between clinical, scintigraphic, and pathologic response; differences between early and delayed uptake in pretherapy studies; and differences in baseline variables between groups of responders and nonresponders. Correlations between outcome variables and baseline tumor size, TNM stage, histologic type, pretherapy early uptake index, and WOR were evaluated by the Spearman ρ test. The level of probability significance was set at an α value of 0.05. The repeatability of the test was assessed by evaluating intrareader and interreader agreement among the institutional reader (a dedicated senior resident) and 2 other masked readers using κ statistics. A κ value > 0.75 was considered an index of strong agreement beyond chance, whereas a κ value of 0.40–0.75 was considered an index of intermediate to good agreement (26).
RESULTS
Table 1 lists the clinical and pathologic characteristics, including pathologic response, of each patient.
Patient Characteristics Before and After Chemotherapy
Prognostic Test Results
Early images (10 min) showed marked uptake of 99mTc-sestamibi in all tumors. The uptake index ranged from 0.48 to 4.85, with a mean of 2.05 ± 1.16. Only 16 of 23 node metastases showed 99mTc-sestamibi uptake. In delayed acquisitions (240 min), the 99mTc-sestamibi uptake index ranged from 0.33 to 4.85, with a significantly reduced mean value (1.64 ± 1.08, P = 0.003).
WOR ranged from 14% to 92% (mean, 50% ± 18%). Table 2 lists the scintigraphic results for each patient. The WOR cutoff was set at >45% by likelihood ratio analysis for the best test results. Accordingly, the test was defined as positive for 18 of 30 patients, who had a WOR > 45%, and negative for 12 of 30 patients, who had a WOR ≤ 45%. The intrareader coefficient of variation for WOR was <2%, and interreader agreement was high, ranging from 80% to 93% (κ = 0.57–0.85). The sensitivity, specificity, and predictive values of WOR are reported in Table 3.
Scintigraphic Results of Pretherapy 99mTc-Sestamibi Study
Prognostic Performance of Test
Outcome Results
After surgery, 15 patients had a substantially unmodified residual tumor (i.e., no response to chemotherapy) and 15 patients had a positive response to chemotherapy. The pathologic response for each patient is reported in Table 1. No significant difference in baseline characteristics (age, clinical tumor and node stage, and tumor size) between the 2 groups (responders and nonresponders) was observed. Outcome did not correlate with baseline tumor size, histologic type, schedule of treatment, or early 99mTc-sestamibi uptake index.
Other Results
Clinical response was positive in 15 patients and negative in 15, correctly identifying only 25 of 30 pathologic outcomes (accuracy, 83%). Scintigraphic response was negative in 16 patients and positive in 14, correctly identifying 29 of 30 pathologic outcomes (accuracy, 97%).
Scintigraphic response as evaluated on posttherapy 99mTc-sestamibi studies also confirmed the prediction of the pretherapy study for 29 of 30 patients (concordance of prognostic and diagnostic results, 97%; Figs. 1 and 2). In the only discordant case (patient 11), the pretherapy scintigraphic test wrongly predicted high MDR expression, whereas the posttherapy test correctly predicted a positive response to chemotherapy.
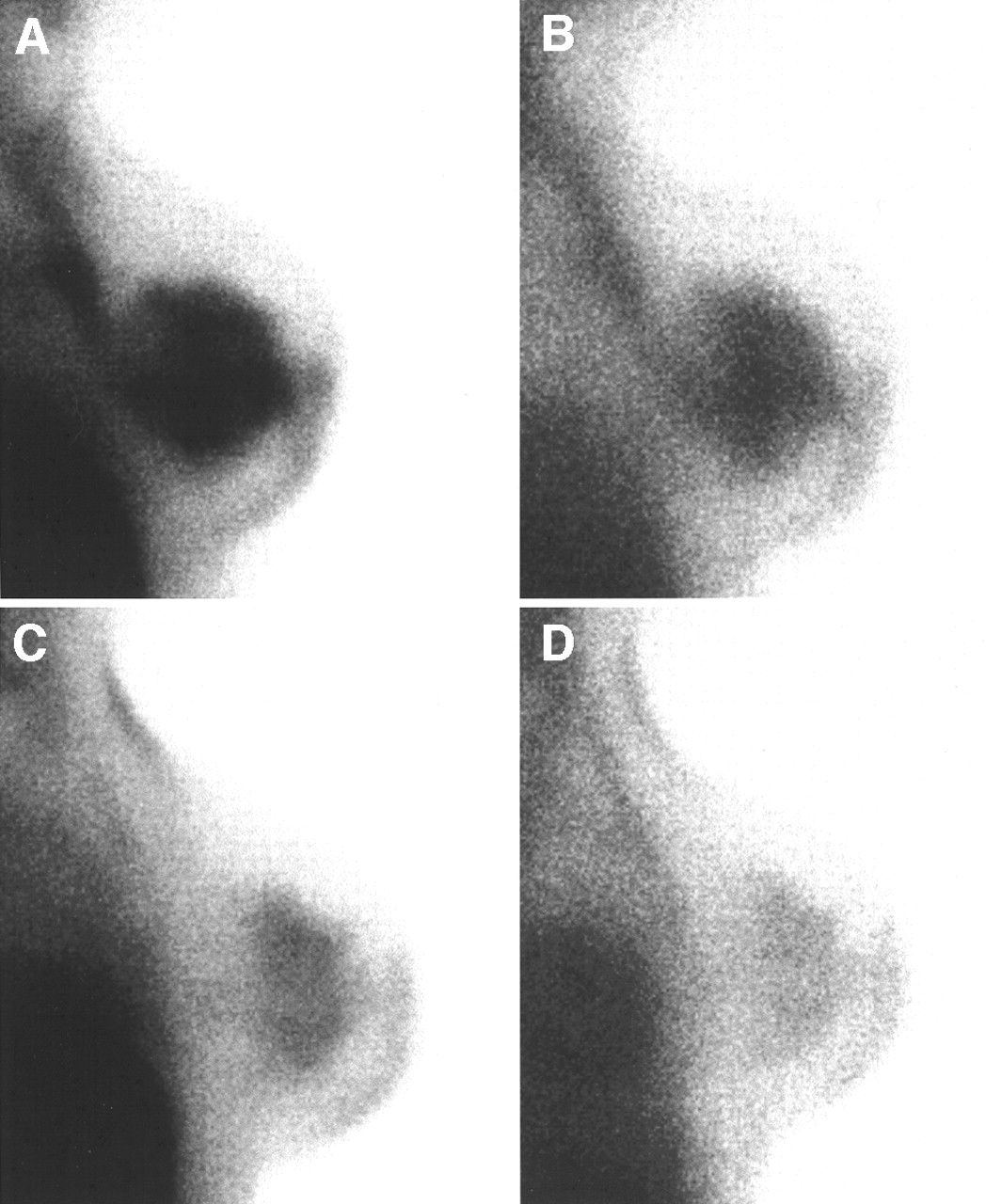
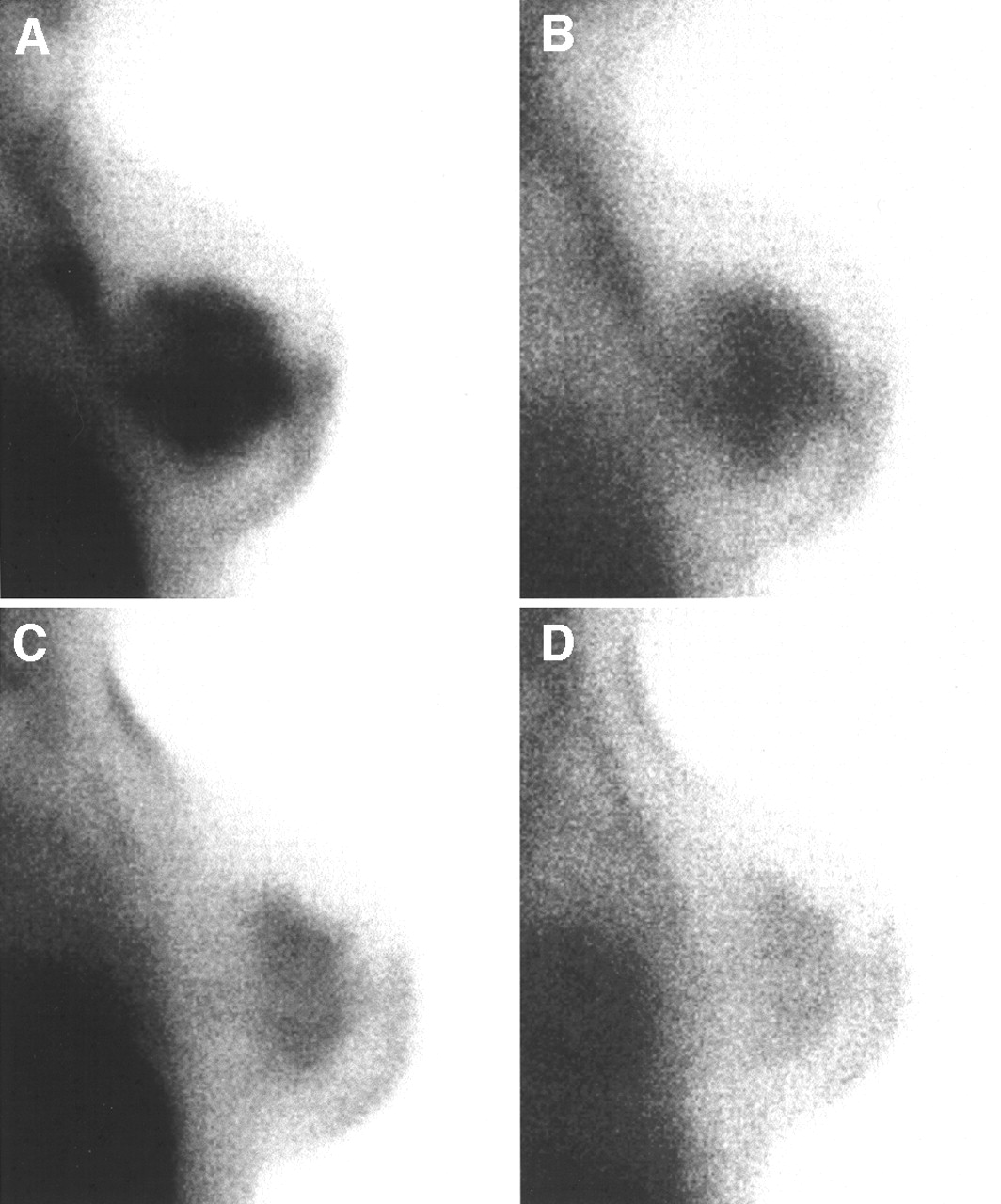
Pretherapy (A and B) and posttherapy (C and D) 99mTc-sestamibi studies (lateral views of right breast in prone position) of patient 30, who showed no response to chemotherapy at pathologic examination. Pretherapy study (A, early image; B, delayed image) evidenced high 99mTc-sestamibi WOR (51%), predicting high MDR expression. Early posttherapy image (C) confirmed negative response to chemotherapy, because tracer uptake persisted in tumoral region. Corresponding delayed image (D) showed evident decrease in tracer uptake, confirming high WOR and high MDR expression.
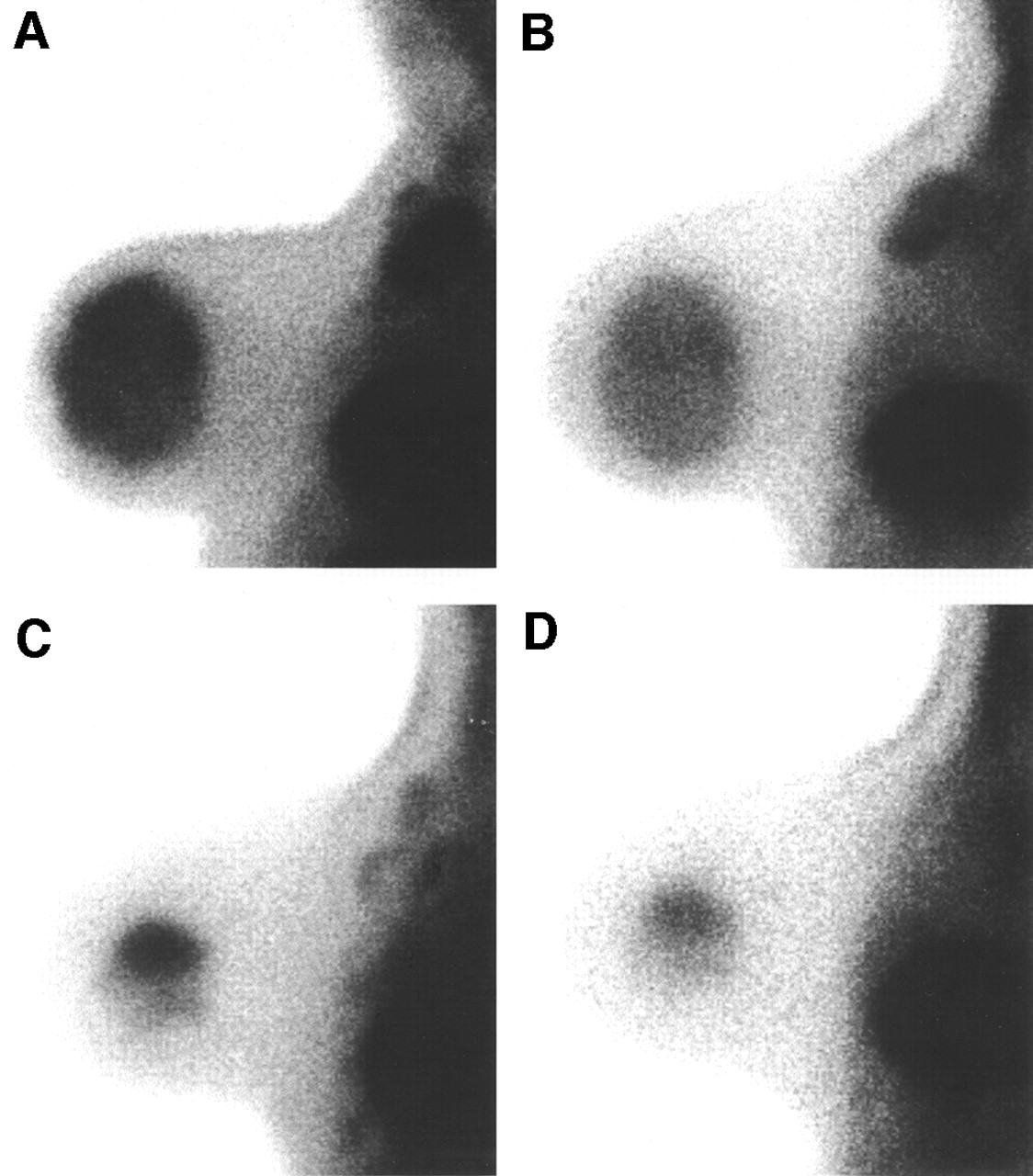
Pretherapy (A and B) and posttherapy (C and D) 99mTc-sestamibi studies (lateral views of left breast in prone position) of patient 29, who showed positive response to chemotherapy at pathologic examination. Pretherapy study evidenced very intense and diffuse tracer uptake both in tumor and in axillary nodes in early image (A) and low 99mTc-sestamibi WOR (30%) in delayed image (B), predicting low MDR expression. Early posttherapy image (C) confirmed positive response to chemotherapy, showing small area of residual tracer uptake in tumoral region and evident decrease of tracer uptake in axilla. Uptake remained substantially unmodified in corresponding delayed image (D).
No tumor characteristic (baseline tumor size, histologic type, or estrogen or progesterone receptor status) or other baseline variables (schedule of treatment or early 99mTc-sestamibi uptake index) correlated with the pathologic response to chemotherapy.
DISCUSSION
Intrinsic or acquired chemoresistance is the major cause of chemotherapy failure in many tumors, including breast cancer (1–4). MDR modulators may be used to increase the efficacy of chemotherapy when chemoresistance is identified (27). Unfortunately, immunohistochemical measurements of MDR glycoprotein on tumor samples are not effective for this purpose (13–16,28). Therefore, noninvasive imaging with 99mTc-labeled complexes revealing the function of cellular efflux pumps is a topic that raises much interest (17,19,21).
99mTc-sestamibi distribution and kinetics into tumoral cells is determined by mechanisms with different biologic significance. In fact, early 99mTc-sestamibi uptake is caused by negative potentials across the plasma membrane and the inner mitochondrial matrix and is an expression of tumor viability (17,29,30). Conversely, efflux is regulated by MDR glycoproteins and may be considered a marker of chemoresistance (19–21,31,32).
Preliminary clinical investigations on patients with breast cancer yielded promising results. A positive correlation was found between the efflux rate of 99mTc-sestamibi and Pgp expression (22) or lack of response to chemotherapy (25,33). Retention of 99mTc-sestamibi appeared to also correlate with chemosensitivity to anthracyclines (34).
Unfortunately, the available results are not comparable because of wide differences in study design, tumor histologic type, method of 99mTc-sestamibi scintigraphy acquisition and processing, and gold standard (24,35–37). The reliability of 99mTc-sestamibi efflux in predicting MDR remains to be validated, and a method for clinical routine use has not been standardized yet.
A well-designed study on this topic, with a reasonable gold standard (i.e., pathologic evidence of tumor response), was previously reported (33). The authors evaluated 99mTc-sestamibi efflux kinetics by clearance analysis in 39 patients with locally advanced breast cancer and concluded that this functional approach may identify patients at high risk of treatment failure. The method was too complex and time consuming for routine use, requiring both dynamic acquisition and 4 following planar images. In addition, the high rate of false-negative findings (35%) seriously limited the diagnostic performance of the test, considering the high prevalence of disease (59% of patients were nonresponders).
In this study, we validated a simple, reproducible, and reliable method for 99mTc-sestamibi WOR analysis. The method, requiring only 2 sequential planar images and a quantitative measure of an index (WOR) by simple regions-of-interest design, was more practical for routine examinations. Determination of the WOR cutoff value (>45%) by likelihood ratio analysis for best test results was also a simple method and closely fulfilled the need for a clinically useful criterion.
This method also performed well in predicting chemoresistance (Table 3). In fact, we observed a sensitivity significantly higher than that previously reported by Ciarniello et al. (33) (100% vs. 65%, P < 0.001) and a similar specificity (80% vs. 87%, P = 0.6). The difference in test sensitivity was likely caused by the different criteria used to set the cutoff value. In fact, Ciarniello et al. established their cutoff value by correlating 99mTc-sestamibi clearance (i.e., half-life) with in vitro Pgp expression. On the contrary, in our study the best test result was identified on the basis of objective pathologic tumor response to chemotherapy. Considering that not only Pgp but also MDR-associated glycoprotein is responsible for 99mTc-sestamibi efflux, systems measuring only Pgp expressions are likely to underestimate clinical chemoresistance and to be characterized by low sensitivity.
In our study, the negative predictive value of the test was 100%. This result ensured a good response to neoadjuvant chemotherapy by all patients with a negative test (i.e., WOR < 45%), ruling out all patients with high expression of chemoresistance. On the contrary, a positive test was associated with a high probability of chemoresistance (positive predictive value, 83%, with a 95% confidence interval of 58%–96%). In these patients, the use of chemorevertant or chemomodulator agents can be justified.
The high likelihood ratio observed (i.e., 5) indicated that the test result would greatly raise the prior probability of suspected disease. In fact, by applying Bayes’ equation for clinical diagnosis, we could observe a posttest probability of disease of 72%–88%, as opposed to a pretest probability of 35%–59%. This further analysis confirmed that the 99mTc-sestamibi WOR was clinically useful for assessing the probability of intrinsic chemoresistance in patients with locally advanced breast cancer before neoadjuvant chemotherapy planning.
A false-positive test was observed in 3 patients (20%). Two of these patients presented with strongly inflammatory disease that showed very diffuse and intense uptake. These characteristics probably interfered with the mechanisms of 99mTc-sestamibi kinetics. In the third patient, the WOR in the prognostic study was high, whereas the diagnostic test showed an evident reduction in 99mTc-sestamibi uptake in the tumor after chemotherapy. This patient had a positive pathologic response but was found to have progressing disease immediately after surgery.
Another interesting observation concerns the WOR value obtained in the posttherapy study. All patients with a high WOR on the pretherapy study also had a high value on the posttherapy study, confirming the presence of chemoresistance. In addition, 5 of 12 patients with a low WOR (<45%) before therapy showed a high WOR (>45%) on the posttherapy study. These patients could have acquired chemoresistance during neoadjuvant chemotherapy. In fact, in addition to the presence of intrinsic chemoresistance, which remains unaffected by the first cycle of chemotherapy, the development of acquired resistance during treatment must be considered. Acquired resistance develops mostly through mutation of gene induction but can also arise when a resistant fraction survives from a tumor that initially responded to the chemotherapy (27). The change in WOR pattern from low to high during neoadjuvant chemotherapy can represent survival of a resistant tumor fraction or any other mechanism implied in induction of chemoresistance. Further data on long-term follow-up are clearly needed to confirm this hypothesis.
CONCLUSION
This study showed that 99mTc-sestamibi WOR, as a test for predicting tumor response to neoadjuvant chemotherapy, is reliable, simple, noninvasive, reproducible, and effective. The clinical role of the test is quite important, because a negative test (WOR ≤ 45%) rules out chemoresistance, ensuring the effectiveness of neoadjuvant chemotherapy. Conversely, a positive test (WOR > 45%) indicates a high probability of chemoresistance and suggests that chemorevertant or chemomodulator agents should be used.
Acknowledgments
This study was supported in part by grant 2490/00/CadC from the Fondazione Italiana per la Ricerca Sul Cancro.
Footnotes
Received Aug. 14, 2001; revision accepted Feb. 4, 2002.
For correspondence or reprints contact: Rosa Sciuto, MD, via della Giuliana 83/a, 00195, Rome, Italy.
E-mail: sciuto{at}ifo.it





{kind=link}
{kind=link}