


Abstract
There has been no consensus on a standard calculational approach regarding the concept of administered activity in ventilation studies involving inhaled radioisotope gas or radioaerosols. This is caused in part by a lack of knowledge regarding the actual activity that enters the lung space (as opposed to activity introduced into the delivery system) and to the extended administration times (ta) associated with delivery protocols. Methods: This pamphlet reviewed the three primary ventilation procedures, including rebreathing-system protocols, continuous-flow generator output techniques, and radioaerosol delivery systems. Results: For each technique, an analytic expression has been derived for a new parameter called lung administered cumulated activity, ÃL(0,ta), which is the cumulated activity in the lungs during the administration phase. In addition, another potentially useful parameter has been defined—the mean administered activity for ventilation procedures, which normalizes the administered cumulated activity in the lung over the administration period and may serve to standardize descriptions of protocols between patients and institutions. Examples are provided that illustrate these new concepts for typical ventilation protocol administration parameters. Conclusion: The models presented can be employed to evaluate lung administered cumulated activity for use in ventilation dose estimate reports as a function of explicit variables (e.g., spirometer volume, generator output rate, wash-in half-time, administration time). In practice, it is recommended that dose estimate reports be based on measurements of cumulated activity in the lung over the administration period and normalized to this administered cumulated activity.
Concepts involving administered activity for ventilation studies have not been adequately defined or standardized for use in dose estimate reports involving inhaled radioisotope gas or radioaerosols. Two principal factors contributing to this situation are lack of knowledge of the activity that enters the lung space (as opposed to activity introduced into the ventilation delivery system) and the extended period of time required for administration until equilibrium is established or the wash-in phase is otherwise terminated. In this report, the concepts associated with administered activity during ventilation studies are reviewed, and a practical definition involving administered cumulated activity is developed.
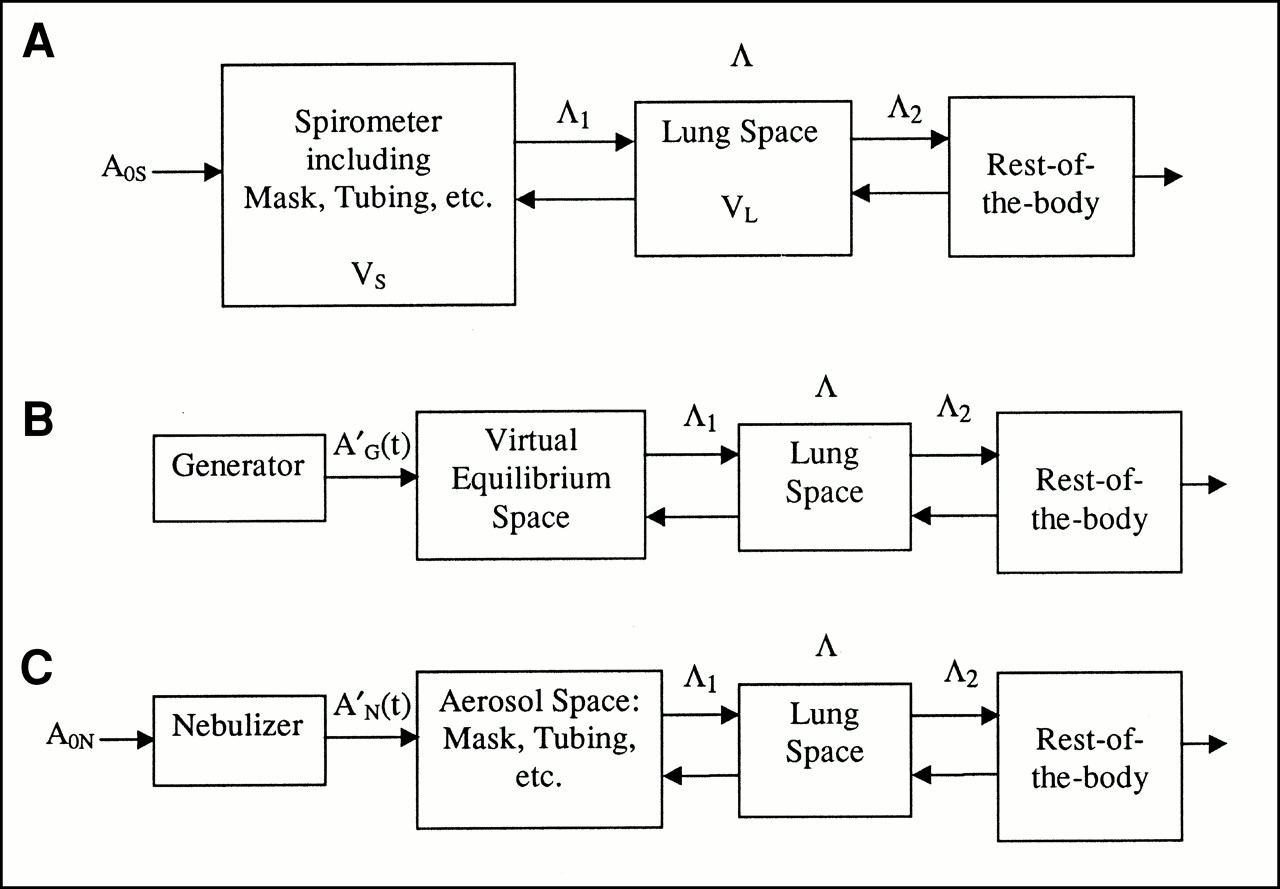
The ventilation study procedures to be considered include rebreathing-system protocols (spirometer/mouthpiece or mask) (1–3), continuous-flow generator output techniques (4–8), and radioaerosol delivery systems (9–12). Figure 1 provides schematic representations of these delivery methods. For the rebreathing system (Fig. 1A), A0S represents the activity introduced into the closed spirometer volume (at time t = 0). Radioactivity equilibrium is reached through breathing-induced exchange between the spirometer volume and the lung space. The rest of the body compartment communicates with the lungs and also provides biologic exit pathways. For the generator-based protocol involving a continuous flow of air (or oxygen) through the generator (Fig. 1B), AG′(t) represents the generator output activity rate (assumed to be constant for this discussion) introduced into the patient mask. As a convenience in the model description, a “virtual” equilibrium space is defined as the interface compartment between the generator and the lung that includes the patient mask and tubing. In Figure 1C, the aerosol delivery schematic incorporates the nebulizer component with its output activity at a rate, AN′(t), entering the aerosol space consisting of the patient mask, tubing, and reservoir bag plus valves (if present). At time t = 0, an initial activity A0N is introduced into the nebulizer chamber.

Schematic representation of radioisotope inhalation delivery systems. (A) Rebreathing system. (B) Continuous-flow generator output system. (C) Radioaerosol delivery system. Terms are defined in text.
General ConsiderationS
For most nuclear medicine procedures, radioisotopes are introduced into the body as a single, instantaneous administration of activity A0 (either by injection or orally) or as a timed infusion in which the input may be mathematically described as:
 Eq. 1
A′(t) represents the activity infusion rate (in MBq/s), and ta is the time over which the activity is administered. In both cases, a definite, quantifiable activity may be assigned as having entered the body (administered activity). It is recognized that for short administration protocols (ta → 0), A′(t) becomes a delta function and Equation 1 is reduced to case 1, namely Ain = A0.
Eq. 1
A′(t) represents the activity infusion rate (in MBq/s), and ta is the time over which the activity is administered. In both cases, a definite, quantifiable activity may be assigned as having entered the body (administered activity). It is recognized that for short administration protocols (ta → 0), A′(t) becomes a delta function and Equation 1 is reduced to case 1, namely Ain = A0.
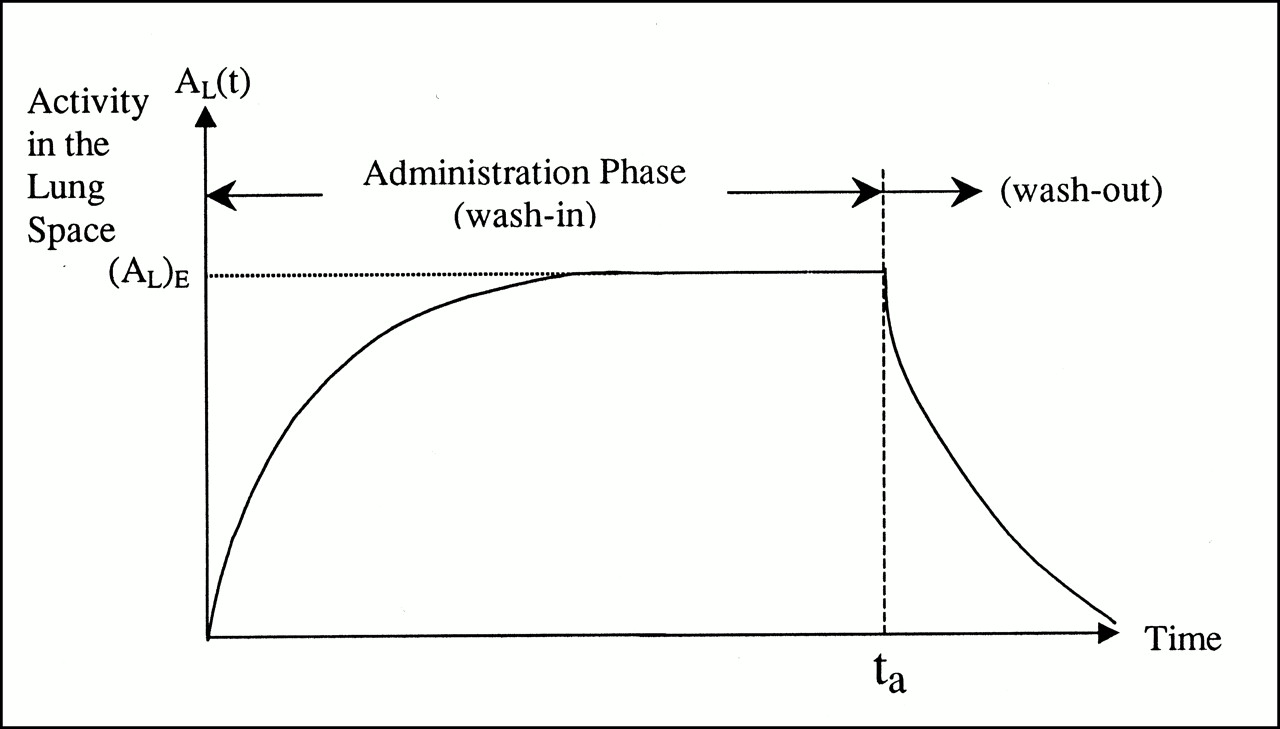
For situations involving ventilation procedures with no initial activity in the lung space, the administration phase is moderated by the inspiration and exhalation patterns that effectuate breathing-promoted mixing. However, it is this mixing process involving exhalation of activity that adds complexity to the definition of administered activity for ventilation studies and underscores the need for a closer examination of the associated concepts. Figure 2 illustrates the activity in the lung space as a function of time, AL(t). The administration phase (wash-in) may be described as a volume-associated change (inspiration volume minus expiration volume) superimposed on an inverse dilution curve representing the mixing of ambient air in the lung with radioactivity (radiosotope gas or radioaerosol). However, in this article, lung activity is modeled more simply as an average value (as shown in Fig. 2) without incorporating the fine mathematic details of changes in inspiration and expiration volume. For the first two methods, after sufficient time, an equilibrium distribution is established in the lung space, (AL)E, in which, for the rebreathing protocol, the activity concentrations (activity per unit volume) in all parts of the system (spirometer and lung space) are equal, and, for the generator technique, the activity concentrations in the virtual equilibrium space and lung space are equal. At time ta, the administration (delivery) phase is terminated. The washout phase after cessation of input involves elimination of activity primarily by exhalation and exhibits a rapid drop-off in the AL(t) curve. However, this washout phase is distinct from the administration phase and does not affect the concept of administered activity for ventilation studies. The discussion below focuses on determination of (AL)E for each of these first two ventilation procedures. However, for the aerosol delivery system, no true equilibrium state is reached over the period of administration. In clinical practice for aerosol inhalation procedures, the activity in a patient’s lungs continues to increase until aerosol concentrations sufficient for the required imaging statistics (typically approximately 37 MBq [1 mCi] delivered to the lung space) are achieved, at which point the administration phase is terminated.

Activity in lung space, AL(t), as function of time. At time ta, administration phase is concluded and washout begins. Activity equilibrium distribution (AL)E is established for rebreathing and generator systems; however, for radioaerosol delivery system, administration is terminated on rising portion of lung activity curve.
Rebreathing-System Protocol (Spirometer/Mouthpiece or Mask)
At equilibrium, activity in the lungs (ignoring physical decay) is given as:
 Eq. 2
with
Eq. 2
with
 Eq. 3
where A0S is the activity introduced into the spirometer, VL is the volume of the lungs (an average between the inspiration and expiration volumes), and VS is the volume of the spirometer. The activity in the lungs as a function of time during the administration phase is:
Eq. 3
where A0S is the activity introduced into the spirometer, VL is the volume of the lungs (an average between the inspiration and expiration volumes), and VS is the volume of the spirometer. The activity in the lungs as a function of time during the administration phase is:
 Eq. 4
where the wash-in rate constant Λ incorporates aspects of mixing or dilution, radioactivity decay, and transport into and out of the rest of the body. Integrating with respect to time (from t = 0 to ta) provides an expression for the lung cumulated activity during the spirometer protocol administration phase or, in the new terminology, lung administered cumulated activity:
Eq. 4
where the wash-in rate constant Λ incorporates aspects of mixing or dilution, radioactivity decay, and transport into and out of the rest of the body. Integrating with respect to time (from t = 0 to ta) provides an expression for the lung cumulated activity during the spirometer protocol administration phase or, in the new terminology, lung administered cumulated activity:
 Eq. 5
Thus, the lung administered cumulated activity represents a specific subcomponent of total lung cumulated activity limited to the period of radioisotope delivery. Equation 5 is identical to Equation 6 in reference 1 for radioxenons with fA0S = AL(∞). By rearranging Equation 5, the lung administered cumulated activity per activity initially introduced into the spirometer may be defined as:
Eq. 5
Thus, the lung administered cumulated activity represents a specific subcomponent of total lung cumulated activity limited to the period of radioisotope delivery. Equation 5 is identical to Equation 6 in reference 1 for radioxenons with fA0S = AL(∞). By rearranging Equation 5, the lung administered cumulated activity per activity initially introduced into the spirometer may be defined as:
 Eq. 6
Eq. 6
Continuous-Flow Generator Output Techniques
The rate of activity output from the continuous-flow generator (Fig. 1B) is taken as constant (A′(t) = A′). For convenience in the model description, a virtual equilibrium space has been defined to accept the output from the generator. The virtual-space physical components are the patient mask and associated connecting tubing. The activity in the lungs as a function of time during the administration phase is given as:
 Eq. 7
The rate constant Λ again incorporates aspects of transport (turnover) into and from the rest of the body, as well as radioactive decay. For situations in which the radioisotope physical half-life, TP (= ln2/λ, where λ is the physical decay constant), is short compared with the administration period, the equilibrium activity is given as:
Eq. 7
The rate constant Λ again incorporates aspects of transport (turnover) into and from the rest of the body, as well as radioactive decay. For situations in which the radioisotope physical half-life, TP (= ln2/λ, where λ is the physical decay constant), is short compared with the administration period, the equilibrium activity is given as:
 Eq. 8
Equation 7 is similar to an equation provided in reference 8 for 8lmKr; however, the equilibrium distribution there is given the symbol E with no rigorous definition.
Eq. 8
Equation 7 is similar to an equation provided in reference 8 for 8lmKr; however, the equilibrium distribution there is given the symbol E with no rigorous definition.
The lung administered cumulated activity for the generator technique (defined similarly to that for the spirometer protocol) is:
 Eq. 9
The lung administered cumulated activity per generator output activity rate may be written as:
Eq. 9
The lung administered cumulated activity per generator output activity rate may be written as:
 Eq. 10
Eq. 10
Radioaerosol Delivery Techniques
At the start of the radioaerosol delivery procedure, an initial activity, A0N, is introduced into the nebulizer chamber in a specified fluid volume (1–5 mL). An air or oxygen flow rate is established (8–10 L/min) to maintain a constant aerosol generation rate, A′G(t), over the period of administration. In practice, the generation rate is nearly constant until the nebulizer dead volume (sputter condition) is reached—generally <1 mL. However, the output may actually rise slightly because of concentrating effects within the nebulizer liquid volume (R. King, Medi-Nuclear Corp., Baldwin Park, CA; oral communication, September 1999). Typically with 99mTc aerosols, the patient may breathe for 3–5 min, with the activity in the lungs increasing over this administration period until adequate imaging statistics are achieved. For a model in which the patient is allowed to breathe indefinitely, the final (equilibrium) activity in the lungs (ignoring physical decay) would be:
 Eq. 11
where g is the fraction of the activity initially placed in the nebulizer (A0N) that would be deposited in the lungs for long (infinite) administration periods. The factor g depends on many variables, including the activity concentration as introduced into the nebulizer; the nebulizer dead volume (sputter) in relationship to the fluid volume introduced into the nebulizer; the activity retained in the tubing, mouthpiece, and mask; the activity trapped in the filter on exhalation (and/or the activity vented); the average particle size; and the patient breathing rate and tidal volume. As such, g is not a parameter that can be derived analytically from (or related directly to) other system parameters, for example, as f was related to VL and VS in Equation 3. Its value depends on the efficiency of the specific nebulizer device along with other factors as listed above, and this value may range from 0.1 to 0.5, with the higher value associated with newer recirculating-system designs.
Eq. 11
where g is the fraction of the activity initially placed in the nebulizer (A0N) that would be deposited in the lungs for long (infinite) administration periods. The factor g depends on many variables, including the activity concentration as introduced into the nebulizer; the nebulizer dead volume (sputter) in relationship to the fluid volume introduced into the nebulizer; the activity retained in the tubing, mouthpiece, and mask; the activity trapped in the filter on exhalation (and/or the activity vented); the average particle size; and the patient breathing rate and tidal volume. As such, g is not a parameter that can be derived analytically from (or related directly to) other system parameters, for example, as f was related to VL and VS in Equation 3. Its value depends on the efficiency of the specific nebulizer device along with other factors as listed above, and this value may range from 0.1 to 0.5, with the higher value associated with newer recirculating-system designs.
The activity in the lungs as a function of time during the administration phase is:
 Eq. 12
As stated previously, the rate constant Λ reflects all aspects of transport into and out of the lung space and includes radioactive decay.
Eq. 12
As stated previously, the rate constant Λ reflects all aspects of transport into and out of the lung space and includes radioactive decay.
The lung administered cumulated activity for the aerosol delivery system (defined in a format similar to that for the other techniques) is:
 Eq. 13
The lung administered cumulated activity per activity initially placed in the nebulizer is then:
Eq. 13
The lung administered cumulated activity per activity initially placed in the nebulizer is then:
 Eq. 14
Eq. 14
DISCUSSION
Rebreathing-System Protocol (Spirometer)
Previous treatments of the rebreathing protocol (e.g., (1)) have normalized the radiation dose to the activity introduced into the spirometer (A0S). Because of spirometer–lung volume mixing as discussed above, this normalization step is not equivalent to using A0, the activity administered to the patient, which has been the traditional normalization factor in dosimetry evaluations. Nevertheless, for comparison of radiation doses for the same spirometer system (or for a standard spirometer volume VS), there may be some validity and rationale for using A0S to normalize the results. However, the preferred approach for estimating the dose would be through direct measurement of AL(t), which incorporates patient-specific aspects of lung volume, inspiration and expiration, and other exit pathways.
Continuous-Flow Generator Output Techniques
Reference 8 presents the data as absorbed dose per activity-minute in the lungs (rad/[mCi · min] or mGy/[mBq · min]) with an equilibrium value of 37 MBq (1 mCi) in the lung spaces. Thus, the normalization is in units of cumulated activity, although this concept was not discussed directly in this report.
Radioaerosol Delivery Techniques
Reference 12 presents the data as absorbed dose per unit administered activity. The assumption is made that 37 MBq (1 mCi) have been delivered to the lung alveoli (in a specific aerosol volume) over the administration period.
Mean Administered Activity for Ventilation Procedures
Another potentially useful parameter is the mean administered activity for ventilation procedures:
 Eq. 15
As defined, this parameter normalizes the administered cumulated activity in the lung over the administered period and may serve to standardize descriptions of the protocols between patients or institutions.
Eq. 15
As defined, this parameter normalizes the administered cumulated activity in the lung over the administered period and may serve to standardize descriptions of the protocols between patients or institutions.
CONCLUSION
The analytic models presented may be employed to evaluate the lung administered cumulated activity for ventilation studies as a function of explicit variables encountered in clinical protocols, including, for example, spirometer volume, generator activity output rate, lung wash-in half-time, and administration time. Standardization of the calculational approach used to estimate the radiation dose may be achieved through use of the new parameter, lung administered cumulated activity. It is recommended that dose estimate reports be based on measurements of cumulated activity in the lung over the administration period and normalized to this administered cumulated activity. The term “administered activity” should not be associated with MBq · min (or mCi · min), as is the current practice in certain situations.
Examples
Rebreathing-System Protocol (Spirometer/Mouthpiece or Mask)
The spirometer ventilation protocol commonly specifies a 5-min breathing period (administration phase or wash-in) during which equilibrium is established (Fig. 2). For 133Xe, the activity A0S may range from 185 to 925 MBq (5–25 mCi), with a typical value of 370 MBq (10 mCi) introduced into a total spirometer volume (VS) of 5–10 L. In reference 1, dosimetry was evaluated under a model with VS values of 5, 7.5, and 10 L. Other investigators have provided data for ventilation studies showing average patient lung volumes that range from 1.9 to 5.2 L (3.9 ± 1.1 L; population, n = 13 [8 male, 5 female]) (2). The wash-in rate constant Λ depends on both the spirometer and the lung volumes. For the model described in reference 1, Λ values ranged from approximately 2.4 to 2.9 per minute (144–173 per hour), corresponding to a wash-in half-time (T1/2)wash-in of ∼0.29 to 0.24 min. However, in other studies, wash-in half-times up to nearly 2 min have been observed for specific patients, with an average approximately 0.65 ± 0.5 min (3).
Examples of lung administered cumulated activity per initial spirometer activity, (ÃL(0,ta))S/A0S, are provided in Figure 3 using the model parameter values shown in Table 1. The lung administered cumulated activity per initial spirometer activity as a function of wash-in half-time is presented for the rebreathing ventilation procedure according to Equation 6. The data include a family of curves for values of the ratio f corresponding to VS values of 5 and 10 L and VL values of 2.5 and 4.0 L (Table 1). For a (T1/2)wash-in as long as 2 min, conditions fall slightly short of achieving full equilibrium for the 5-min administration phase, with the level reached being ∼82% of maximum. However, for (T1/2)wash-in of 0.5 and 1.0 min, the values achieved are 99.9% and ∼97%, respectively.

Example of rebreathing ventilation protocol shows lung administered cumulated activity per initial spirometer activity as function of wash-in half-time for ta = 5 min.
Model Parameters Used in Lung Administered Cumulated Activity Examples
As shown in Figure 3 (and as expected according to Eq. 6), as the spirometer volume increases, the administered cumulated activity per initial spirometer activity decreases, whereas conversely, as the lung volume gets larger, the ÃL/A0S value increases. In general, as the wash-in half-time increases, ÃL/A0S decreases. If the wash-in uptakes were instantaneous ([T1/2]wash-in = 0), the ÃL/A0S intercept values given by f ta would range from 1 to 2.22 min for ta = 5 min and f = 0.20 and 0.44, respectively. In the specific example for administration of A0S = 370 MBq (10 mCi) and f = 0.2, ta = 5 min, and (T1/2)wash-in = 0.5 min, the lung administered cumulated activity ÃL(0,5) = 318.2 MBq · min (8.6 mCi · min), and the mean administered activity for ventilation 〈(AL)0V〉 = 63.6 MBq (1.72 mCi) (from Eq. 15).
Continuous-Flow Generator Output Techniques
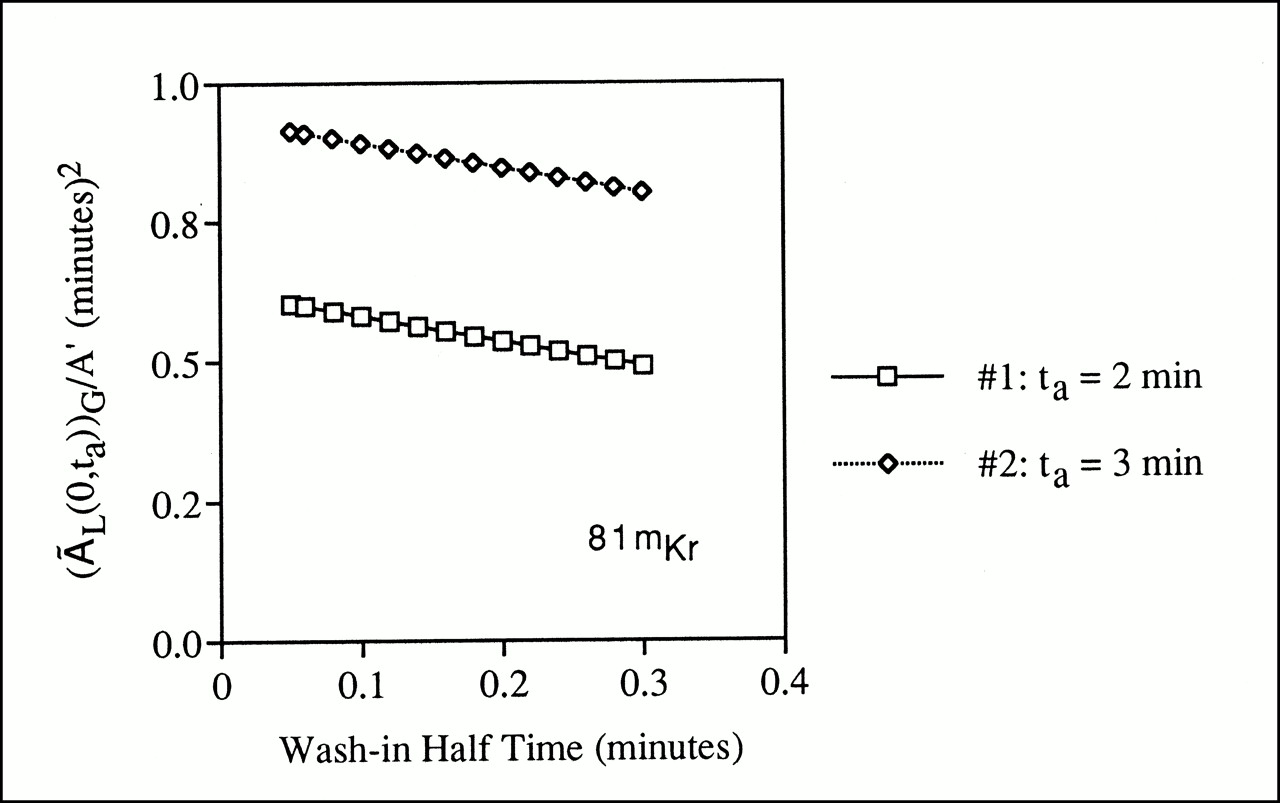
For ventilation studies using an 81Rb/81mKr generator with a typical output activity flow rate of 185–1850 MBq/min (5–50 mCi/min), lung equilibrium is established rapidly, in less than 30 s (5), with the inhalation (administration phase) usually continued for 2–3 min (2). For 81mKr with a short physical half-life of 13 s, the equilibrium activity value will be taken as (AL)E = A′/λ according to Equation 8, although the requirement that λt ≫ 1 is only marginally satisfied over a period ta = 2 min. For this example, (T1/2)wash-in has been taken to range from 0.05 to 0.3 min (Table 1). Figure 4 presents the lung administrated cumulated activity per generator activity output rate for 81mKr. The values increase with increasing length of the administration period ta and fall off with increasing wash-in half-times as calculated from Equation 10. For a specific example with an A′ = 740 MBq/min (20 mCi/min), ta = 2 min, and (T1/2)wash-in = 0.1 min, the lung administered cumulated activity ÃL(0,2) = 429.2 MBq · min (11.6 mCi · min), and the mean administered activity for ventilation 〈(AL)0V〉 = 214.6 MBq (5.8 mCi).

Example of generator ventilation technique shows lung administered cumulated activity per generator activity output rate as function of wash-in half-time.
Radioaerosol Delivery Techniques
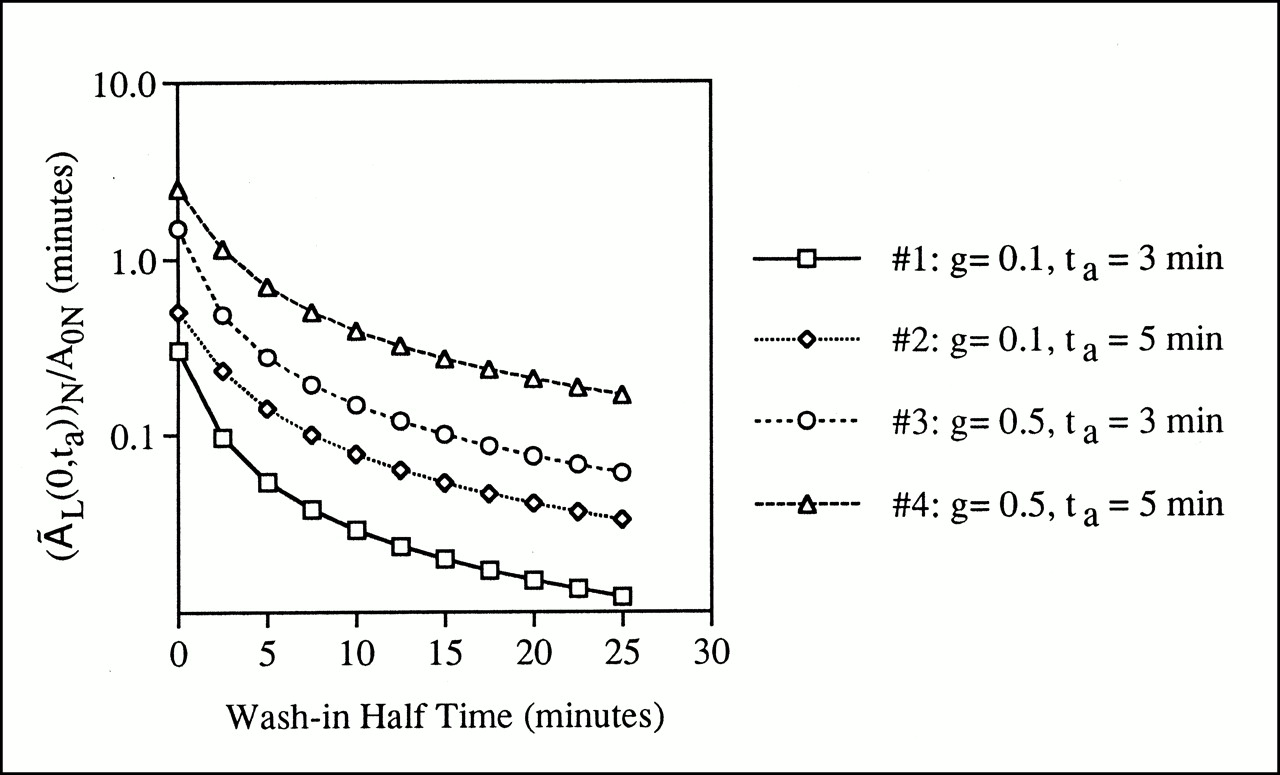
For ventilation studies using 99mTc–diethylenetriaminepentaacetic acid aerosols, the initial activity introduced into the nebulizer (A0N) may be 1110–2220 MBq (30–60 mCi) in a volume of 1–5 mL. Depending on the style of the nebulizer system and the air flow rate, the aerosol generation rate might range from 0.1 to 0.3 mL/min. The particle diameter is maintained at or below ∼1 μm. In general, standard nebulizer systems are relatively inefficient, with only 10%–15% of the radioaerosol being deposited in the lung space. In a typical clinical study, the patient breathes the radioaerosol for 3–5 min, with the inhalation phase being terminated when sufficient imaging count statistics have been achieved. Approximately 37 MBq (1 mCi) may be introduced into the lung at this point with no equilibrium established. For this example, (T1/2)wash-in has been taken to range from 2.5 to 25 min (Table 1), which reflects the relatively slow aerosol generation and deposition mechanisms. As indicated in Figure 5 (and as expected from Eq. 14), the administered cumulated activity per initial nebulizer activity increases as both the fraction g and the administration time increase. The fall-off in the administered cumulated activity with increasing wash-in half-time is relatively rapid for values out to 10 min. In a specific example, given A0N = 1850 MBq (50 mCi), g = 0.1, ta = 3 min, and (T1/2)wash-in = 10 min, the lung administered cumulated activity ÃL(0,10) = 54 MBq · min (1.46 mCi · min) and the mean administered activity for ventilation 〈(AL)0V〉 = 18.1 MBq (0.49 mCi).
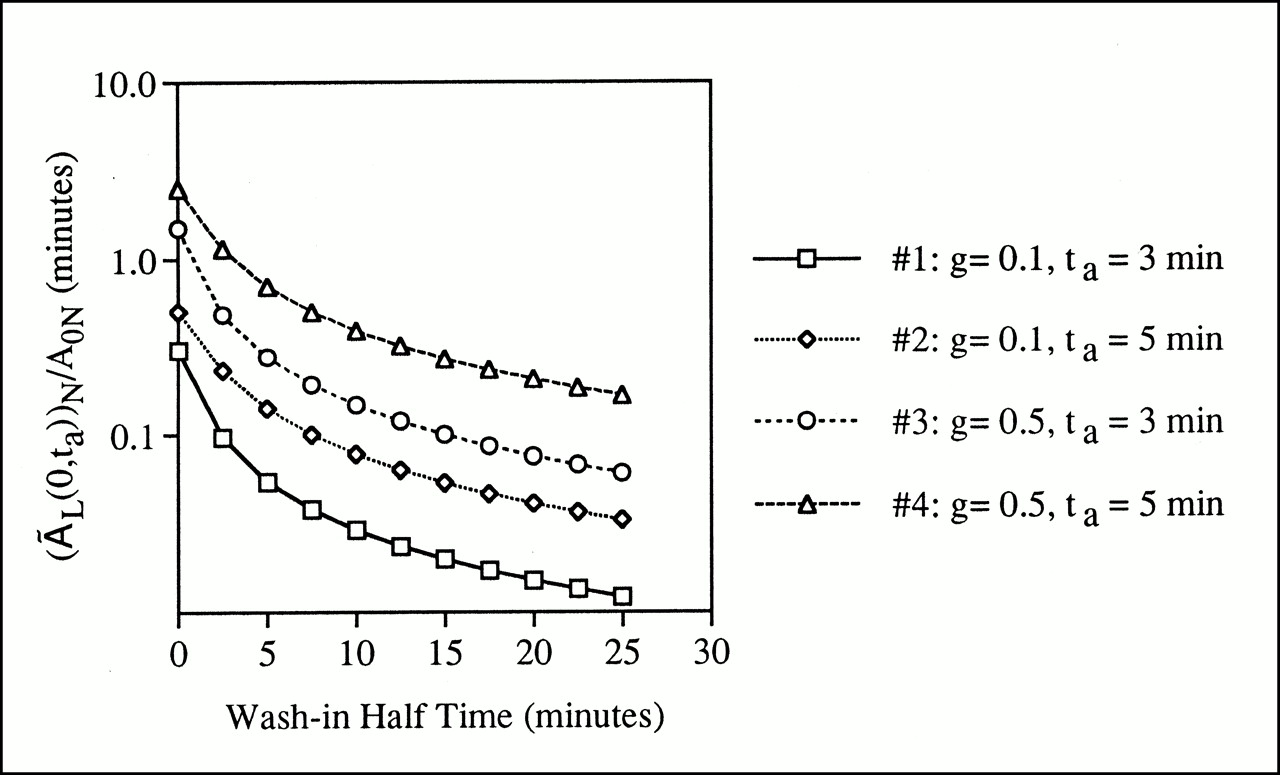
Example of radioaerosol ventilation technique shows lung administered cumulated activity per initial nebulizer activity as function of wash-in half-time.
Footnotes
Received Jun. 13, 2000; revision accepted Nov. 10, 2000.
For correspondence or reprints contact: Stephen R. Thomas, PhD, 6167 Medical Sciences Bldg., College of Medicine, University of Cincinnati, 231 Bethesda Ave., Cincinnati, OH 45267-0579.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.